User login
Leadership Academy 2016 heads to Florida in October
Ever wish you had more leadership training in medical school or your residency programs? Feel a bit overwhelmed when developing operational plans for your hospital or negotiating important contracts? Join SHM in sunny Lake Buena Vista, Fla., October 24–27, for its esteemed Leadership Academy (www.shmleadershipacademy.org). SHM Leadership Academy prepares clinicians, academicians, and administrators with vital leadership skills traditionally not taught throughout the course of medical training, tailored specifically to hospital medicine.
“SHM’s Leadership Academy teaches leadership skills for individuals all across the spectrum of the hospital team. My experience helped me to raise the bar not only to benefit myself but also my institution and especially my patients,” says Ron Greeno, MD, MHM. “I highly recommend this experience to any hospital medicine professionals who aspire to take their leadership skills to the next level.”
All three courses run concurrently over the span of the four days and are led by world-renowned faculty. This expanded meeting will provide attendees with unprecedented networking opportunities with hundreds of colleagues and enhanced career development.
Available Leadership Academy courses include:
- Leadership Foundations, a four-day course that serves as the first step in your leadership journey. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and much more. Attendees are divided into smaller moderated groups to ensure meaningful, relevant application of concepts to hands-on activities.
- Advanced Leadership: Influential Management, a course that builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more through world-renowned faculty and applied exercises.
(Prerequisite: Leadership Foundations or an advanced management degree upon course director approval)
- Advanced Leadership: Mastering Teamwork, a course developed in response to high demand from previous Leadership Academy attendees. Participants learn how to critically assess program growth opportunities and develop operational plans; utilize the principles of SWARM intelligence; lead, manage, and motivate teams in complex hospital environments; and develop effective communication strategies.
(Prerequisite: Leadership Foundations or an advanced management degree upon course director approval.)
SHM members receive reduced rates for course tuition. For more information on how to register, visit www.SHMLeadershipAcademy.org.
Ever wish you had more leadership training in medical school or your residency programs? Feel a bit overwhelmed when developing operational plans for your hospital or negotiating important contracts? Join SHM in sunny Lake Buena Vista, Fla., October 24–27, for its esteemed Leadership Academy (www.shmleadershipacademy.org). SHM Leadership Academy prepares clinicians, academicians, and administrators with vital leadership skills traditionally not taught throughout the course of medical training, tailored specifically to hospital medicine.
“SHM’s Leadership Academy teaches leadership skills for individuals all across the spectrum of the hospital team. My experience helped me to raise the bar not only to benefit myself but also my institution and especially my patients,” says Ron Greeno, MD, MHM. “I highly recommend this experience to any hospital medicine professionals who aspire to take their leadership skills to the next level.”
All three courses run concurrently over the span of the four days and are led by world-renowned faculty. This expanded meeting will provide attendees with unprecedented networking opportunities with hundreds of colleagues and enhanced career development.
Available Leadership Academy courses include:
- Leadership Foundations, a four-day course that serves as the first step in your leadership journey. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and much more. Attendees are divided into smaller moderated groups to ensure meaningful, relevant application of concepts to hands-on activities.
- Advanced Leadership: Influential Management, a course that builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more through world-renowned faculty and applied exercises.
(Prerequisite: Leadership Foundations or an advanced management degree upon course director approval)
- Advanced Leadership: Mastering Teamwork, a course developed in response to high demand from previous Leadership Academy attendees. Participants learn how to critically assess program growth opportunities and develop operational plans; utilize the principles of SWARM intelligence; lead, manage, and motivate teams in complex hospital environments; and develop effective communication strategies.
(Prerequisite: Leadership Foundations or an advanced management degree upon course director approval.)
SHM members receive reduced rates for course tuition. For more information on how to register, visit www.SHMLeadershipAcademy.org.
Ever wish you had more leadership training in medical school or your residency programs? Feel a bit overwhelmed when developing operational plans for your hospital or negotiating important contracts? Join SHM in sunny Lake Buena Vista, Fla., October 24–27, for its esteemed Leadership Academy (www.shmleadershipacademy.org). SHM Leadership Academy prepares clinicians, academicians, and administrators with vital leadership skills traditionally not taught throughout the course of medical training, tailored specifically to hospital medicine.
“SHM’s Leadership Academy teaches leadership skills for individuals all across the spectrum of the hospital team. My experience helped me to raise the bar not only to benefit myself but also my institution and especially my patients,” says Ron Greeno, MD, MHM. “I highly recommend this experience to any hospital medicine professionals who aspire to take their leadership skills to the next level.”
All three courses run concurrently over the span of the four days and are led by world-renowned faculty. This expanded meeting will provide attendees with unprecedented networking opportunities with hundreds of colleagues and enhanced career development.
Available Leadership Academy courses include:
- Leadership Foundations, a four-day course that serves as the first step in your leadership journey. Attendees learn how to evaluate personal leadership strengths and weaknesses, create and execute a communication strategy for key team members, understand key hospital drivers, examine how hospital metrics are derived, and much more. Attendees are divided into smaller moderated groups to ensure meaningful, relevant application of concepts to hands-on activities.
- Advanced Leadership: Influential Management, a course that builds skills around driving culture change through specific leadership behaviors and actions, financial storytelling, engaging in effective professional negotiation activities with proven techniques, and more through world-renowned faculty and applied exercises.
(Prerequisite: Leadership Foundations or an advanced management degree upon course director approval)
- Advanced Leadership: Mastering Teamwork, a course developed in response to high demand from previous Leadership Academy attendees. Participants learn how to critically assess program growth opportunities and develop operational plans; utilize the principles of SWARM intelligence; lead, manage, and motivate teams in complex hospital environments; and develop effective communication strategies.
(Prerequisite: Leadership Foundations or an advanced management degree upon course director approval.)
SHM members receive reduced rates for course tuition. For more information on how to register, visit www.SHMLeadershipAcademy.org.
Researchers Say Procalcitonin is Linked to Shorter Treatment and Reduced Mortality in Critically Ill
NEW YORK (Reuters Health) - Use of the marker procalcitonin to guide antibacterial therapy in the critically ill is associated with shorter treatment and reduced mortality, according to Dutch researchers.
As Dr. Evelien de Jong told Reuters Health by email, "Antibiotic overconsumption is one of the largest threats to medicine in the near future. Our study is the largest randomized controlled trial of antibiotic reduction in intensive care units (ICUs) and will, hopefully, contribute to a more individualized antibiotic duration per patient and an overall reduction of antibiotic use."
In a February 29 online paper in the Lancet Infectious Diseases, Dr. de Jong, of VU University Medical Center, Amsterdam, and colleagues noted that a "drop in procalcitonin concentration might help (clinicians) to discontinue antibiotic use in a more timely fashion" than reliance on biomarkers such as C-reactive protein.
To investigate, the researchers studied 1,575 ICU patients who received antibiotics and were randomized to procalcitonin-guided antibiotic discontinuation or standard of care. Fifteen were excluded from the procalcitonin group and 14 were excluded from the standard care group.
"In the procalcitonin-guided group, a non-binding advice to discontinue antibiotics was provided if procalcitonin concentration had decreased by 80% or more of its peak value or to 0.5 ug/L or lower," the authors reported.
In all, 538 (71%) of 761 patients in the procalcitonin-guided group and 457 (58%) of 785 patients in the standard-of-care group completed their antibiotic treatment in the ICU.
Median consumption of antibiotics was 7.5 daily defined doses in the procalcitonin group, significantly less than the 9.3 daily defined doses in the standard-of-care group, for a mean group absolute difference of 2.69 (p<0.0001).
Median duration of treatment was also significantly shorter in the procalcitonin-guided group (five versus seven days), for a mean group absolute difference of 1.22 (p<0.0001).
Mortality at 28 days was also significantly less than in the standard-of-care group. This was 20% versus 27% in intention-to-treat analysis. At one year, corresponding per protocol proportions were 36% and 43%.
Overall, the researchers concluded, "Procalcitonin concentrations might help physicians in deciding whether or not the presumed infection is truly bacterial, leading to more adequate diagnosis and treatment, the cornerstones of antibiotic stewardship."
Commenting by email, Dr. Philipp Schuetz, coauthor of an accompanying editorial, told Reuters Health, "This well-done and large landmark trial proves that procalcitonin-guided care reduces unnecessary antibiotic courses in critical care patients with assumed or proven infection and thereby improves patient outcomes, namely overall survival."
Dr. Schuetz, of the University of Basel, Switzerland, concluded, "We should now adapt our guidelines and start to (adopt) more widespread use of procalcitonin protocols in clinical practice to slow emergence of bacterial resistance and improve sepsis care."
NEW YORK (Reuters Health) - Use of the marker procalcitonin to guide antibacterial therapy in the critically ill is associated with shorter treatment and reduced mortality, according to Dutch researchers.
As Dr. Evelien de Jong told Reuters Health by email, "Antibiotic overconsumption is one of the largest threats to medicine in the near future. Our study is the largest randomized controlled trial of antibiotic reduction in intensive care units (ICUs) and will, hopefully, contribute to a more individualized antibiotic duration per patient and an overall reduction of antibiotic use."
In a February 29 online paper in the Lancet Infectious Diseases, Dr. de Jong, of VU University Medical Center, Amsterdam, and colleagues noted that a "drop in procalcitonin concentration might help (clinicians) to discontinue antibiotic use in a more timely fashion" than reliance on biomarkers such as C-reactive protein.
To investigate, the researchers studied 1,575 ICU patients who received antibiotics and were randomized to procalcitonin-guided antibiotic discontinuation or standard of care. Fifteen were excluded from the procalcitonin group and 14 were excluded from the standard care group.
"In the procalcitonin-guided group, a non-binding advice to discontinue antibiotics was provided if procalcitonin concentration had decreased by 80% or more of its peak value or to 0.5 ug/L or lower," the authors reported.
In all, 538 (71%) of 761 patients in the procalcitonin-guided group and 457 (58%) of 785 patients in the standard-of-care group completed their antibiotic treatment in the ICU.
Median consumption of antibiotics was 7.5 daily defined doses in the procalcitonin group, significantly less than the 9.3 daily defined doses in the standard-of-care group, for a mean group absolute difference of 2.69 (p<0.0001).
Median duration of treatment was also significantly shorter in the procalcitonin-guided group (five versus seven days), for a mean group absolute difference of 1.22 (p<0.0001).
Mortality at 28 days was also significantly less than in the standard-of-care group. This was 20% versus 27% in intention-to-treat analysis. At one year, corresponding per protocol proportions were 36% and 43%.
Overall, the researchers concluded, "Procalcitonin concentrations might help physicians in deciding whether or not the presumed infection is truly bacterial, leading to more adequate diagnosis and treatment, the cornerstones of antibiotic stewardship."
Commenting by email, Dr. Philipp Schuetz, coauthor of an accompanying editorial, told Reuters Health, "This well-done and large landmark trial proves that procalcitonin-guided care reduces unnecessary antibiotic courses in critical care patients with assumed or proven infection and thereby improves patient outcomes, namely overall survival."
Dr. Schuetz, of the University of Basel, Switzerland, concluded, "We should now adapt our guidelines and start to (adopt) more widespread use of procalcitonin protocols in clinical practice to slow emergence of bacterial resistance and improve sepsis care."
NEW YORK (Reuters Health) - Use of the marker procalcitonin to guide antibacterial therapy in the critically ill is associated with shorter treatment and reduced mortality, according to Dutch researchers.
As Dr. Evelien de Jong told Reuters Health by email, "Antibiotic overconsumption is one of the largest threats to medicine in the near future. Our study is the largest randomized controlled trial of antibiotic reduction in intensive care units (ICUs) and will, hopefully, contribute to a more individualized antibiotic duration per patient and an overall reduction of antibiotic use."
In a February 29 online paper in the Lancet Infectious Diseases, Dr. de Jong, of VU University Medical Center, Amsterdam, and colleagues noted that a "drop in procalcitonin concentration might help (clinicians) to discontinue antibiotic use in a more timely fashion" than reliance on biomarkers such as C-reactive protein.
To investigate, the researchers studied 1,575 ICU patients who received antibiotics and were randomized to procalcitonin-guided antibiotic discontinuation or standard of care. Fifteen were excluded from the procalcitonin group and 14 were excluded from the standard care group.
"In the procalcitonin-guided group, a non-binding advice to discontinue antibiotics was provided if procalcitonin concentration had decreased by 80% or more of its peak value or to 0.5 ug/L or lower," the authors reported.
In all, 538 (71%) of 761 patients in the procalcitonin-guided group and 457 (58%) of 785 patients in the standard-of-care group completed their antibiotic treatment in the ICU.
