User login
Simple Tool Improves Communication Between Patients, Hospitalists
Hospitalists at the University of Michigan Health System in Ann Arbor have developed a tool to help facilitate patient communication with physicians and to "actively participate in their treatments," says Aaron Farberg, MD. "Their treatment plans will, in turn, be more effective," Dr. Farberg adds.
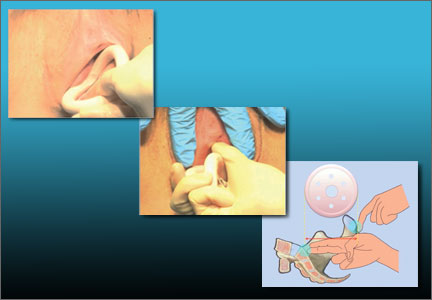
Called Dear Doctor (DD) notes, the tool is a pre-formatted notepad placed on a bedside table for hospital patients to consult throughout their stay. Patients can write down questions under three suggested prompts: diagnosis and treatment, tests and procedures, and medications. Such a simple tool is "absent in the inpatient setting, and can have an impact on a patient’s perceived and actual medical care," Dr. Farberg says.
Family members of patients can also benefit from DD notes by voicing their questions or concerns to the physicians. “Often their active participation in the healthcare plan is an essential element in successful treatment,” Dr. Farberg says.
Surveyed patients experienced better communication with hospitalists and had an enhanced experience with their providers and hospital. Patients and their families were happy their questions were answered and not forgotten. They had a sense of control and accountability in their own care. The study urges hospitalists and care providers to be mindful of the patient’s entire experience throughout hospital stay. TH
Visit our website for more information on hospitalists and patient communication.
Hospitalists at the University of Michigan Health System in Ann Arbor have developed a tool to help facilitate patient communication with physicians and to "actively participate in their treatments," says Aaron Farberg, MD. "Their treatment plans will, in turn, be more effective," Dr. Farberg adds.
Called Dear Doctor (DD) notes, the tool is a pre-formatted notepad placed on a bedside table for hospital patients to consult throughout their stay. Patients can write down questions under three suggested prompts: diagnosis and treatment, tests and procedures, and medications. Such a simple tool is "absent in the inpatient setting, and can have an impact on a patient’s perceived and actual medical care," Dr. Farberg says.
Family members of patients can also benefit from DD notes by voicing their questions or concerns to the physicians. “Often their active participation in the healthcare plan is an essential element in successful treatment,” Dr. Farberg says.
Surveyed patients experienced better communication with hospitalists and had an enhanced experience with their providers and hospital. Patients and their families were happy their questions were answered and not forgotten. They had a sense of control and accountability in their own care. The study urges hospitalists and care providers to be mindful of the patient’s entire experience throughout hospital stay. TH
Visit our website for more information on hospitalists and patient communication.
Hospitalists at the University of Michigan Health System in Ann Arbor have developed a tool to help facilitate patient communication with physicians and to "actively participate in their treatments," says Aaron Farberg, MD. "Their treatment plans will, in turn, be more effective," Dr. Farberg adds.
Called Dear Doctor (DD) notes, the tool is a pre-formatted notepad placed on a bedside table for hospital patients to consult throughout their stay. Patients can write down questions under three suggested prompts: diagnosis and treatment, tests and procedures, and medications. Such a simple tool is "absent in the inpatient setting, and can have an impact on a patient’s perceived and actual medical care," Dr. Farberg says.
Family members of patients can also benefit from DD notes by voicing their questions or concerns to the physicians. “Often their active participation in the healthcare plan is an essential element in successful treatment,” Dr. Farberg says.
Surveyed patients experienced better communication with hospitalists and had an enhanced experience with their providers and hospital. Patients and their families were happy their questions were answered and not forgotten. They had a sense of control and accountability in their own care. The study urges hospitalists and care providers to be mindful of the patient’s entire experience throughout hospital stay. TH
Visit our website for more information on hospitalists and patient communication.
Intravenous Haloperidol Does Not Prevent ICU Delirium
Clinical question: Can haloperidol reduce delirium in critically ill patients if initiated early in ICU stay?