Median consumption of antibiotics was 7.5 daily defined doses in the procalcitonin group, significantly less than the 9.3 daily defined doses in the standard-of-care group, for a mean group absolute difference of 2.69 (p<0.0001).
Median duration of treatment was also significantly shorter in the procalcitonin-guided group (five versus seven days), for a mean group absolute difference of 1.22 (p<0.0001).
Mortality at 28 days was also significantly less than in the standard-of-care group. This was 20% versus 27% in intention-to-treat analysis. At one year, corresponding per protocol proportions were 36% and 43%.
Overall, the researchers concluded, "Procalcitonin concentrations might help physicians in deciding whether or not the presumed infection is truly bacterial, leading to more adequate diagnosis and treatment, the cornerstones of antibiotic stewardship."
Commenting by email, Dr. Philipp Schuetz, coauthor of an accompanying editorial, told Reuters Health, "This well-done and large landmark trial proves that procalcitonin-guided care reduces unnecessary antibiotic courses in critical care patients with assumed or proven infection and thereby improves patient outcomes, namely overall survival."
Dr. Schuetz, of the University of Basel, Switzerland, concluded, "We should now adapt our guidelines and start to (adopt) more widespread use of procalcitonin protocols in clinical practice to slow emergence of bacterial resistance and improve sepsis care."
Increasing metabolite levels may prevent GVHD

Photo by Aaron Logan
Increasing levels of a gut microbiome-derived metabolite could help prevent graft-versus-host disease (GVHD) after hematopoietic stem cell transplant (HSCT), according to preclinical research published in Nature Immunology.
For this study, researchers searched for alterations in the gut microbiome to see whether metabolites could impact outcomes after HSCT.
They found that levels of a metabolite called butyrate were significantly reduced in the intestinal tract of mice that received a transplant.
When the researchers increased butyrate levels in these mice, they saw a decrease in the incidence and severity of GVHD.
“Our findings suggest we can prevent graft-vs-host disease by bolstering the amount of the microbiome-derived metabolite butyrate,” said study author Pavan Reddy, MD, of the University of Michigan Comprehensive Cancer Center in Ann Arbor.
He and his colleagues found they could mitigate GVHD by administering butyrate to mice or by altering the composition of indigenous gastrointestinal microbiota so they produced high levels of butyrate.
The team noted that diet is another way to control butyrate production by the gut microbiome—specifically, through resistant starch such as that found in potatoes.
The researchers hope to begin a clinical trial later this year in which they will combine resistant starch with current methods of preventing GVHD to assess whether they can increase butyrate and reduce the incidence and severity of GVHD in HSCT recipients.
“This is a whole new approach,” Dr Reddy said. “The idea is to make the host cells stronger, to be able to withstand the assault of the donor immune cells while reducing the risk of infection or [disease] relapse.” ![]()
Photo by Aaron Logan
Increasing levels of a gut microbiome-derived metabolite could help prevent graft-versus-host disease (GVHD) after hematopoietic stem cell transplant (HSCT), according to preclinical research published in Nature Immunology.
For this study, researchers searched for alterations in the gut microbiome to see whether metabolites could impact outcomes after HSCT.
They found that levels of a metabolite called butyrate were significantly reduced in the intestinal tract of mice that received a transplant.
When the researchers increased butyrate levels in these mice, they saw a decrease in the incidence and severity of GVHD.
“Our findings suggest we can prevent graft-vs-host disease by bolstering the amount of the microbiome-derived metabolite butyrate,” said study author Pavan Reddy, MD, of the University of Michigan Comprehensive Cancer Center in Ann Arbor.
He and his colleagues found they could mitigate GVHD by administering butyrate to mice or by altering the composition of indigenous gastrointestinal microbiota so they produced high levels of butyrate.
The team noted that diet is another way to control butyrate production by the gut microbiome—specifically, through resistant starch such as that found in potatoes.
The researchers hope to begin a clinical trial later this year in which they will combine resistant starch with current methods of preventing GVHD to assess whether they can increase butyrate and reduce the incidence and severity of GVHD in HSCT recipients.
“This is a whole new approach,” Dr Reddy said. “The idea is to make the host cells stronger, to be able to withstand the assault of the donor immune cells while reducing the risk of infection or [disease] relapse.” ![]()
Photo by Aaron Logan
Increasing levels of a gut microbiome-derived metabolite could help prevent graft-versus-host disease (GVHD) after hematopoietic stem cell transplant (HSCT), according to preclinical research published in Nature Immunology.
For this study, researchers searched for alterations in the gut microbiome to see whether metabolites could impact outcomes after HSCT.
They found that levels of a metabolite called butyrate were significantly reduced in the intestinal tract of mice that received a transplant.
When the researchers increased butyrate levels in these mice, they saw a decrease in the incidence and severity of GVHD.
“Our findings suggest we can prevent graft-vs-host disease by bolstering the amount of the microbiome-derived metabolite butyrate,” said study author Pavan Reddy, MD, of the University of Michigan Comprehensive Cancer Center in Ann Arbor.
He and his colleagues found they could mitigate GVHD by administering butyrate to mice or by altering the composition of indigenous gastrointestinal microbiota so they produced high levels of butyrate.
The team noted that diet is another way to control butyrate production by the gut microbiome—specifically, through resistant starch such as that found in potatoes.
The researchers hope to begin a clinical trial later this year in which they will combine resistant starch with current methods of preventing GVHD to assess whether they can increase butyrate and reduce the incidence and severity of GVHD in HSCT recipients.
“This is a whole new approach,” Dr Reddy said. “The idea is to make the host cells stronger, to be able to withstand the assault of the donor immune cells while reducing the risk of infection or [disease] relapse.” ![]()
EMA recommends safety measures for idelalisib

Photo courtesy of
Gilead Sciences, Inc.
In light of recently reported safety concerns, the European Medicines Agency’s (EMA) Pharmacovigilance Risk Assessment Committee (PRAC) has issued provisional advice for doctors and patients using idelalisib (Zydelig).
The EMA recently began reviewing the safety of idelalisib because of serious adverse events, most of which were infection-related, that were reported in 3 clinical trials investigating idelalisib in combination with other drugs.
These trials have since been stopped.
Now, the PRAC is making provisional recommendations to ensure idelalisib is used as safely as possible outside of clinical trials.
These recommendations will be forwarded to the European Commission, which will issue a provisional legally binding decision applicable in all European Union (EU) member states.
In the EU, idelalisib is approved as monotherapy for adults with follicular lymphoma that is refractory to 2 prior lines of treatment.
Idelalisib is also approved for use in combination with rituximab to treat adults with chronic lymphocytic leukemia (CLL) who have received at least 1 prior therapy or as first-line treatment in the presence of 17p deletion or TP53 mutation in CLL patients considered unsuitable for chemo-immunotherapy.
Recommendations
The PRAC is recommending that previously untreated CLL patients with 17p deletion or TP53 mutation do not begin treatment with idelalisib. In addition, doctors should re-evaluate each patient taking idelalisib as first-line treatment for CLL and only continue treatment if the benefits outweigh the risks.
Idelalisib can continue to be used in combination, only with rituximab, in CLL patients who have received at least 1 prior therapy and as monotherapy in patients with follicular lymphoma that is refractory to 2 lines of treatment.
Patients with any evidence of ongoing systemic infection should not be started on treatment with idelalisib.
And patients should be informed about the risk of serious infections with idelalisib.
All patients who do receive idelalisib should take antibiotics to prevent Pneumocystis jirovecii pneumonia, and they should be monitored for respiratory signs and symptoms. Regular clinical and laboratory monitoring for cytomegalovirus infection is also recommended.
Patients should have regular blood tests to detect neutropenia. In case a patient has moderate or severe neutropenia, treatment with idelalisib may have to be interrupted, in line with the updated summary of product characteristics.
The EMA said further details on these provisional measures will be provided in writing to healthcare professionals, and the product information will be updated accordingly.
Likewise, further information on the review of idelalisib will be provided as necessary and once the review is finished.
About the review
The EMA’s review of idelalisib started after a higher rate of serious adverse events, including deaths, was seen in 3 clinical trials evaluating the addition of idelalisib to standard therapy in first-line CLL and relapsed indolent non-Hodgkin lymphoma (NHL).
Most of the deaths were related to infections such as Pneumocystis jirovecii pneumonia and cytomegalovirus infection. Other excess deaths were related mainly to respiratory events.
The NHL studies (NCT01732926 and NCT01732913) included patients with disease characteristics different from those covered by the currently approved indication for idelalisib and investigated combinations of drugs that are not currently approved in the EU—idelalisib plus rituximab for NHL and idelalisib plus bendamustine and rituximab for NHL.
The CLL trial (NCT01980888) involved patients who had not received previous treatment, some of whom had the 17p deletion or TP53 mutation. However, the trial also investigated a combination of drugs not currently approved in the EU—idelalisib plus bendamustine and rituximab.
At present, the PRAC is conducting the review. Once the PRAC is finished, its recommendations will be forwarded to the EMA’s Committee for Medicinal Products for Human Use, which will adopt a final opinion.
The European Commission will take this opinion into account and adopt a legally binding decision that is applicable in all EU member states. ![]()
Photo courtesy of
Gilead Sciences, Inc.
In light of recently reported safety concerns, the European Medicines Agency’s (EMA) Pharmacovigilance Risk Assessment Committee (PRAC) has issued provisional advice for doctors and patients using idelalisib (Zydelig).
The EMA recently began reviewing the safety of idelalisib because of serious adverse events, most of which were infection-related, that were reported in 3 clinical trials investigating idelalisib in combination with other drugs.
These trials have since been stopped.
Now, the PRAC is making provisional recommendations to ensure idelalisib is used as safely as possible outside of clinical trials.
These recommendations will be forwarded to the European Commission, which will issue a provisional legally binding decision applicable in all European Union (EU) member states.
In the EU, idelalisib is approved as monotherapy for adults with follicular lymphoma that is refractory to 2 prior lines of treatment.
Idelalisib is also approved for use in combination with rituximab to treat adults with chronic lymphocytic leukemia (CLL) who have received at least 1 prior therapy or as first-line treatment in the presence of 17p deletion or TP53 mutation in CLL patients considered unsuitable for chemo-immunotherapy.
Recommendations
The PRAC is recommending that previously untreated CLL patients with 17p deletion or TP53 mutation do not begin treatment with idelalisib. In addition, doctors should re-evaluate each patient taking idelalisib as first-line treatment for CLL and only continue treatment if the benefits outweigh the risks.
Idelalisib can continue to be used in combination, only with rituximab, in CLL patients who have received at least 1 prior therapy and as monotherapy in patients with follicular lymphoma that is refractory to 2 lines of treatment.
Patients with any evidence of ongoing systemic infection should not be started on treatment with idelalisib.
And patients should be informed about the risk of serious infections with idelalisib.
All patients who do receive idelalisib should take antibiotics to prevent Pneumocystis jirovecii pneumonia, and they should be monitored for respiratory signs and symptoms. Regular clinical and laboratory monitoring for cytomegalovirus infection is also recommended.
Patients should have regular blood tests to detect neutropenia. In case a patient has moderate or severe neutropenia, treatment with idelalisib may have to be interrupted, in line with the updated summary of product characteristics.
The EMA said further details on these provisional measures will be provided in writing to healthcare professionals, and the product information will be updated accordingly.
Likewise, further information on the review of idelalisib will be provided as necessary and once the review is finished.
About the review
The EMA’s review of idelalisib started after a higher rate of serious adverse events, including deaths, was seen in 3 clinical trials evaluating the addition of idelalisib to standard therapy in first-line CLL and relapsed indolent non-Hodgkin lymphoma (NHL).
Most of the deaths were related to infections such as Pneumocystis jirovecii pneumonia and cytomegalovirus infection. Other excess deaths were related mainly to respiratory events.
The NHL studies (NCT01732926 and NCT01732913) included patients with disease characteristics different from those covered by the currently approved indication for idelalisib and investigated combinations of drugs that are not currently approved in the EU—idelalisib plus rituximab for NHL and idelalisib plus bendamustine and rituximab for NHL.
The CLL trial (NCT01980888) involved patients who had not received previous treatment, some of whom had the 17p deletion or TP53 mutation. However, the trial also investigated a combination of drugs not currently approved in the EU—idelalisib plus bendamustine and rituximab.
At present, the PRAC is conducting the review. Once the PRAC is finished, its recommendations will be forwarded to the EMA’s Committee for Medicinal Products for Human Use, which will adopt a final opinion.
The European Commission will take this opinion into account and adopt a legally binding decision that is applicable in all EU member states. ![]()
Photo courtesy of
Gilead Sciences, Inc.