Background: Prior studies suggest antipsychotics reduce intensity and duration of delirium in hospitalized patients. Evidence is mixed for preventing delirium. A trial of risperidone demonstrated delirium rate reduction in coronary artery bypass grafting (CABG) patients, but another trial of haloperidol in hip surgery patients failed to prevent onset of delirium. There is little evidence on antipsychotics in ICU delirium.
Study design: Randomized, double-blinded, placebo-controlled trial.
Setting: Single, adult ICU in England.
Synopsis: The study randomized 142 critically ill patients to receive 2.5 mg of intravenous haloperidol versus placebo every eight hours for up to 14 days. There was no significant difference between groups in the total time spent free of delirium or coma. Limitations include the use of open-label haloperidol in 21% of the placebo group patients. More sedation but less agitation was seen with the use of haloperidol, which also prolonged QTc. No severe adverse effects were observed.
This study supports the idea that scheduled antipsychotics should not be used to reduce ICU delirium. Addressing modifiable risk factors and using dexmedetomidine rather than lorazepam for sedation in the ICU continue to be first-line strategies to lower delirium rates.
Bottom line: Prophylactic haloperidol should not be used to prevent ICU delirium.
Citation: Page VJ, Ely EW, Gates S, et al. Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomized, double-blind, placebo-controlled trial. Lancet Respir Med. 2013;1(7):515-523.
Visit our website for more information on treating delirium in hospitalized patients.
Clinical question: Can haloperidol reduce delirium in critically ill patients if initiated early in ICU stay?
Background: Prior studies suggest antipsychotics reduce intensity and duration of delirium in hospitalized patients. Evidence is mixed for preventing delirium. A trial of risperidone demonstrated delirium rate reduction in coronary artery bypass grafting (CABG) patients, but another trial of haloperidol in hip surgery patients failed to prevent onset of delirium. There is little evidence on antipsychotics in ICU delirium.
Study design: Randomized, double-blinded, placebo-controlled trial.
Setting: Single, adult ICU in England.
Synopsis: The study randomized 142 critically ill patients to receive 2.5 mg of intravenous haloperidol versus placebo every eight hours for up to 14 days. There was no significant difference between groups in the total time spent free of delirium or coma. Limitations include the use of open-label haloperidol in 21% of the placebo group patients. More sedation but less agitation was seen with the use of haloperidol, which also prolonged QTc. No severe adverse effects were observed.
This study supports the idea that scheduled antipsychotics should not be used to reduce ICU delirium. Addressing modifiable risk factors and using dexmedetomidine rather than lorazepam for sedation in the ICU continue to be first-line strategies to lower delirium rates.
Bottom line: Prophylactic haloperidol should not be used to prevent ICU delirium.
Citation: Page VJ, Ely EW, Gates S, et al. Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomized, double-blind, placebo-controlled trial. Lancet Respir Med. 2013;1(7):515-523.
Visit our website for more information on treating delirium in hospitalized patients.
Clinical question: Can haloperidol reduce delirium in critically ill patients if initiated early in ICU stay?
Background: Prior studies suggest antipsychotics reduce intensity and duration of delirium in hospitalized patients. Evidence is mixed for preventing delirium. A trial of risperidone demonstrated delirium rate reduction in coronary artery bypass grafting (CABG) patients, but another trial of haloperidol in hip surgery patients failed to prevent onset of delirium. There is little evidence on antipsychotics in ICU delirium.
Study design: Randomized, double-blinded, placebo-controlled trial.
Setting: Single, adult ICU in England.
Synopsis: The study randomized 142 critically ill patients to receive 2.5 mg of intravenous haloperidol versus placebo every eight hours for up to 14 days. There was no significant difference between groups in the total time spent free of delirium or coma. Limitations include the use of open-label haloperidol in 21% of the placebo group patients. More sedation but less agitation was seen with the use of haloperidol, which also prolonged QTc. No severe adverse effects were observed.
This study supports the idea that scheduled antipsychotics should not be used to reduce ICU delirium. Addressing modifiable risk factors and using dexmedetomidine rather than lorazepam for sedation in the ICU continue to be first-line strategies to lower delirium rates.
Bottom line: Prophylactic haloperidol should not be used to prevent ICU delirium.
Citation: Page VJ, Ely EW, Gates S, et al. Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomized, double-blind, placebo-controlled trial. Lancet Respir Med. 2013;1(7):515-523.