In light of recently reported safety concerns, the European Medicines Agency’s (EMA) Pharmacovigilance Risk Assessment Committee (PRAC) has issued provisional advice for doctors and patients using idelalisib (Zydelig).
The EMA recently began reviewing the safety of idelalisib because of serious adverse events, most of which were infection-related, that were reported in 3 clinical trials investigating idelalisib in combination with other drugs.
These trials have since been stopped.
Now, the PRAC is making provisional recommendations to ensure idelalisib is used as safely as possible outside of clinical trials.
These recommendations will be forwarded to the European Commission, which will issue a provisional legally binding decision applicable in all European Union (EU) member states.
In the EU, idelalisib is approved as monotherapy for adults with follicular lymphoma that is refractory to 2 prior lines of treatment.
Idelalisib is also approved for use in combination with rituximab to treat adults with chronic lymphocytic leukemia (CLL) who have received at least 1 prior therapy or as first-line treatment in the presence of 17p deletion or TP53 mutation in CLL patients considered unsuitable for chemo-immunotherapy.
Recommendations
The PRAC is recommending that previously untreated CLL patients with 17p deletion or TP53 mutation do not begin treatment with idelalisib. In addition, doctors should re-evaluate each patient taking idelalisib as first-line treatment for CLL and only continue treatment if the benefits outweigh the risks.
Idelalisib can continue to be used in combination, only with rituximab, in CLL patients who have received at least 1 prior therapy and as monotherapy in patients with follicular lymphoma that is refractory to 2 lines of treatment.
Patients with any evidence of ongoing systemic infection should not be started on treatment with idelalisib.
And patients should be informed about the risk of serious infections with idelalisib.
All patients who do receive idelalisib should take antibiotics to prevent Pneumocystis jirovecii pneumonia, and they should be monitored for respiratory signs and symptoms. Regular clinical and laboratory monitoring for cytomegalovirus infection is also recommended.
Patients should have regular blood tests to detect neutropenia. In case a patient has moderate or severe neutropenia, treatment with idelalisib may have to be interrupted, in line with the updated summary of product characteristics.
The EMA said further details on these provisional measures will be provided in writing to healthcare professionals, and the product information will be updated accordingly.
Likewise, further information on the review of idelalisib will be provided as necessary and once the review is finished.
About the review
The EMA’s review of idelalisib started after a higher rate of serious adverse events, including deaths, was seen in 3 clinical trials evaluating the addition of idelalisib to standard therapy in first-line CLL and relapsed indolent non-Hodgkin lymphoma (NHL).
Most of the deaths were related to infections such as Pneumocystis jirovecii pneumonia and cytomegalovirus infection. Other excess deaths were related mainly to respiratory events.
The NHL studies (NCT01732926 and NCT01732913) included patients with disease characteristics different from those covered by the currently approved indication for idelalisib and investigated combinations of drugs that are not currently approved in the EU—idelalisib plus rituximab for NHL and idelalisib plus bendamustine and rituximab for NHL.
The CLL trial (NCT01980888) involved patients who had not received previous treatment, some of whom had the 17p deletion or TP53 mutation. However, the trial also investigated a combination of drugs not currently approved in the EU—idelalisib plus bendamustine and rituximab.
At present, the PRAC is conducting the review. Once the PRAC is finished, its recommendations will be forwarded to the EMA’s Committee for Medicinal Products for Human Use, which will adopt a final opinion.
The European Commission will take this opinion into account and adopt a legally binding decision that is applicable in all EU member states. ![]()
FDA proposes ban on most powdered medical gloves

Photo by Chonion Antoine
The US Food and Drug Administration (FDA) is proposing a ban on most powdered gloves in the US.
The proposed ban applies to powdered surgeon’s gloves, powdered patient examination gloves, and absorbable powder for lubricating a surgeon’s glove.
The FDA said these gloves pose an unreasonable and substantial risk of illness or injury to healthcare providers, patients, and other individuals who are exposed to them, which cannot be corrected through new or updated labeling.
“This ban is about protecting patients and healthcare professionals from a danger they might not even be aware of,” said Jeffrey Shuren, MD, director of FDA’s Center for Devices and Radiological Health.
“We take bans very seriously and only take this action when we feel it’s necessary to protect the public health.”
The FDA said powdered gloves are dangerous for a variety of reasons. In particular, aerosolized glove powder on natural rubber latex gloves, but not on synthetic powdered gloves, can carry proteins that may cause respiratory allergic reactions.
Although powdered synthetic gloves do not present the risk of allergic reactions, these gloves are associated with an extensive list of potentially serious adverse events, including severe airway inflammation, wound inflammation, and post-surgical adhesions. These side effects have been attributed to the use of glove powder with all types of gloves.
As these risks cannot be corrected through new or updated labeling, the FDA is moving forward with the proposal to ban these products, which—if finalized—would ultimately remove them from the marketplace completely.
In making the determination that these products are dangerous and present an unreasonable and substantial risk, the FDA considered all available evidence, which included a thorough review of the scientific literature and comments received on a February 2011 Federal Register Notice.
The FDA also conducted an economic analysis that showed a powdered glove ban would not cause a glove shortage, and the economic impact of a ban would not be significant. The ban is also not likely to impact medical practice, because many non-powdered protective glove options are currently available.
The FDA has determined that the banning standard would not apply to powdered radiographic protection gloves. The agency is not aware of any powdered radiographic protection gloves that are currently on the market.
Non-powdered surgeon gloves and non-powdered patient examination gloves will not be included in the ban and will remain Class I medical devices. Therefore, the FDA is also proposing amendments to their classification regulations to clarify that they apply only to non-powdered gloves.
The proposed rule is available online at www.regulations.gov for public comment for 90 days. ![]()
Photo by Chonion Antoine
The US Food and Drug Administration (FDA) is proposing a ban on most powdered gloves in the US.
The proposed ban applies to powdered surgeon’s gloves, powdered patient examination gloves, and absorbable powder for lubricating a surgeon’s glove.
The FDA said these gloves pose an unreasonable and substantial risk of illness or injury to healthcare providers, patients, and other individuals who are exposed to them, which cannot be corrected through new or updated labeling.
“This ban is about protecting patients and healthcare professionals from a danger they might not even be aware of,” said Jeffrey Shuren, MD, director of FDA’s Center for Devices and Radiological Health.
“We take bans very seriously and only take this action when we feel it’s necessary to protect the public health.”
The FDA said powdered gloves are dangerous for a variety of reasons. In particular, aerosolized glove powder on natural rubber latex gloves, but not on synthetic powdered gloves, can carry proteins that may cause respiratory allergic reactions.
Although powdered synthetic gloves do not present the risk of allergic reactions, these gloves are associated with an extensive list of potentially serious adverse events, including severe airway inflammation, wound inflammation, and post-surgical adhesions. These side effects have been attributed to the use of glove powder with all types of gloves.
As these risks cannot be corrected through new or updated labeling, the FDA is moving forward with the proposal to ban these products, which—if finalized—would ultimately remove them from the marketplace completely.
In making the determination that these products are dangerous and present an unreasonable and substantial risk, the FDA considered all available evidence, which included a thorough review of the scientific literature and comments received on a February 2011 Federal Register Notice.
The FDA also conducted an economic analysis that showed a powdered glove ban would not cause a glove shortage, and the economic impact of a ban would not be significant. The ban is also not likely to impact medical practice, because many non-powdered protective glove options are currently available.
The FDA has determined that the banning standard would not apply to powdered radiographic protection gloves. The agency is not aware of any powdered radiographic protection gloves that are currently on the market.
Non-powdered surgeon gloves and non-powdered patient examination gloves will not be included in the ban and will remain Class I medical devices. Therefore, the FDA is also proposing amendments to their classification regulations to clarify that they apply only to non-powdered gloves.
The proposed rule is available online at www.regulations.gov for public comment for 90 days. ![]()
Photo by Chonion Antoine
The US Food and Drug Administration (FDA) is proposing a ban on most powdered gloves in the US.
The proposed ban applies to powdered surgeon’s gloves, powdered patient examination gloves, and absorbable powder for lubricating a surgeon’s glove.
The FDA said these gloves pose an unreasonable and substantial risk of illness or injury to healthcare providers, patients, and other individuals who are exposed to them, which cannot be corrected through new or updated labeling.
“This ban is about protecting patients and healthcare professionals from a danger they might not even be aware of,” said Jeffrey Shuren, MD, director of FDA’s Center for Devices and Radiological Health.
“We take bans very seriously and only take this action when we feel it’s necessary to protect the public health.”
The FDA said powdered gloves are dangerous for a variety of reasons. In particular, aerosolized glove powder on natural rubber latex gloves, but not on synthetic powdered gloves, can carry proteins that may cause respiratory allergic reactions.
Although powdered synthetic gloves do not present the risk of allergic reactions, these gloves are associated with an extensive list of potentially serious adverse events, including severe airway inflammation, wound inflammation, and post-surgical adhesions. These side effects have been attributed to the use of glove powder with all types of gloves.
As these risks cannot be corrected through new or updated labeling, the FDA is moving forward with the proposal to ban these products, which—if finalized—would ultimately remove them from the marketplace completely.
In making the determination that these products are dangerous and present an unreasonable and substantial risk, the FDA considered all available evidence, which included a thorough review of the scientific literature and comments received on a February 2011 Federal Register Notice.
The FDA also conducted an economic analysis that showed a powdered glove ban would not cause a glove shortage, and the economic impact of a ban would not be significant. The ban is also not likely to impact medical practice, because many non-powdered protective glove options are currently available.
The FDA has determined that the banning standard would not apply to powdered radiographic protection gloves. The agency is not aware of any powdered radiographic protection gloves that are currently on the market.
Non-powdered surgeon gloves and non-powdered patient examination gloves will not be included in the ban and will remain Class I medical devices. Therefore, the FDA is also proposing amendments to their classification regulations to clarify that they apply only to non-powdered gloves.
The proposed rule is available online at www.regulations.gov for public comment for 90 days. ![]()
Four genes control growth of HSCs, team says
Image by John Perry
Four genes govern the growth and multiplication of hematopoietic stem cells (HSCs), according to a study published in Cell Reports.
Investigators conducted a genome-wide RNA interference screen in cells derived from human cord blood, looking for genes whose knockdown maintained the HSC phenotype during culture.
This revealed the 4 genes—STAG2, RAD21, STAG1, and SMC3—which are all members of the cohesin complex.
“The discovery showed that this protein complex is crucial and has an overarching function in the growth of the blood stem cells,” said study author Jonas Larsson, MD, PhD, of Lund University in Sweden.
Dr Larsson and his colleagues screened 15,000 genes for this study and found 20 candidates with a strong capacity to affect the balance of growth in HSCs.
Four of the genes—STAG2, RAD21, STAG1, and SMC3—were physically connected through cooperation in the cohesin complex. This complex forms a sort of brace that holds different parts of the DNA strand together in the cell.
The researchers believe this allows the cohesin complex to control access to the “on/off switches” in the DNA and to change the impulses that HSCs receive from various genes, thereby affecting whether an HSC multiplies or matures.
“Clarifying what regulates the balance between multiplication and maturation of blood stem cells could provide the right keys to expanding them outside the body,” said Roman Galeev, a doctoral student at Lund University.
“In addition, it would enable the identification of new points of attack for the treatment of blood cancer, which is precisely a disruption of the balance between multiplication and maturation.”
Galeev noted that research by other groups has revealed mutations in the cohesin complex genes in patients with hematologic malignancies (Mazumdar C, Cell Stem Cell 2015; Mullenders J, J Exp Med 2015; and Viny AD, J Exp Med 2015).
“This is incredibly exciting,” Galeev said. “Together with the results from our study, this indicates that the cohesin genes are directly and crucially significant in the development of blood cancer.”
“Our findings entail a new understanding of how the expansion of blood stem cells is controlled. Eventually, this can lead to new ways of affecting the process, either to prevent the development of cancer or to expand the stem cells for transplant.” ![]()
Image by John Perry
Four genes govern the growth and multiplication of hematopoietic stem cells (HSCs), according to a study published in Cell Reports.
Investigators conducted a genome-wide RNA interference screen in cells derived from human cord blood, looking for genes whose knockdown maintained the HSC phenotype during culture.
This revealed the 4 genes—STAG2, RAD21, STAG1, and SMC3—which are all members of the cohesin complex.
“The discovery showed that this protein complex is crucial and has an overarching function in the growth of the blood stem cells,” said study author Jonas Larsson, MD, PhD, of Lund University in Sweden.
Dr Larsson and his colleagues screened 15,000 genes for this study and found 20 candidates with a strong capacity to affect the balance of growth in HSCs.