Visit our website for more information on treating delirium in hospitalized patients.
Hyperglycemia, Hypoglycemia Challenge Hospitalists Equally
Glycemic control in hospitalized patients is possible without having to achieve the much-debated standard of intensive glycemic control. That’s what Irl Hirsch, MD, professor of medicine at the University of Washington in Seattle, said in a presentation on management of diabetes in the hospitalized patient at the UCSF conference.
“We instituted intravenous insulin protocols throughout our hospital in 1992,” before recent medical controversies about IGC, Dr. Hirsch said. Eventually, a target weight dimension of 100 to 180 mg/dL of blood glucose became the hospital standard.
The number of hospitalized patients with diabetes increased 93% between 1988 and 2009. Many hospitalists encounter diabetics and order insulin for them every day, Dr. Hirsch said. Although hyperglycemia, which is seen in 78% of hospitalized patients with diabetes and 26% of those without, is linked to mortality regardless of diabetic status, mortality is greater in patients with diabetes, especially in those newly diagnosed with hyperglycemia, Dr. Hirsch said.1 Hypoglycemia often is overlooked due to 
Doctors need to find a safe middle ground, he said, noting that intensive insulin therapy has not been shown to improve major outcomes, including ICU mortality. “The real danger is that we can’t get glucose under tight control without risking hypoglycemia,” he said. “We’ve had almost no hypoglycemia in our hospital for the past couple of years.”
In his talk, Dr. Hirsch took particular issue with the persistence of “sliding scale” approaches to titrating insulin therapy in hospitalized patients, basing the amount of insulin on current glucose level but not taking into consideration how long previous insulin treatments might be active or whether the insulin is “stacking” in the patient’s bloodstream. “The sliding scale doesn’t work. It’s dangerous, and that’s why I’m on this crusade,” he stated. Over time, basal bolus administration works better, Dr. Hirsch said, adding that continued improvements in the technology of continuous glucose monitoring will help to put an end to the controversy. TH
Larry Beresford is a freelance writer in San Franscisco.
Reference
1. Kosiborod M, Inzucchi S, Clark B, et al. National patterns of glucose control among patients hospitalized with acute myocardial infarction. J Am Coll Cardiol. 2007;49:1018–1183:1283A.
Glycemic control in hospitalized patients is possible without having to achieve the much-debated standard of intensive glycemic control. That’s what Irl Hirsch, MD, professor of medicine at the University of Washington in Seattle, said in a presentation on management of diabetes in the hospitalized patient at the UCSF conference.
“We instituted intravenous insulin protocols throughout our hospital in 1992,” before recent medical controversies about IGC, Dr. Hirsch said. Eventually, a target weight dimension of 100 to 180 mg/dL of blood glucose became the hospital standard.
The number of hospitalized patients with diabetes increased 93% between 1988 and 2009. Many hospitalists encounter diabetics and order insulin for them every day, Dr. Hirsch said. Although hyperglycemia, which is seen in 78% of hospitalized patients with diabetes and 26% of those without, is linked to mortality regardless of diabetic status, mortality is greater in patients with diabetes, especially in those newly diagnosed with hyperglycemia, Dr. Hirsch said.1 Hypoglycemia often is overlooked due to
Doctors need to find a safe middle ground, he said, noting that intensive insulin therapy has not been shown to improve major outcomes, including ICU mortality. “The real danger is that we can’t get glucose under tight control without risking hypoglycemia,” he said. “We’ve had almost no hypoglycemia in our hospital for the past couple of years.”
In his talk, Dr. Hirsch took particular issue with the persistence of “sliding scale” approaches to titrating insulin therapy in hospitalized patients, basing the amount of insulin on current glucose level but not taking into consideration how long previous insulin treatments might be active or whether the insulin is “stacking” in the patient’s bloodstream. “The sliding scale doesn’t work. It’s dangerous, and that’s why I’m on this crusade,” he stated. Over time, basal bolus administration works better, Dr. Hirsch said, adding that continued improvements in the technology of continuous glucose monitoring will help to put an end to the controversy. TH
Larry Beresford is a freelance writer in San Franscisco.
Reference
1. Kosiborod M, Inzucchi S, Clark B, et al. National patterns of glucose control among patients hospitalized with acute myocardial infarction. J Am Coll Cardiol. 2007;49:1018–1183:1283A.