Four of the genes—STAG2, RAD21, STAG1, and SMC3—were physically connected through cooperation in the cohesin complex. This complex forms a sort of brace that holds different parts of the DNA strand together in the cell.
The researchers believe this allows the cohesin complex to control access to the “on/off switches” in the DNA and to change the impulses that HSCs receive from various genes, thereby affecting whether an HSC multiplies or matures.
“Clarifying what regulates the balance between multiplication and maturation of blood stem cells could provide the right keys to expanding them outside the body,” said Roman Galeev, a doctoral student at Lund University.
“In addition, it would enable the identification of new points of attack for the treatment of blood cancer, which is precisely a disruption of the balance between multiplication and maturation.”
Galeev noted that research by other groups has revealed mutations in the cohesin complex genes in patients with hematologic malignancies (Mazumdar C, Cell Stem Cell 2015; Mullenders J, J Exp Med 2015; and Viny AD, J Exp Med 2015).
“This is incredibly exciting,” Galeev said. “Together with the results from our study, this indicates that the cohesin genes are directly and crucially significant in the development of blood cancer.”
“Our findings entail a new understanding of how the expansion of blood stem cells is controlled. Eventually, this can lead to new ways of affecting the process, either to prevent the development of cancer or to expand the stem cells for transplant.” ![]()
Image by John Perry
Four genes govern the growth and multiplication of hematopoietic stem cells (HSCs), according to a study published in Cell Reports.
Investigators conducted a genome-wide RNA interference screen in cells derived from human cord blood, looking for genes whose knockdown maintained the HSC phenotype during culture.
This revealed the 4 genes—STAG2, RAD21, STAG1, and SMC3—which are all members of the cohesin complex.
“The discovery showed that this protein complex is crucial and has an overarching function in the growth of the blood stem cells,” said study author Jonas Larsson, MD, PhD, of Lund University in Sweden.
Dr Larsson and his colleagues screened 15,000 genes for this study and found 20 candidates with a strong capacity to affect the balance of growth in HSCs.
Four of the genes—STAG2, RAD21, STAG1, and SMC3—were physically connected through cooperation in the cohesin complex. This complex forms a sort of brace that holds different parts of the DNA strand together in the cell.
The researchers believe this allows the cohesin complex to control access to the “on/off switches” in the DNA and to change the impulses that HSCs receive from various genes, thereby affecting whether an HSC multiplies or matures.
“Clarifying what regulates the balance between multiplication and maturation of blood stem cells could provide the right keys to expanding them outside the body,” said Roman Galeev, a doctoral student at Lund University.
“In addition, it would enable the identification of new points of attack for the treatment of blood cancer, which is precisely a disruption of the balance between multiplication and maturation.”
Galeev noted that research by other groups has revealed mutations in the cohesin complex genes in patients with hematologic malignancies (Mazumdar C, Cell Stem Cell 2015; Mullenders J, J Exp Med 2015; and Viny AD, J Exp Med 2015).
“This is incredibly exciting,” Galeev said. “Together with the results from our study, this indicates that the cohesin genes are directly and crucially significant in the development of blood cancer.”
“Our findings entail a new understanding of how the expansion of blood stem cells is controlled. Eventually, this can lead to new ways of affecting the process, either to prevent the development of cancer or to expand the stem cells for transplant.” ![]()
Cyclosporine in SJS/TEN Management: A Brief Review
As dermatology residents, the telephone calls we get at 2 am usually are the toughest for 2 reasons: (1) we rarely get calls at 2 am, and (2) it usually means there is a case to rule out Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). Stevens-Johnson syndrome and TEN are severe mucocutaneous eruptions that usually develop due to drug reactions and involve a continuum of conjunctivitis, mucocutaneous sloughing, keratinocyte death, and bullae development. Body surface area (BSA) coverage determines the distinction between SJS and TEN; less than 10% BSA affected indicates SJS, 10% to 30% BSA affected indicates overlap between SJS and TEN, and greater than 30% BSA affected indicates TEN.1 The mortality rates for these conditions range from 1% to 5% in SJS versus 25% to 30% in TEN.2
Being driven and dedicated residents, we rise to the challenge by arranging appropriate consultations, obtaining frozen section biopsies, providing recommendations to remove unnecessary medications, and offering skin care management. However, what comes next? Intravenous immunoglobulin (IVIG)? Cyclosporine? Or is it appropriate to allow the reaction to continue its course? Dermatology programs have a varying standard of care due to the limited number of studies conducted on SJS/TEN patients. Few studies have relayed the efficacy of cyclosporine; however, published results have shown that cyclosporine can decrease the overall mortality risk and minimize disease progression.2-5 In this article, I will review some of the key studies conducted in the last 5 years regarding the use of cyclosporine in the therapeutic plan for SJS/TEN.
In one retrospective analysis conducted by Kirchhof et al1 in 2014, 35 patients with SJS/TEN who were treated with IVIG and 15 who were treated with cyclosporine were evaluated for mortality benefit. Two patients were treated with both cyclosporine and IVIG and were included in both arms of the study. Overall, the evaluation indicated that cyclosporine can potentially have a better overall advantage in treatment of SJS/TEN over IVIG.1 Although this study had an uneven number of patients treated with IVIG versus cyclosporine, a nonstandardized way of comparing patients with early SJS to TEN patients, and no double-blind randomized trial, cyclosporine may still show benefit over IVIG.
Singh et al6 conducted an uncontrolled open study in a tertiary care center (July 2011–June 2012) that showed a similar result of benefit with cyclosporine in SJS, SJS/TEN, and TEN patients. Eleven participants were included in the study based on SCORTEN (Score of Toxic Epidermal Necrosis) criteria (age, >40 years; heart rate, >120 BPM; serum blood urea nitrogen level, >28 mg/dL; body surface area affected, >10%; serum bicarbonate, >20 mEq/L; serum glucose, >252 mg/dL). They were treated with cyclosporine 3 mg/kg for 7 days and then tapered over another 7 days. Six participants were treated with corticosteroids. Participants treated with cyclosporine reepithelialized in 16.7 days compared to 23 days with corticosteroids. The hospital stay was 18.09 days in participants treated with cyclosporine versus 26 days in those treated with corticosteroids. Lastly, 2 participants who were treated with corticosteroids died as opposed to none with cyclosporine.6 Although the power of this study also was limited and it was not a randomized, double-blind, controlled trial, it provides more evidence that cyclosporine can be efficacious in SJS/TEN patients.
A phase 2 open trial conducted by Valeyrie-Allanore et al7 evaluated the benefit and efficacy of cyclosporine in SJS/TEN patients. There were 29 participants at the start of the study (SJS, n=10; SJS/TEN, n=12; TEN, n=7) and 26 completed treatment. Cyclosporine was administered orally at 3 mg/kg for 10 days and tapered over the following month. This study noted 3 basic principles: First, patients tolerated cyclosporine well; second, limited disease progression was noted in 62% (18/29) of participants around day 3 and in only about 35% (11/29) of IVIG patients; and third, no deaths were noted in all participants.7
Final Thoughts
Case reports have indicated that cyclosporine may be effective in limiting progression of SJS/TEN; however, a double-blind study has not validated this finding. Hence, patients should be evaluated on a case-by-case basis to determine if they should be treated with cyclosporine or IVIG or simply complete the course of the disease process with supportive care.
1. Kirchhof MG, Miliszewski MA, Sikora S, et al. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J Am Acad Dermatol. 2014;71:941-947.
2. Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis, part I: introduction, history, classification, clinical features, systemic manifestations, etiology, and immunopathogenesis. J Am Acad Dermatol. 2013;69:173.e1-173.e13, quiz 185-186.
3. Arévalo JM, Lorente JA, González-Herrada C, et al. Treatment of toxic epidermal necrolysis with cyclosporin A. J Trauma. 2000;48:473-478.
4. Aihara Y, Ito R, Ito S, et al. Toxic epidermal necrolysis in a child successfully treated with cyclosporine A and methylprednisolone. Pediatr Int. 2007;49:659-662.
5. Hewitt J, Ormerod AD. Toxic epidermal necrolysis treated with cyclosporin. Clin Exp Dermatol. 1992;17:264-265.
6. Singh GK, Chatterjee M, Verma R. Cyclosporine in Stevens Johnson syndrome and toxic epidermal necrolysis and retrospective comparison with systemic corticosteroid. Indian J Dermatol Venereol Leprol. 2013;79:686-692.
7. Valeyrie-Allanore P, Wolkenstein L, Brochard N, et al. Open trial of ciclosporin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2010;163:847-853.
As dermatology residents, the telephone calls we get at 2 am usually are the toughest for 2 reasons: (1) we rarely get calls at 2 am, and (2) it usually means there is a case to rule out Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). Stevens-Johnson syndrome and TEN are severe mucocutaneous eruptions that usually develop due to drug reactions and involve a continuum of conjunctivitis, mucocutaneous sloughing, keratinocyte death, and bullae development. Body surface area (BSA) coverage determines the distinction between SJS and TEN; less than 10% BSA affected indicates SJS, 10% to 30% BSA affected indicates overlap between SJS and TEN, and greater than 30% BSA affected indicates TEN.1 The mortality rates for these conditions range from 1% to 5% in SJS versus 25% to 30% in TEN.2
Being driven and dedicated residents, we rise to the challenge by arranging appropriate consultations, obtaining frozen section biopsies, providing recommendations to remove unnecessary medications, and offering skin care management. However, what comes next? Intravenous immunoglobulin (IVIG)? Cyclosporine? Or is it appropriate to allow the reaction to continue its course? Dermatology programs have a varying standard of care due to the limited number of studies conducted on SJS/TEN patients. Few studies have relayed the efficacy of cyclosporine; however, published results have shown that cyclosporine can decrease the overall mortality risk and minimize disease progression.2-5 In this article, I will review some of the key studies conducted in the last 5 years regarding the use of cyclosporine in the therapeutic plan for SJS/TEN.
In one retrospective analysis conducted by Kirchhof et al1 in 2014, 35 patients with SJS/TEN who were treated with IVIG and 15 who were treated with cyclosporine were evaluated for mortality benefit. Two patients were treated with both cyclosporine and IVIG and were included in both arms of the study. Overall, the evaluation indicated that cyclosporine can potentially have a better overall advantage in treatment of SJS/TEN over IVIG.1 Although this study had an uneven number of patients treated with IVIG versus cyclosporine, a nonstandardized way of comparing patients with early SJS to TEN patients, and no double-blind randomized trial, cyclosporine may still show benefit over IVIG.
Singh et al6 conducted an uncontrolled open study in a tertiary care center (July 2011–June 2012) that showed a similar result of benefit with cyclosporine in SJS, SJS/TEN, and TEN patients. Eleven participants were included in the study based on SCORTEN (Score of Toxic Epidermal Necrosis) criteria (age, >40 years; heart rate, >120 BPM; serum blood urea nitrogen level, >28 mg/dL; body surface area affected, >10%; serum bicarbonate, >20 mEq/L; serum glucose, >252 mg/dL). They were treated with cyclosporine 3 mg/kg for 7 days and then tapered over another 7 days. Six participants were treated with corticosteroids. Participants treated with cyclosporine reepithelialized in 16.7 days compared to 23 days with corticosteroids. The hospital stay was 18.09 days in participants treated with cyclosporine versus 26 days in those treated with corticosteroids. Lastly, 2 participants who were treated with corticosteroids died as opposed to none with cyclosporine.6 Although the power of this study also was limited and it was not a randomized, double-blind, controlled trial, it provides more evidence that cyclosporine can be efficacious in SJS/TEN patients.
A phase 2 open trial conducted by Valeyrie-Allanore et al7 evaluated the benefit and efficacy of cyclosporine in SJS/TEN patients. There were 29 participants at the start of the study (SJS, n=10; SJS/TEN, n=12; TEN, n=7) and 26 completed treatment. Cyclosporine was administered orally at 3 mg/kg for 10 days and tapered over the following month. This study noted 3 basic principles: First, patients tolerated cyclosporine well; second, limited disease progression was noted in 62% (18/29) of participants around day 3 and in only about 35% (11/29) of IVIG patients; and third, no deaths were noted in all participants.7
Final Thoughts
Case reports have indicated that cyclosporine may be effective in limiting progression of SJS/TEN; however, a double-blind study has not validated this finding. Hence, patients should be evaluated on a case-by-case basis to determine if they should be treated with cyclosporine or IVIG or simply complete the course of the disease process with supportive care.
As dermatology residents, the telephone calls we get at 2 am usually are the toughest for 2 reasons: (1) we rarely get calls at 2 am, and (2) it usually means there is a case to rule out Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). Stevens-Johnson syndrome and TEN are severe mucocutaneous eruptions that usually develop due to drug reactions and involve a continuum of conjunctivitis, mucocutaneous sloughing, keratinocyte death, and bullae development. Body surface area (BSA) coverage determines the distinction between SJS and TEN; less than 10% BSA affected indicates SJS, 10% to 30% BSA affected indicates overlap between SJS and TEN, and greater than 30% BSA affected indicates TEN.1 The mortality rates for these conditions range from 1% to 5% in SJS versus 25% to 30% in TEN.2
Being driven and dedicated residents, we rise to the challenge by arranging appropriate consultations, obtaining frozen section biopsies, providing recommendations to remove unnecessary medications, and offering skin care management. However, what comes next? Intravenous immunoglobulin (IVIG)? Cyclosporine? Or is it appropriate to allow the reaction to continue its course? Dermatology programs have a varying standard of care due to the limited number of studies conducted on SJS/TEN patients. Few studies have relayed the efficacy of cyclosporine; however, published results have shown that cyclosporine can decrease the overall mortality risk and minimize disease progression.2-5 In this article, I will review some of the key studies conducted in the last 5 years regarding the use of cyclosporine in the therapeutic plan for SJS/TEN.
In one retrospective analysis conducted by Kirchhof et al1 in 2014, 35 patients with SJS/TEN who were treated with IVIG and 15 who were treated with cyclosporine were evaluated for mortality benefit. Two patients were treated with both cyclosporine and IVIG and were included in both arms of the study. Overall, the evaluation indicated that cyclosporine can potentially have a better overall advantage in treatment of SJS/TEN over IVIG.1 Although this study had an uneven number of patients treated with IVIG versus cyclosporine, a nonstandardized way of comparing patients with early SJS to TEN patients, and no double-blind randomized trial, cyclosporine may still show benefit over IVIG.
Singh et al6 conducted an uncontrolled open study in a tertiary care center (July 2011–June 2012) that showed a similar result of benefit with cyclosporine in SJS, SJS/TEN, and TEN patients. Eleven participants were included in the study based on SCORTEN (Score of Toxic Epidermal Necrosis) criteria (age, >40 years; heart rate, >120 BPM; serum blood urea nitrogen level, >28 mg/dL; body surface area affected, >10%; serum bicarbonate, >20 mEq/L; serum glucose, >252 mg/dL). They were treated with cyclosporine 3 mg/kg for 7 days and then tapered over another 7 days. Six participants were treated with corticosteroids. Participants treated with cyclosporine reepithelialized in 16.7 days compared to 23 days with corticosteroids. The hospital stay was 18.09 days in participants treated with cyclosporine versus 26 days in those treated with corticosteroids. Lastly, 2 participants who were treated with corticosteroids died as opposed to none with cyclosporine.6 Although the power of this study also was limited and it was not a randomized, double-blind, controlled trial, it provides more evidence that cyclosporine can be efficacious in SJS/TEN patients.
A phase 2 open trial conducted by Valeyrie-Allanore et al7 evaluated the benefit and efficacy of cyclosporine in SJS/TEN patients. There were 29 participants at the start of the study (SJS, n=10; SJS/TEN, n=12; TEN, n=7) and 26 completed treatment. Cyclosporine was administered orally at 3 mg/kg for 10 days and tapered over the following month. This study noted 3 basic principles: First, patients tolerated cyclosporine well; second, limited disease progression was noted in 62% (18/29) of participants around day 3 and in only about 35% (11/29) of IVIG patients; and third, no deaths were noted in all participants.7
Final Thoughts
Case reports have indicated that cyclosporine may be effective in limiting progression of SJS/TEN; however, a double-blind study has not validated this finding. Hence, patients should be evaluated on a case-by-case basis to determine if they should be treated with cyclosporine or IVIG or simply complete the course of the disease process with supportive care.
1. Kirchhof MG, Miliszewski MA, Sikora S, et al. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J Am Acad Dermatol. 2014;71:941-947.
2. Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis, part I: introduction, history, classification, clinical features, systemic manifestations, etiology, and immunopathogenesis. J Am Acad Dermatol. 2013;69:173.e1-173.e13, quiz 185-186.
3. Arévalo JM, Lorente JA, González-Herrada C, et al. Treatment of toxic epidermal necrolysis with cyclosporin A. J Trauma. 2000;48:473-478.
4. Aihara Y, Ito R, Ito S, et al. Toxic epidermal necrolysis in a child successfully treated with cyclosporine A and methylprednisolone. Pediatr Int. 2007;49:659-662.
5. Hewitt J, Ormerod AD. Toxic epidermal necrolysis treated with cyclosporin. Clin Exp Dermatol. 1992;17:264-265.
6. Singh GK, Chatterjee M, Verma R. Cyclosporine in Stevens Johnson syndrome and toxic epidermal necrolysis and retrospective comparison with systemic corticosteroid. Indian J Dermatol Venereol Leprol. 2013;79:686-692.
7. Valeyrie-Allanore P, Wolkenstein L, Brochard N, et al. Open trial of ciclosporin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2010;163:847-853.
1. Kirchhof MG, Miliszewski MA, Sikora S, et al. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J Am Acad Dermatol. 2014;71:941-947.
2. Schwartz RA, McDonough PH, Lee BW. Toxic epidermal necrolysis, part I: introduction, history, classification, clinical features, systemic manifestations, etiology, and immunopathogenesis. J Am Acad Dermatol. 2013;69:173.e1-173.e13, quiz 185-186.
3. Arévalo JM, Lorente JA, González-Herrada C, et al. Treatment of toxic epidermal necrolysis with cyclosporin A. J Trauma. 2000;48:473-478.
4. Aihara Y, Ito R, Ito S, et al. Toxic epidermal necrolysis in a child successfully treated with cyclosporine A and methylprednisolone. Pediatr Int. 2007;49:659-662.
5. Hewitt J, Ormerod AD. Toxic epidermal necrolysis treated with cyclosporin. Clin Exp Dermatol. 1992;17:264-265.
6. Singh GK, Chatterjee M, Verma R. Cyclosporine in Stevens Johnson syndrome and toxic epidermal necrolysis and retrospective comparison with systemic corticosteroid. Indian J Dermatol Venereol Leprol. 2013;79:686-692.
7. Valeyrie-Allanore P, Wolkenstein L, Brochard N, et al. Open trial of ciclosporin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 2010;163:847-853.

Wanted: Better evidence on fast-track lung resection
A host of medical specialties have adopted strategies to speed recovery of surgical patients, reduce length of hospital stays, and cut costs, known as fast-track or enhanced-recovery pathways, but when it comes to elective lung resection, the medical evidence has yet to establish if patients in expedited recovery protocols fare any better than do those in a conventional recovery course, a systematic review in the March issue of the Journal of Thoracic and Cardiovascular Surgery reported (2016 Mar;151:708-15).
A team of investigators from McGill University in Montreal performed a systematic review of six studies that evaluated patient outcomes of both traditional and enhanced-recovery pathways (ERPs) in elective lung resection. They concluded that ERPs may reduce the length of hospital stays and hospital costs but that well-designed trials are needed to overcome limitations of existing studies.
“The influence of ERPs on postoperative outcomes after lung resection has not been extensively studied in comparative studies involving a control group receiving traditional care,” lead author Julio F. Fiore Jr., Ph.D., and his colleagues said. One of the six studies they reviewed was a randomized clinical trial. The six studies involved a total of 1,612 participants (821 ERP, 791 control).
The researchers also reported that the studies they analyzed shared a significant limitation. “Risk of bias favoring enhanced-recovery pathways was high,” Dr. Fiore and his colleagues wrote. The studies were unclear if patient selection may have factored into the results.
Five studies reported shorter hospital length of stay (LOS) for the ERP group. “The majority of the studies reported that LOS was significantly shorter when patients undergoing lung resection were treated within an ERP, which corroborates the results observed in other surgical populations,” Dr. Fiore and his colleagues said.
Three nonrandomized studies also evaluated costs per patient. Two reported significantly lower costs for ERP patients: $13,093 vs. $14,439 for controls; and $13,432 vs. $17,103 for controls (Jpn. J. Thorac. Cardiovasc. Surg. 2006 Sep;54:387-90; Ann. Thorac. Surg. 1998 Sep;66:914-9). The third showed what the authors said was no statistically significant cost differential between the two groups: $14,792 for ERP vs. $16,063 for controls (Ann. Thorac. Surg. 1997 Aug;64:299-302).
Three studies evaluated readmission rates, but only one showed measurably lower rates for the ERP group: 3% vs. 10% for controls (Lung Cancer. 2012 Dec;78:270-5). Three studies measured complication rates in both groups. Two reported cardiopulmonary complication rates of 18% and 17% in the ERP group vs. 16% and 14% in the control group, respectively (Eur. J. Cardiothorac. Surg. 2012 May;41:1083-7; Lung Cancer. 2012 Dec;78:270-5). One reported rates of pulmonary complications of 7% for ERP vs. 36% for controls (Eur. J. Cardiothorac. Surg. 2008 Jul;34:174-80).
Dr. Fiore and his colleagues pointed out that some of the studies they reviewed were completed before video-assisted thoracic surgery became routine for lung resection. But they acknowledged that research in other surgical specialties have validated the role of ERP, along with minimally invasive surgery, to improve outcomes. “Future research should investigate whether this holds true for patients undergoing lung resection,” they said.
The study authors had no financial relationships to disclose.
The task that Dr. Fiore and colleagues undertook to evaluate and compare disparate studies of fast-track surgery in lung resection is “akin to comparing not just apples and oranges but apples to zucchini,” Dr. Lisa M. Brown of University of California, Davis, Medical Center said in her invited analysis (J. Thorac. Cardiovasc. Surg. 2016 Mar;151:715-16). Without the authors’ “descriptive approach,” Dr. Brown said, “the results of a true meta-analysis would be uninterpretable.”

|
Dr. Lisa M. Brown |
Nonetheless, the systematic review underscores the need for a blinded, randomized trial, Dr. Brown said. “Furthermore, rather than measuring [hospital] stay, subjects should be evaluated for readiness for discharge, because this would reduce the effect of systems-based obstacles to discharge,” she said. Enhanced recovery pathways (ERPs) in colorectal surgery have been used as models for other specialties, but the novelty of these pathways versus traditional care may be difficult to replicate in thoracic surgery, she said. Strategies such as antibiotic prophylaxis and epidural analgesia in thoracic surgery “are not dissimilar enough from standard care to elicit a difference in outcome,” she said.
In thoracic surgery, ERPs must consider the challenges of pain control and chest tube management unique in these patients, Dr. Brown said. For pain control, paravertebral blockade rather than epidural analgesia could lead to earlier hospital discharges. Use of chest tubes is commonly a matter of surgeon preference, she said, but chest tubes without an air leak and with acceptable fluid output can be safely removed, and even patients with an air leak but no pneumothorax on water seal can go home with a chest tube, Dr. Brown said.
Dr. Brown had no financial relationships to disclose.
The task that Dr. Fiore and colleagues undertook to evaluate and compare disparate studies of fast-track surgery in lung resection is “akin to comparing not just apples and oranges but apples to zucchini,” Dr. Lisa M. Brown of University of California, Davis, Medical Center said in her invited analysis (J. Thorac. Cardiovasc. Surg. 2016 Mar;151:715-16). Without the authors’ “descriptive approach,” Dr. Brown said, “the results of a true meta-analysis would be uninterpretable.”
|
|
Dr. Lisa M. Brown |
Nonetheless, the systematic review underscores the need for a blinded, randomized trial, Dr. Brown said. “Furthermore, rather than measuring [hospital] stay, subjects should be evaluated for readiness for discharge, because this would reduce the effect of systems-based obstacles to discharge,” she said. Enhanced recovery pathways (ERPs) in colorectal surgery have been used as models for other specialties, but the novelty of these pathways versus traditional care may be difficult to replicate in thoracic surgery, she said. Strategies such as antibiotic prophylaxis and epidural analgesia in thoracic surgery “are not dissimilar enough from standard care to elicit a difference in outcome,” she said.
In thoracic surgery, ERPs must consider the challenges of pain control and chest tube management unique in these patients, Dr. Brown said. For pain control, paravertebral blockade rather than epidural analgesia could lead to earlier hospital discharges. Use of chest tubes is commonly a matter of surgeon preference, she said, but chest tubes without an air leak and with acceptable fluid output can be safely removed, and even patients with an air leak but no pneumothorax on water seal can go home with a chest tube, Dr. Brown said.
Dr. Brown had no financial relationships to disclose.