Glycemic control in hospitalized patients is possible without having to achieve the much-debated standard of intensive glycemic control. That’s what Irl Hirsch, MD, professor of medicine at the University of Washington in Seattle, said in a presentation on management of diabetes in the hospitalized patient at the UCSF conference.
“We instituted intravenous insulin protocols throughout our hospital in 1992,” before recent medical controversies about IGC, Dr. Hirsch said. Eventually, a target weight dimension of 100 to 180 mg/dL of blood glucose became the hospital standard.
The number of hospitalized patients with diabetes increased 93% between 1988 and 2009. Many hospitalists encounter diabetics and order insulin for them every day, Dr. Hirsch said. Although hyperglycemia, which is seen in 78% of hospitalized patients with diabetes and 26% of those without, is linked to mortality regardless of diabetic status, mortality is greater in patients with diabetes, especially in those newly diagnosed with hyperglycemia, Dr. Hirsch said.1 Hypoglycemia often is overlooked due to
Doctors need to find a safe middle ground, he said, noting that intensive insulin therapy has not been shown to improve major outcomes, including ICU mortality. “The real danger is that we can’t get glucose under tight control without risking hypoglycemia,” he said. “We’ve had almost no hypoglycemia in our hospital for the past couple of years.”
In his talk, Dr. Hirsch took particular issue with the persistence of “sliding scale” approaches to titrating insulin therapy in hospitalized patients, basing the amount of insulin on current glucose level but not taking into consideration how long previous insulin treatments might be active or whether the insulin is “stacking” in the patient’s bloodstream. “The sliding scale doesn’t work. It’s dangerous, and that’s why I’m on this crusade,” he stated. Over time, basal bolus administration works better, Dr. Hirsch said, adding that continued improvements in the technology of continuous glucose monitoring will help to put an end to the controversy. TH
Larry Beresford is a freelance writer in San Franscisco.
Reference
1. Kosiborod M, Inzucchi S, Clark B, et al. National patterns of glucose control among patients hospitalized with acute myocardial infarction. J Am Coll Cardiol. 2007;49:1018–1183:1283A.
Thinking about the institution of marriage – Part I
Throughout history, views of marriage have evolved as societies change. Since the 6th century, the Roman Catholic Church has played a prominent role in thinking and developing our ideas about marriage and family. In October, the church sent out a document that included a questionnaire to its bishops around the world to find out what Catholics think about the "modern family." The Vatican sent out the document in preparation for the Synod of Bishops on the Family, which is slated for October 2014. Before we get the results, let’s review how society has reflected on marriage and family.
Historically, marriages often were strategic alliances between families. It was common for marriage to be between first and second cousins in order to strengthen family ties. Polygamy has been common throughout history and continues in many communities to this day.
Monogamy is also found throughout history, but in 1215, the Catholic Church decreed that partners had to publicly post notices of an impending marriage in a local parish to cut down on the number of invalid marriages. Until the 1500s, the Catholic Church accepted a couple’s word that they had exchanged marriage vows, with no witnesses or corroborating evidence needed. In the 1500s, with the rise in Protestantism, marriage became a civil matter rather than a sacrament. By 1639, states such as Massachusetts began requiring marriage licenses, and by the 19th century, marriage licenses were common in the United States.
Marriage through the ages
Here is a listing of the way in which marriage has been conceptualized over the years:
Arranged alliances: A strategic alliance between families.
Family ties: Keeping alliances within the family; the majority of all marriages throughout history were between first and second cousins.
Polygamy: A phenomenon that has been common throughout history.
Babies optional: In many early cultures, men could dissolve a marriage or take another wife if a woman was infertile. However, the early Christian church was a trailblazer in arguing that marriage was not contingent upon producing offspring.
Monogamy: This practice became the guiding principle for Western marriages between the 6th and 9th centuries because of the church.
Sacred vs. secular: In 1215, the Roman Catholic Church decreed that partners had to publicly post notices, or banns, of an impending marriage in a local parish in order to cut down on the number of invalid marriages. Until the 1500s, the church accepted a couple’s word that they had exchanged marriage vows, with no witnesses or corroborating evidence needed.
Civil marriage: By 1639, states such as Massachusetts began requiring marriage licenses and, by the 19th century, marriage licenses were common in the United States.