The task that Dr. Fiore and colleagues undertook to evaluate and compare disparate studies of fast-track surgery in lung resection is “akin to comparing not just apples and oranges but apples to zucchini,” Dr. Lisa M. Brown of University of California, Davis, Medical Center said in her invited analysis (J. Thorac. Cardiovasc. Surg. 2016 Mar;151:715-16). Without the authors’ “descriptive approach,” Dr. Brown said, “the results of a true meta-analysis would be uninterpretable.”
|
|
Dr. Lisa M. Brown |
Nonetheless, the systematic review underscores the need for a blinded, randomized trial, Dr. Brown said. “Furthermore, rather than measuring [hospital] stay, subjects should be evaluated for readiness for discharge, because this would reduce the effect of systems-based obstacles to discharge,” she said. Enhanced recovery pathways (ERPs) in colorectal surgery have been used as models for other specialties, but the novelty of these pathways versus traditional care may be difficult to replicate in thoracic surgery, she said. Strategies such as antibiotic prophylaxis and epidural analgesia in thoracic surgery “are not dissimilar enough from standard care to elicit a difference in outcome,” she said.
In thoracic surgery, ERPs must consider the challenges of pain control and chest tube management unique in these patients, Dr. Brown said. For pain control, paravertebral blockade rather than epidural analgesia could lead to earlier hospital discharges. Use of chest tubes is commonly a matter of surgeon preference, she said, but chest tubes without an air leak and with acceptable fluid output can be safely removed, and even patients with an air leak but no pneumothorax on water seal can go home with a chest tube, Dr. Brown said.
Dr. Brown had no financial relationships to disclose.
A host of medical specialties have adopted strategies to speed recovery of surgical patients, reduce length of hospital stays, and cut costs, known as fast-track or enhanced-recovery pathways, but when it comes to elective lung resection, the medical evidence has yet to establish if patients in expedited recovery protocols fare any better than do those in a conventional recovery course, a systematic review in the March issue of the Journal of Thoracic and Cardiovascular Surgery reported (2016 Mar;151:708-15).
A team of investigators from McGill University in Montreal performed a systematic review of six studies that evaluated patient outcomes of both traditional and enhanced-recovery pathways (ERPs) in elective lung resection. They concluded that ERPs may reduce the length of hospital stays and hospital costs but that well-designed trials are needed to overcome limitations of existing studies.
“The influence of ERPs on postoperative outcomes after lung resection has not been extensively studied in comparative studies involving a control group receiving traditional care,” lead author Julio F. Fiore Jr., Ph.D., and his colleagues said. One of the six studies they reviewed was a randomized clinical trial. The six studies involved a total of 1,612 participants (821 ERP, 791 control).
The researchers also reported that the studies they analyzed shared a significant limitation. “Risk of bias favoring enhanced-recovery pathways was high,” Dr. Fiore and his colleagues wrote. The studies were unclear if patient selection may have factored into the results.
Five studies reported shorter hospital length of stay (LOS) for the ERP group. “The majority of the studies reported that LOS was significantly shorter when patients undergoing lung resection were treated within an ERP, which corroborates the results observed in other surgical populations,” Dr. Fiore and his colleagues said.
Three nonrandomized studies also evaluated costs per patient. Two reported significantly lower costs for ERP patients: $13,093 vs. $14,439 for controls; and $13,432 vs. $17,103 for controls (Jpn. J. Thorac. Cardiovasc. Surg. 2006 Sep;54:387-90; Ann. Thorac. Surg. 1998 Sep;66:914-9). The third showed what the authors said was no statistically significant cost differential between the two groups: $14,792 for ERP vs. $16,063 for controls (Ann. Thorac. Surg. 1997 Aug;64:299-302).
Three studies evaluated readmission rates, but only one showed measurably lower rates for the ERP group: 3% vs. 10% for controls (Lung Cancer. 2012 Dec;78:270-5). Three studies measured complication rates in both groups. Two reported cardiopulmonary complication rates of 18% and 17% in the ERP group vs. 16% and 14% in the control group, respectively (Eur. J. Cardiothorac. Surg. 2012 May;41:1083-7; Lung Cancer. 2012 Dec;78:270-5). One reported rates of pulmonary complications of 7% for ERP vs. 36% for controls (Eur. J. Cardiothorac. Surg. 2008 Jul;34:174-80).
Dr. Fiore and his colleagues pointed out that some of the studies they reviewed were completed before video-assisted thoracic surgery became routine for lung resection. But they acknowledged that research in other surgical specialties have validated the role of ERP, along with minimally invasive surgery, to improve outcomes. “Future research should investigate whether this holds true for patients undergoing lung resection,” they said.
The study authors had no financial relationships to disclose.
A host of medical specialties have adopted strategies to speed recovery of surgical patients, reduce length of hospital stays, and cut costs, known as fast-track or enhanced-recovery pathways, but when it comes to elective lung resection, the medical evidence has yet to establish if patients in expedited recovery protocols fare any better than do those in a conventional recovery course, a systematic review in the March issue of the Journal of Thoracic and Cardiovascular Surgery reported (2016 Mar;151:708-15).
A team of investigators from McGill University in Montreal performed a systematic review of six studies that evaluated patient outcomes of both traditional and enhanced-recovery pathways (ERPs) in elective lung resection. They concluded that ERPs may reduce the length of hospital stays and hospital costs but that well-designed trials are needed to overcome limitations of existing studies.
“The influence of ERPs on postoperative outcomes after lung resection has not been extensively studied in comparative studies involving a control group receiving traditional care,” lead author Julio F. Fiore Jr., Ph.D., and his colleagues said. One of the six studies they reviewed was a randomized clinical trial. The six studies involved a total of 1,612 participants (821 ERP, 791 control).
The researchers also reported that the studies they analyzed shared a significant limitation. “Risk of bias favoring enhanced-recovery pathways was high,” Dr. Fiore and his colleagues wrote. The studies were unclear if patient selection may have factored into the results.
Five studies reported shorter hospital length of stay (LOS) for the ERP group. “The majority of the studies reported that LOS was significantly shorter when patients undergoing lung resection were treated within an ERP, which corroborates the results observed in other surgical populations,” Dr. Fiore and his colleagues said.
Three nonrandomized studies also evaluated costs per patient. Two reported significantly lower costs for ERP patients: $13,093 vs. $14,439 for controls; and $13,432 vs. $17,103 for controls (Jpn. J. Thorac. Cardiovasc. Surg. 2006 Sep;54:387-90; Ann. Thorac. Surg. 1998 Sep;66:914-9). The third showed what the authors said was no statistically significant cost differential between the two groups: $14,792 for ERP vs. $16,063 for controls (Ann. Thorac. Surg. 1997 Aug;64:299-302).
Three studies evaluated readmission rates, but only one showed measurably lower rates for the ERP group: 3% vs. 10% for controls (Lung Cancer. 2012 Dec;78:270-5). Three studies measured complication rates in both groups. Two reported cardiopulmonary complication rates of 18% and 17% in the ERP group vs. 16% and 14% in the control group, respectively (Eur. J. Cardiothorac. Surg. 2012 May;41:1083-7; Lung Cancer. 2012 Dec;78:270-5). One reported rates of pulmonary complications of 7% for ERP vs. 36% for controls (Eur. J. Cardiothorac. Surg. 2008 Jul;34:174-80).
Dr. Fiore and his colleagues pointed out that some of the studies they reviewed were completed before video-assisted thoracic surgery became routine for lung resection. But they acknowledged that research in other surgical specialties have validated the role of ERP, along with minimally invasive surgery, to improve outcomes. “Future research should investigate whether this holds true for patients undergoing lung resection,” they said.
The study authors had no financial relationships to disclose.
Key clinical point: Well-designed clinical trials are needed to determine the effectiveness of fast-track recovery pathways in lung resection.
Major finding: Fast-track lung resection patients showed no differences in readmissions, overall complication and death rates compared to patients subjected to a traditional recovery course.
Data source: Systematic review of six studies published from 1997 to 2012 that involved 1,612 individuals who had lung resection.
Disclosures: The study authors had no financial relationships to disclose.

Antisclerostin osteoporosis drugs might worsen or unmask rheumatoid arthritis
Antisclerostin monoclonal antibodies have shown their ability to increase bone density in phase II and III trials of men and women with osteoporosis but could potentially have the opposite effect in patients with rheumatoid arthritis or other chronic inflammatory diseases in which tumor necrosis factor–alpha (TNF-alpha) plays an important role, according to new research.
The new work, conducted by Corinna Wehmeyer, Ph.D., of the Institute of Experimental Musculoskeletal Medicine at University Hospital Muenster (Germany) and her colleagues, shows that the bone formation–inhibiting protein sclerostin is not expressed in bone only, as was previously thought, but is also expressed on the synovial cells of patients with rheumatoid arthritis (RA).

Dr. Wehmeyer and her associates were surprised to find that inhibiting sclerostin in a human TNF-alpha transgenic mouse model of RA actually accelerated joint damage rather than prevented it, suggesting that sclerostin actually had a protective role in the presence of chronic TNF-alpha–mediated inflammation. They confirmed this by demonstrating that sclerostin inhibited TNF-alpha signaling in fibroblast-like synoviocytes and showing that blocking sclerostin caused less or little worsening of bone erosions in mouse models of RA that are more dependent on a robust T and B cell response accompanied by high cytokine expression within the joint, rather than damage driven by TNF-alpha.
“These findings strongly suggest that in chronic TNF-alpha–mediated inflammation, sclerostin expression is upregulated as part of an attempt to reestablish bone homeostasis, where it exerts protective functions,” the authors wrote (Sci Transl Med. 2016 Mar 16;8:330ra34. doi: 10.1126/scitranslmed.aac4351).
The research needs confirmation in humans with RA and potentially in other chronic inflammatory diseases in which TNF-alpha plays an important role. “Nevertheless, the preliminary data in three different models indicate that sclerostin antibody therapy could be contraindicated in patients with chronic TNF-alpha–dependent inflammatory conditions. The possibility of adverse pathological effects means that caution should be taken both when considering such treatment in RA or in patients with chronic TNF-alpha–dependent comorbidities. Thus, to translate these findings to patients, first strategies to use sclerostin inhibition should exclude inflammatory comorbidities and very thoroughly monitor inflammatory events in patients to which such therapies are applied,” the researchers advised.
In an editorial, Dr. Frank Rauch of McGill University, Montreal, and Dr. Rick Adachi of the department of rheumatology at McMaster University, Hamilton, Ont., wrote that antisclerostin “treatment might accelerate joint destruction, at least when the inflammatory process is not quelled first. Patients with established RA usually undergo anti-inflammatory treatment, and it is unclear whether sclerostin inactivation would be detrimental in this context. Mouse data suggest that antisclerostin treatment might bring about regression of bone erosions when combined with TNF-alpha inhibition. The new work mirrors the situation of patients who have unrecognized RA while on antisclerostin therapy or who develop RA while receiving this treatment” (Sci Transl Med. 2016 Mar 16;8:330fs7. doi: 10.1126/scitranslmed.aaf4628).
Antisclerostin antibodies in trials
Trials of the antisclerostin monoclonal antibodies romosozumab and blosozumab have been successful in treating postmenopausal women and men with osteoporosis.
Romosozumab codevelopers UCB and Amgen reported that the biologic agent significantly reduced the rate of new vertebral fractures by 73% versus placebo at 12 months in the randomized, double-blind phase III FRAME (Fracture Study in Postmenopausal Women With Osteoporosis) study. In the 7,180-patient trial, the reduction was 75% versus placebo at 24 months after both treatment groups had been transitioned to denosumab given every 6 months in the second year of treatment. Romosozumab also significantly lowered the relative risk of clinical fractures (composite of vertebral and nonvertebral fractures) by 36% at 12 months, but the difference was not statistically significant at 24 months.
In the initial 12-month treatment period, the most commonly reported adverse events in both arms (greater than 10%) were arthralgia, nasopharyngitis, and back pain. There were no differences in the proportions of patients who reported hearing loss or worsening of knee osteoarthritis. There were two positively adjudicated events of osteonecrosis of the jaw in the romosozumab treatment group, one after completing romosozumab dosing and the other after completing romosozumab treatment and receiving the initial dose of denosumab. There was one positively adjudicated event of atypical femoral fracture after 3 months of romosozumab treatment.
Phase III results from the 244-patient BRIDGE (Placebo-Controlled Study Evaluating the Efficacy and Safety of Romosozumab in Treating Men With Osteoporosis) trial found a significant increase in bone mineral density (BMD) at the lumbar spine at 12 months, which was the study’s primary endpoint. Other significant increases in femoral neck and total hip BMD were detected at 12 months. Cardiovascular severe adverse events occurred in 4.9% of men on romosozumab and 2.5% on placebo, including death in 0.6% and 1.2%, respectively. At least 5% or more of patients who received romosozumab reported nasopharyngitis, back pain, hypertension, headache, and constipation. About 5% of patients who received romosozumab in each trial had injection-site reactions, most of which were mild.
A phase II trial of blosozumab in 120 postmenopausal women with low bone mineral density (mean lumbar spine T-score –2.8) showed that the drug increased BMD in the lumbar spine by 17.7% above baseline at 52 weeks, femoral neck by 8.4%, and total hip by 6.2%, compared with decreases of 1.6%, 0.6%, and 0.7%, respectively, with placebo (J Bone Miner Res. 2015 Feb;30[2]:216-24). However, mild injection-site reactions were reported by up to 40% of women taking blosozumab, and 35% developed antidrug antibodies after exposure to blosozumab. Eli Lilly, its developer, is looking at possible ways to reformulate the drug before it moves to phase III.
The study in Science Translational Medicine was supported by the German Research Foundation. The authors had no competing interests to disclose.
Antisclerostin monoclonal antibodies have shown their ability to increase bone density in phase II and III trials of men and women with osteoporosis but could potentially have the opposite effect in patients with rheumatoid arthritis or other chronic inflammatory diseases in which tumor necrosis factor–alpha (TNF-alpha) plays an important role, according to new research.
The new work, conducted by Corinna Wehmeyer, Ph.D., of the Institute of Experimental Musculoskeletal Medicine at University Hospital Muenster (Germany) and her colleagues, shows that the bone formation–inhibiting protein sclerostin is not expressed in bone only, as was previously thought, but is also expressed on the synovial cells of patients with rheumatoid arthritis (RA).
Dr. Wehmeyer and her associates were surprised to find that inhibiting sclerostin in a human TNF-alpha transgenic mouse model of RA actually accelerated joint damage rather than prevented it, suggesting that sclerostin actually had a protective role in the presence of chronic TNF-alpha–mediated inflammation. They confirmed this by demonstrating that sclerostin inhibited TNF-alpha signaling in fibroblast-like synoviocytes and showing that blocking sclerostin caused less or little worsening of bone erosions in mouse models of RA that are more dependent on a robust T and B cell response accompanied by high cytokine expression within the joint, rather than damage driven by TNF-alpha.
“These findings strongly suggest that in chronic TNF-alpha–mediated inflammation, sclerostin expression is upregulated as part of an attempt to reestablish bone homeostasis, where it exerts protective functions,” the authors wrote (Sci Transl Med. 2016 Mar 16;8:330ra34. doi: 10.1126/scitranslmed.aac4351).
The research needs confirmation in humans with RA and potentially in other chronic inflammatory diseases in which TNF-alpha plays an important role. “Nevertheless, the preliminary data in three different models indicate that sclerostin antibody therapy could be contraindicated in patients with chronic TNF-alpha–dependent inflammatory conditions. The possibility of adverse pathological effects means that caution should be taken both when considering such treatment in RA or in patients with chronic TNF-alpha–dependent comorbidities. Thus, to translate these findings to patients, first strategies to use sclerostin inhibition should exclude inflammatory comorbidities and very thoroughly monitor inflammatory events in patients to which such therapies are applied,” the researchers advised.
In an editorial, Dr. Frank Rauch of McGill University, Montreal, and Dr. Rick Adachi of the department of rheumatology at McMaster University, Hamilton, Ont., wrote that antisclerostin “treatment might accelerate joint destruction, at least when the inflammatory process is not quelled first. Patients with established RA usually undergo anti-inflammatory treatment, and it is unclear whether sclerostin inactivation would be detrimental in this context. Mouse data suggest that antisclerostin treatment might bring about regression of bone erosions when combined with TNF-alpha inhibition. The new work mirrors the situation of patients who have unrecognized RA while on antisclerostin therapy or who develop RA while receiving this treatment” (Sci Transl Med. 2016 Mar 16;8:330fs7. doi: 10.1126/scitranslmed.aaf4628).
Antisclerostin antibodies in trials
Trials of the antisclerostin monoclonal antibodies romosozumab and blosozumab have been successful in treating postmenopausal women and men with osteoporosis.
Romosozumab codevelopers UCB and Amgen reported that the biologic agent significantly reduced the rate of new vertebral fractures by 73% versus placebo at 12 months in the randomized, double-blind phase III FRAME (Fracture Study in Postmenopausal Women With Osteoporosis) study. In the 7,180-patient trial, the reduction was 75% versus placebo at 24 months after both treatment groups had been transitioned to denosumab given every 6 months in the second year of treatment. Romosozumab also significantly lowered the relative risk of clinical fractures (composite of vertebral and nonvertebral fractures) by 36% at 12 months, but the difference was not statistically significant at 24 months.
In the initial 12-month treatment period, the most commonly reported adverse events in both arms (greater than 10%) were arthralgia, nasopharyngitis, and back pain. There were no differences in the proportions of patients who reported hearing loss or worsening of knee osteoarthritis. There were two positively adjudicated events of osteonecrosis of the jaw in the romosozumab treatment group, one after completing romosozumab dosing and the other after completing romosozumab treatment and receiving the initial dose of denosumab. There was one positively adjudicated event of atypical femoral fracture after 3 months of romosozumab treatment.
Phase III results from the 244-patient BRIDGE (Placebo-Controlled Study Evaluating the Efficacy and Safety of Romosozumab in Treating Men With Osteoporosis) trial found a significant increase in bone mineral density (BMD) at the lumbar spine at 12 months, which was the study’s primary endpoint. Other significant increases in femoral neck and total hip BMD were detected at 12 months. Cardiovascular severe adverse events occurred in 4.9% of men on romosozumab and 2.5% on placebo, including death in 0.6% and 1.2%, respectively. At least 5% or more of patients who received romosozumab reported nasopharyngitis, back pain, hypertension, headache, and constipation. About 5% of patients who received romosozumab in each trial had injection-site reactions, most of which were mild.
A phase II trial of blosozumab in 120 postmenopausal women with low bone mineral density (mean lumbar spine T-score –2.8) showed that the drug increased BMD in the lumbar spine by 17.7% above baseline at 52 weeks, femoral neck by 8.4%, and total hip by 6.2%, compared with decreases of 1.6%, 0.6%, and 0.7%, respectively, with placebo (J Bone Miner Res. 2015 Feb;30[2]:216-24). However, mild injection-site reactions were reported by up to 40% of women taking blosozumab, and 35% developed antidrug antibodies after exposure to blosozumab. Eli Lilly, its developer, is looking at possible ways to reformulate the drug before it moves to phase III.
The study in Science Translational Medicine was supported by the German Research Foundation. The authors had no competing interests to disclose.
Antisclerostin monoclonal antibodies have shown their ability to increase bone density in phase II and III trials of men and women with osteoporosis but could potentially have the opposite effect in patients with rheumatoid arthritis or other chronic inflammatory diseases in which tumor necrosis factor–alpha (TNF-alpha) plays an important role, according to new research.
The new work, conducted by Corinna Wehmeyer, Ph.D., of the Institute of Experimental Musculoskeletal Medicine at University Hospital Muenster (Germany) and her colleagues, shows that the bone formation–inhibiting protein sclerostin is not expressed in bone only, as was previously thought, but is also expressed on the synovial cells of patients with rheumatoid arthritis (RA).
Dr. Wehmeyer and her associates were surprised to find that inhibiting sclerostin in a human TNF-alpha transgenic mouse model of RA actually accelerated joint damage rather than prevented it, suggesting that sclerostin actually had a protective role in the presence of chronic TNF-alpha–mediated inflammation. They confirmed this by demonstrating that sclerostin inhibited TNF-alpha signaling in fibroblast-like synoviocytes and showing that blocking sclerostin caused less or little worsening of bone erosions in mouse models of RA that are more dependent on a robust T and B cell response accompanied by high cytokine expression within the joint, rather than damage driven by TNF-alpha.
“These findings strongly suggest that in chronic TNF-alpha–mediated inflammation, sclerostin expression is upregulated as part of an attempt to reestablish bone homeostasis, where it exerts protective functions,” the authors wrote (Sci Transl Med. 2016 Mar 16;8:330ra34. doi: 10.1126/scitranslmed.aac4351).
The research needs confirmation in humans with RA and potentially in other chronic inflammatory diseases in which TNF-alpha plays an important role. “Nevertheless, the preliminary data in three different models indicate that sclerostin antibody therapy could be contraindicated in patients with chronic TNF-alpha–dependent inflammatory conditions. The possibility of adverse pathological effects means that caution should be taken both when considering such treatment in RA or in patients with chronic TNF-alpha–dependent comorbidities. Thus, to translate these findings to patients, first strategies to use sclerostin inhibition should exclude inflammatory comorbidities and very thoroughly monitor inflammatory events in patients to which such therapies are applied,” the researchers advised.
In an editorial, Dr. Frank Rauch of McGill University, Montreal, and Dr. Rick Adachi of the department of rheumatology at McMaster University, Hamilton, Ont., wrote that antisclerostin “treatment might accelerate joint destruction, at least when the inflammatory process is not quelled first. Patients with established RA usually undergo anti-inflammatory treatment, and it is unclear whether sclerostin inactivation would be detrimental in this context. Mouse data suggest that antisclerostin treatment might bring about regression of bone erosions when combined with TNF-alpha inhibition. The new work mirrors the situation of patients who have unrecognized RA while on antisclerostin therapy or who develop RA while receiving this treatment” (Sci Transl Med. 2016 Mar 16;8:330fs7. doi: 10.1126/scitranslmed.aaf4628).
Antisclerostin antibodies in trials
Trials of the antisclerostin monoclonal antibodies romosozumab and blosozumab have been successful in treating postmenopausal women and men with osteoporosis.
Romosozumab codevelopers UCB and Amgen reported that the biologic agent significantly reduced the rate of new vertebral fractures by 73% versus placebo at 12 months in the randomized, double-blind phase III FRAME (Fracture Study in Postmenopausal Women With Osteoporosis) study. In the 7,180-patient trial, the reduction was 75% versus placebo at 24 months after both treatment groups had been transitioned to denosumab given every 6 months in the second year of treatment. Romosozumab also significantly lowered the relative risk of clinical fractures (composite of vertebral and nonvertebral fractures) by 36% at 12 months, but the difference was not statistically significant at 24 months.
In the initial 12-month treatment period, the most commonly reported adverse events in both arms (greater than 10%) were arthralgia, nasopharyngitis, and back pain. There were no differences in the proportions of patients who reported hearing loss or worsening of knee osteoarthritis. There were two positively adjudicated events of osteonecrosis of the jaw in the romosozumab treatment group, one after completing romosozumab dosing and the other after completing romosozumab treatment and receiving the initial dose of denosumab. There was one positively adjudicated event of atypical femoral fracture after 3 months of romosozumab treatment.
Phase III results from the 244-patient BRIDGE (Placebo-Controlled Study Evaluating the Efficacy and Safety of Romosozumab in Treating Men With Osteoporosis) trial found a significant increase in bone mineral density (BMD) at the lumbar spine at 12 months, which was the study’s primary endpoint. Other significant increases in femoral neck and total hip BMD were detected at 12 months. Cardiovascular severe adverse events occurred in 4.9% of men on romosozumab and 2.5% on placebo, including death in 0.6% and 1.2%, respectively. At least 5% or more of patients who received romosozumab reported nasopharyngitis, back pain, hypertension, headache, and constipation. About 5% of patients who received romosozumab in each trial had injection-site reactions, most of which were mild.
A phase II trial of blosozumab in 120 postmenopausal women with low bone mineral density (mean lumbar spine T-score –2.8) showed that the drug increased BMD in the lumbar spine by 17.7% above baseline at 52 weeks, femoral neck by 8.4%, and total hip by 6.2%, compared with decreases of 1.6%, 0.6%, and 0.7%, respectively, with placebo (J Bone Miner Res. 2015 Feb;30[2]:216-24). However, mild injection-site reactions were reported by up to 40% of women taking blosozumab, and 35% developed antidrug antibodies after exposure to blosozumab. Eli Lilly, its developer, is looking at possible ways to reformulate the drug before it moves to phase III.
The study in Science Translational Medicine was supported by the German Research Foundation. The authors had no competing interests to disclose.