Romance: By the 1900s, mutual attraction became important.
Market economics: Families historically controlled access to inheritance of agricultural land, but with the spread of a market economy, it becomes possible for people to marry outside of this inheritance.
Women’s equality: About 50 years ago, in Western countries, women and men began to have equal rights and responsibilities. Instead of being about unique, gender-based roles, most partners conceived of their unions in terms of flexible divisions of labor, companionship, and mutual sexual attraction.
Same-sex marriages: One of the reasons for the stunningly rapid increase in acceptance of same-sex marriage is because heterosexuals have completely changed their notion that all marriages are between a man and a woman, notes Stephanie Coontz, Ph.D. "We now believe marriage is based on love, mutual sexual attraction, equality, and a flexible division of labor."
Source: Adapted from "Marriage, a History: From Obedience to Intimacy, or How Love Conquered Marriage," (New York: Viking, 2005), by Dr. Coontz.
A sacred view of marriage
The Catholic position throughout history has been that marriage is one of the seven sacraments bestowed by Christ. This questionnaire is an attempt by the Vatican to understand more about "mixed or interreligious marriages; the single-parent family; polygamy; marriages with the consequent problem of a dowry, sometimes understood as the purchase price of the woman; the caste system; a culture of noncommitment and a presumption that the marriage bond can be temporary; forms of feminism hostile to the Church; migration and the reformulation of the very concept of the family; relativist pluralism in the conception of marriage; the influence of the media on popular culture in its understanding of marriage and family life; underlying trends of thought in legislative proposals which devalue the idea of permanence and faithfulness in the marriage covenant; an increase in the practice of surrogate motherhood (wombs for hire); and new interpretations of what is considered a human right."
Thirty-nine questions are on the questionnaire. Questions 4, 5, and 6 are of most interest to family psychiatrists. Deserving of admiration is its concern for families in migration and for the mistreatment of women.
The terms "regular" and "irregular," used in the questionnaire, are canonical terms unrelated to what actually happens in any given society. It should also be explained that Catholics who married always had to declare that they would welcome such children as God happened to send along, recognizing that he might choose not to send any. A decision to refuse to accept the possibility of children invalidated the marriage vows and constitutes grounds for annulment.
Excerpts from the Vatican document
Questions 4, 5, and 6 of the Vatican’s questionnaire seem aimed at gathering data on different kinds of families. Here are those three questions:
Pastoral Care in Certain Difficult Marital Situations
a) Is cohabitation ad experimentum a pastoral reality in your particular Church? Can you approximate a percentage?
b) Do unions which are not recognized either religiously or civilly exist? Are reliable statistics available?
c) Are separated couples and those divorced and remarried a pastoral reality in your particular Church? Can you approximate a percentage? How do you deal with this situation in appropriate pastoral programmes? (sic)
d) In all the above cases, how do the baptized live in this irregular situation? Are they aware of it? Are they simply indifferent? Do they feel marginalized or suffer from the impossibility of receiving the sacraments?
f) Could a simplification of canonical practice in recognizing a declaration of nullity of the marriage bond provide a positive contribution to solving the problems of the persons involved? If yes, what form would it take?
Does a ministry exist to attend to these cases? Describe this pastoral ministry? Do such programmes exist on the national and diocesan levels? How is God’s mercy proclaimed to separated couples and those divorced and remarried, and how does the Church put into practice her support for them in their journey of faith?
On Unions of Persons of the Same Sex
a) Is there a law in your country recognizing civil unions for people of the same-sex and equating it in some way to marriage?
b) What is the attitude of the local and particular Churches towards both the State as the promoter of civil unions between persons of the same sex and the people involved in this type of union?
c) What pastoral attention can be given to people who have chosen to live in these types of union?
In the case of unions of persons of the same sex who have adopted children, what can be done pastorally in light of transmitting the faith?
The Education of Children in Irregular Marriages
a) What is the estimated proportion of children and adolescents in these cases, as regards children who are born and raised in regularly constituted families?
b) How do parents in these situations approach the Church? What do they ask? Do they request the sacraments only or do they also want catechesis and the general teaching of religion?
c) How do the particular Churches attempt to meet the needs of the parents of these children to provide them with a Christian education?