FROM SCIENCE TRANSLATIONAL MEDICINE
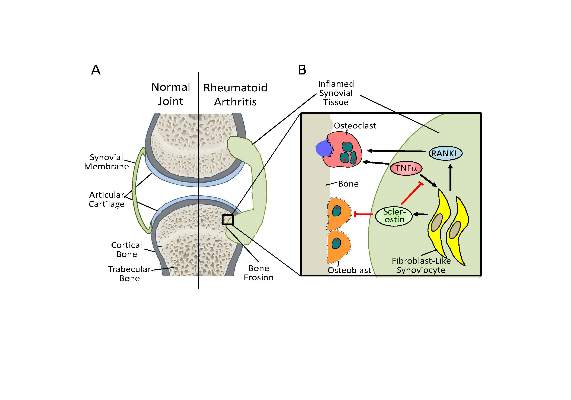
Confluent Erythematous Plaques on the Palm
The Diagnosis: Palmoplantar Lichen Planus
A skin biopsy from a lesion on the inner wrist showed an interface pattern with a dense bandlike infiltrate obscuring the dermoepidermal junction coupled with a superficial perivascular infiltrate (Figure). At higher magnification (×10), the histologic features included compact orthokeratosis, wedge-shaped hypergranulosis, vacuolar degeneration of the basal layer, basal dyskeratosis, a dense lymphohistiocytic infiltrate obscuring the basement membrane, and melanophages in the papillary dermis.
Lichen planus (LP) is a common inflammatory disease of the skin presenting with flat-topped, violaceous, polygonal papules with fine white lines (Wickham striae) on the surface. It is recognized and diagnosed clinically by its characteristic appearance. Common areas of LP presentation include the shins, inner thighs, genitalia, trunk, volar aspect of the wrists, and oral mucosa.
Palmoplantar LP can present as erythematous plaques, punctuate keratosis, diffuse keratoderma, or ulcerated lesions. The most common concern among patients with LP is pruritus. One-fourth of patients with LP may present with lesions on the palms and soles, but diffuse palmoplantar hyperkeratosis is rare.1 Lesions typically heal in 1 to 8 months, with an average of 3 months. Palmoplantar LP recurs within 1 year after stopping treatment in one-third of patients.1
The cause of LP is unknown, but the pathophysiology is beginning to be understood. Cytotoxic CD8+ T cells stimulate apoptosis of the keratinocytes. The induction of this mechanism may be due to a self-antigen in a genetically predisposed patient. The evidence for LP being an autoimmune disease is supported by the high female predominance and the association of LP with other autoimmune diseases.2 Patients with LP have an increased chance of coexisting hepatitis C virus. In a cross-sectional study of 303 patients, Lodi et al3 found that approximately 20% of LP patients were hepatitis C virus seropositive.
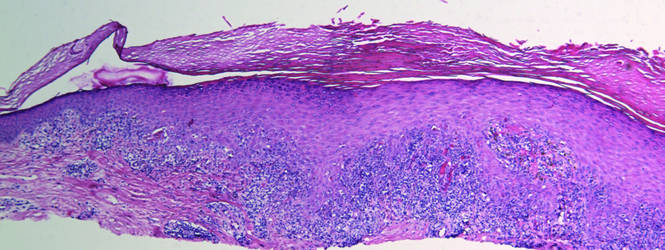
Treatment options for LP include topical and systemic steroids, tazarotene, acitretin, and immunosuppressive agents.4 Our patient initially was treated with oral cyclosporine 100 mg every morning and oral methotrexate at a dose of 7.5 mg weekly. She also was treated with clobetasol ointment 0.05%. After 3 months, cyclosporine was discontinued. Methotrexate was maintained. At 5 months’ followup there was marked improvement of both clinical and symptomatic concerns with only residual palmoplantar erythema.
The differential diagnosis for pruritic palmoplantar hyperkeratosis is large. The most common differential diagnoses include hyperkeratotic eczema, psoriasis, secondary syphilis, and hereditary palmoplantar keratoderma. Lichen planus should be considered in the differential diagnosis of palmoplantar hyperkeratosis. A skin biopsy may be needed, as palmoplantar LP often has an atypical presentation.5
1. Sánchez-Pérez J, Rios Buceta L, Fraga J, et al. Lichen planus with lesions on the palms and/or soles: prevalence and clinicopathological study of 36 patients. Br J Dermatol. 2000;142:310-314.
2. Farhi D, Dupin N. Pathophysiology, etiologic factors, and clinical management of oral lichen planus, part I: facts and controversies. Clin Dermatol. 2010;28:100-108.
3. Lodi G, Giuliani M, Majorana A, et al. Lichen planus and hepatitis C virus: a multicentre study of patients with oral lesions and a systematic review. Br J Dermatol. 2004;151:1172-1181.
4. Karakatsanis G, Patsatsi A, Kastoridou C, et al. Palmoplantar lichen planus with umbilicated papules: an atypical case with rapid therapeutic response to cyclosporin. J Eur Acad Dermatol Venereol. 2007;21:1006-1007.
5. Rotunda AM, Craft N, Haley JC. Hyperkeratotic plaques on the palms and soles. palmoplantar lichen planus, hyperkeratotic variant. Arch Dermatol. 2004;140:1275-1280.
The Diagnosis: Palmoplantar Lichen Planus
A skin biopsy from a lesion on the inner wrist showed an interface pattern with a dense bandlike infiltrate obscuring the dermoepidermal junction coupled with a superficial perivascular infiltrate (Figure). At higher magnification (×10), the histologic features included compact orthokeratosis, wedge-shaped hypergranulosis, vacuolar degeneration of the basal layer, basal dyskeratosis, a dense lymphohistiocytic infiltrate obscuring the basement membrane, and melanophages in the papillary dermis.
Lichen planus (LP) is a common inflammatory disease of the skin presenting with flat-topped, violaceous, polygonal papules with fine white lines (Wickham striae) on the surface. It is recognized and diagnosed clinically by its characteristic appearance. Common areas of LP presentation include the shins, inner thighs, genitalia, trunk, volar aspect of the wrists, and oral mucosa.
Palmoplantar LP can present as erythematous plaques, punctuate keratosis, diffuse keratoderma, or ulcerated lesions. The most common concern among patients with LP is pruritus. One-fourth of patients with LP may present with lesions on the palms and soles, but diffuse palmoplantar hyperkeratosis is rare.1 Lesions typically heal in 1 to 8 months, with an average of 3 months. Palmoplantar LP recurs within 1 year after stopping treatment in one-third of patients.1
The cause of LP is unknown, but the pathophysiology is beginning to be understood. Cytotoxic CD8+ T cells stimulate apoptosis of the keratinocytes. The induction of this mechanism may be due to a self-antigen in a genetically predisposed patient. The evidence for LP being an autoimmune disease is supported by the high female predominance and the association of LP with other autoimmune diseases.2 Patients with LP have an increased chance of coexisting hepatitis C virus. In a cross-sectional study of 303 patients, Lodi et al3 found that approximately 20% of LP patients were hepatitis C virus seropositive.
Treatment options for LP include topical and systemic steroids, tazarotene, acitretin, and immunosuppressive agents.4 Our patient initially was treated with oral cyclosporine 100 mg every morning and oral methotrexate at a dose of 7.5 mg weekly. She also was treated with clobetasol ointment 0.05%. After 3 months, cyclosporine was discontinued. Methotrexate was maintained. At 5 months’ followup there was marked improvement of both clinical and symptomatic concerns with only residual palmoplantar erythema.
The differential diagnosis for pruritic palmoplantar hyperkeratosis is large. The most common differential diagnoses include hyperkeratotic eczema, psoriasis, secondary syphilis, and hereditary palmoplantar keratoderma. Lichen planus should be considered in the differential diagnosis of palmoplantar hyperkeratosis. A skin biopsy may be needed, as palmoplantar LP often has an atypical presentation.5
The Diagnosis: Palmoplantar Lichen Planus
A skin biopsy from a lesion on the inner wrist showed an interface pattern with a dense bandlike infiltrate obscuring the dermoepidermal junction coupled with a superficial perivascular infiltrate (Figure). At higher magnification (×10), the histologic features included compact orthokeratosis, wedge-shaped hypergranulosis, vacuolar degeneration of the basal layer, basal dyskeratosis, a dense lymphohistiocytic infiltrate obscuring the basement membrane, and melanophages in the papillary dermis.
Lichen planus (LP) is a common inflammatory disease of the skin presenting with flat-topped, violaceous, polygonal papules with fine white lines (Wickham striae) on the surface. It is recognized and diagnosed clinically by its characteristic appearance. Common areas of LP presentation include the shins, inner thighs, genitalia, trunk, volar aspect of the wrists, and oral mucosa.
Palmoplantar LP can present as erythematous plaques, punctuate keratosis, diffuse keratoderma, or ulcerated lesions. The most common concern among patients with LP is pruritus. One-fourth of patients with LP may present with lesions on the palms and soles, but diffuse palmoplantar hyperkeratosis is rare.1 Lesions typically heal in 1 to 8 months, with an average of 3 months. Palmoplantar LP recurs within 1 year after stopping treatment in one-third of patients.1
The cause of LP is unknown, but the pathophysiology is beginning to be understood. Cytotoxic CD8+ T cells stimulate apoptosis of the keratinocytes. The induction of this mechanism may be due to a self-antigen in a genetically predisposed patient. The evidence for LP being an autoimmune disease is supported by the high female predominance and the association of LP with other autoimmune diseases.2 Patients with LP have an increased chance of coexisting hepatitis C virus. In a cross-sectional study of 303 patients, Lodi et al3 found that approximately 20% of LP patients were hepatitis C virus seropositive.
Treatment options for LP include topical and systemic steroids, tazarotene, acitretin, and immunosuppressive agents.4 Our patient initially was treated with oral cyclosporine 100 mg every morning and oral methotrexate at a dose of 7.5 mg weekly. She also was treated with clobetasol ointment 0.05%. After 3 months, cyclosporine was discontinued. Methotrexate was maintained. At 5 months’ followup there was marked improvement of both clinical and symptomatic concerns with only residual palmoplantar erythema.
The differential diagnosis for pruritic palmoplantar hyperkeratosis is large. The most common differential diagnoses include hyperkeratotic eczema, psoriasis, secondary syphilis, and hereditary palmoplantar keratoderma. Lichen planus should be considered in the differential diagnosis of palmoplantar hyperkeratosis. A skin biopsy may be needed, as palmoplantar LP often has an atypical presentation.5
1. Sánchez-Pérez J, Rios Buceta L, Fraga J, et al. Lichen planus with lesions on the palms and/or soles: prevalence and clinicopathological study of 36 patients. Br J Dermatol. 2000;142:310-314.
2. Farhi D, Dupin N. Pathophysiology, etiologic factors, and clinical management of oral lichen planus, part I: facts and controversies. Clin Dermatol. 2010;28:100-108.
3. Lodi G, Giuliani M, Majorana A, et al. Lichen planus and hepatitis C virus: a multicentre study of patients with oral lesions and a systematic review. Br J Dermatol. 2004;151:1172-1181.
4. Karakatsanis G, Patsatsi A, Kastoridou C, et al. Palmoplantar lichen planus with umbilicated papules: an atypical case with rapid therapeutic response to cyclosporin. J Eur Acad Dermatol Venereol. 2007;21:1006-1007.
5. Rotunda AM, Craft N, Haley JC. Hyperkeratotic plaques on the palms and soles. palmoplantar lichen planus, hyperkeratotic variant. Arch Dermatol. 2004;140:1275-1280.
1. Sánchez-Pérez J, Rios Buceta L, Fraga J, et al. Lichen planus with lesions on the palms and/or soles: prevalence and clinicopathological study of 36 patients. Br J Dermatol. 2000;142:310-314.
2. Farhi D, Dupin N. Pathophysiology, etiologic factors, and clinical management of oral lichen planus, part I: facts and controversies. Clin Dermatol. 2010;28:100-108.
3. Lodi G, Giuliani M, Majorana A, et al. Lichen planus and hepatitis C virus: a multicentre study of patients with oral lesions and a systematic review. Br J Dermatol. 2004;151:1172-1181.
4. Karakatsanis G, Patsatsi A, Kastoridou C, et al. Palmoplantar lichen planus with umbilicated papules: an atypical case with rapid therapeutic response to cyclosporin. J Eur Acad Dermatol Venereol. 2007;21:1006-1007.
5. Rotunda AM, Craft N, Haley JC. Hyperkeratotic plaques on the palms and soles. palmoplantar lichen planus, hyperkeratotic variant. Arch Dermatol. 2004;140:1275-1280.

A 45-year-old woman was referred to dermatology by her general internist for the management of a pruritic rash on the hands and feet that was unresponsive to topical steroid creams. The pruritus also was unresponsive to hydroxyzine and aspirin. Erythematous plaques were present on the palms and soles. Physical examination revealed thickened volar skin with a yellowish surface. There were individual papules with atrophic tops at the edge of the plaques on the inner wrists. The patient’s medical history was otherwise unremarkable. Blood tests for glucose and liver function did not reveal any abnormalities.