Source: Pastoral Challenges to the Family in the Context of Evangelization
A secular view of marriage
A secular view of marriage has been advanced by economists Betsey Stevenson, Ph.D., and Justin Wolfers, Ph.D., who describe the extent to which marriage is shaped by economic forces. "Productive marriage" is based on a division of labor. In the earlier part of the 20th century in Western countries, school, education, and the emerging TV and magazine markets illustrated how women could be good homemakers and men could be good providers. The liberation of women through education and access to birth control changed the playing field. Prior to this, college-educated women were the least likely to marry. Since the 1960s and 1970s, educated women could prevent pregnancy and support themselves, and found little use for the previous productive model of marriage.
Men, also, did not see educated, financially independent women as suitable marriage partners. The high divorce rate among those who married in the1970s reflected discontent with this model of the productive marriage.
In contrast, Dr. Stevenson and Dr. Wolfers write, "hedonic marriage" occurs when people who marry are of similar age, educational background, and perhaps occupation. The hedonic marriage better suits educated women who seek a companion, and it thrives when time and resources are available to enjoy companionable life. Same-sex marriages make sense when considered in this broad frame. Supporting this concept is the fact that couples who have married in recent years are more likely to stay together than were their parents’ generation. Of course, this discourse is only relevant in parts of the world in which women have access to birth control and opportunities for education, work, and social standing.
Romance and marriage
The question of romance in marriage is the hardest for psychiatrists, as scientists, to address. Romance has always been around, sometimes present in marriages and sometimes not. Romance is thought to be both essential and nonessential to marriage, depending on the purpose of the marriage. A good discussion by Dr. Henry Grunebaum can be found an article titled "Thinking about romantic/erotic love" in the Journal of Marital and Family Therapy(1997;23:295-307). His main points are that we do not have control over our feelings of romantic/erotic love, that these feelings occur relatively infrequently during most people’s lives, that being with a partner whom one loves, is valued and regarded as a good, that it sometimes conflicts with other values and goods, and lastly that although love is regarded as one essential basis for marriage, other qualities and capacities are important in sustaining a long-term relationship such as a marriage. He concludes with, "What makes matters even more challenging is the fact that we ask a great deal of marriage, of any serious intimate relationship. Perhaps the greatest demand we make is that it should combine passion and stability, romance and monogamy, transports of tenderness and excitement from the person who will also perform the many mundane tasks of daily living. In other words, meld everyday love with romantic/erotic love." He offers suggestions for discussion and guidelines for therapists.
Applying all of this in our work
As family psychiatrists, we can allow couples and families a therapeutic space to discuss the meaning and assumptions in their marriage. We can discuss the frame of the marriage: Is it sacred, secular, or postmodern? In this way, we can provide a context to the current struggles that couples and families might have.
To begin, we can ask about the past. We can say, "People get married for different reasons. What were your reasons? Do you consider your marriage to be a sacred or a secular? What does this mean to you?"
Delving deeper and focusing more on the present, "What is your current experience of your marriage? How do your expectations differ now than from your expectations in the past? What is the role of romance in your marriage?
What type of marriage did you want when you began this marriage? Is there romance in your marriage? What kind of marriage do you want now?
Focusing on going forward we can ask: "What works well in your marriage/family? What are your strengths? What needs to change in your marriage?"
In the late 1970s, postmodernism emerged in the world. Postmodernism stands in contrast to the "modern" or scientific view that touts a singularity of truth and a singular view of the world. Social construction is a type of postmodern theory that states that truth, reality, and knowledge are based in the social context of that particular person. Inevitably, postmodernism affects how we think about and conceptualize marriage. Postmodernism and marriage will be the subject of the next column.
I would like to thank Peter Chaloner, M.A., LL.B, B.A. (Honors), and Dip. Theo., for his comments and corrections.
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals" (New York: Routledge, 2013).
Throughout history, views of marriage have evolved as societies change. Since the 6th century, the Roman Catholic Church has played a prominent role in thinking and developing our ideas about marriage and family. In October, the church sent out a document that included a questionnaire to its bishops around the world to find out what Catholics think about the "modern family." The Vatican sent out the document in preparation for the Synod of Bishops on the Family, which is slated for October 2014. Before we get the results, let’s review how society has reflected on marriage and family.
Historically, marriages often were strategic alliances between families. It was common for marriage to be between first and second cousins in order to strengthen family ties. Polygamy has been common throughout history and continues in many communities to this day.
Monogamy is also found throughout history, but in 1215, the Catholic Church decreed that partners had to publicly post notices of an impending marriage in a local parish to cut down on the number of invalid marriages. Until the 1500s, the Catholic Church accepted a couple’s word that they had exchanged marriage vows, with no witnesses or corroborating evidence needed. In the 1500s, with the rise in Protestantism, marriage became a civil matter rather than a sacrament. By 1639, states such as Massachusetts began requiring marriage licenses, and by the 19th century, marriage licenses were common in the United States.
Marriage through the ages
Here is a listing of the way in which marriage has been conceptualized over the years:
Arranged alliances: A strategic alliance between families.
Family ties: Keeping alliances within the family; the majority of all marriages throughout history were between first and second cousins.
Polygamy: A phenomenon that has been common throughout history.
Babies optional: In many early cultures, men could dissolve a marriage or take another wife if a woman was infertile. However, the early Christian church was a trailblazer in arguing that marriage was not contingent upon producing offspring.
Monogamy: This practice became the guiding principle for Western marriages between the 6th and 9th centuries because of the church.
Sacred vs. secular: In 1215, the Roman Catholic Church decreed that partners had to publicly post notices, or banns, of an impending marriage in a local parish in order to cut down on the number of invalid marriages. Until the 1500s, the church accepted a couple’s word that they had exchanged marriage vows, with no witnesses or corroborating evidence needed.
Civil marriage: By 1639, states such as Massachusetts began requiring marriage licenses and, by the 19th century, marriage licenses were common in the United States.
Romance: By the 1900s, mutual attraction became important.
Market economics: Families historically controlled access to inheritance of agricultural land, but with the spread of a market economy, it becomes possible for people to marry outside of this inheritance.
Women’s equality: About 50 years ago, in Western countries, women and men began to have equal rights and responsibilities. Instead of being about unique, gender-based roles, most partners conceived of their unions in terms of flexible divisions of labor, companionship, and mutual sexual attraction.
Same-sex marriages: One of the reasons for the stunningly rapid increase in acceptance of same-sex marriage is because heterosexuals have completely changed their notion that all marriages are between a man and a woman, notes Stephanie Coontz, Ph.D. "We now believe marriage is based on love, mutual sexual attraction, equality, and a flexible division of labor."
Source: Adapted from "Marriage, a History: From Obedience to Intimacy, or How Love Conquered Marriage," (New York: Viking, 2005), by Dr. Coontz.
A sacred view of marriage
The Catholic position throughout history has been that marriage is one of the seven sacraments bestowed by Christ. This questionnaire is an attempt by the Vatican to understand more about "mixed or interreligious marriages; the single-parent family; polygamy; marriages with the consequent problem of a dowry, sometimes understood as the purchase price of the woman; the caste system; a culture of noncommitment and a presumption that the marriage bond can be temporary; forms of feminism hostile to the Church; migration and the reformulation of the very concept of the family; relativist pluralism in the conception of marriage; the influence of the media on popular culture in its understanding of marriage and family life; underlying trends of thought in legislative proposals which devalue the idea of permanence and faithfulness in the marriage covenant; an increase in the practice of surrogate motherhood (wombs for hire); and new interpretations of what is considered a human right."
Thirty-nine questions are on the questionnaire. Questions 4, 5, and 6 are of most interest to family psychiatrists. Deserving of admiration is its concern for families in migration and for the mistreatment of women.
The terms "regular" and "irregular," used in the questionnaire, are canonical terms unrelated to what actually happens in any given society. It should also be explained that Catholics who married always had to declare that they would welcome such children as God happened to send along, recognizing that he might choose not to send any. A decision to refuse to accept the possibility of children invalidated the marriage vows and constitutes grounds for annulment.
Excerpts from the Vatican document
Questions 4, 5, and 6 of the Vatican’s questionnaire seem aimed at gathering data on different kinds of families. Here are those three questions:
Pastoral Care in Certain Difficult Marital Situations
a) Is cohabitation ad experimentum a pastoral reality in your particular Church? Can you approximate a percentage?
b) Do unions which are not recognized either religiously or civilly exist? Are reliable statistics available?
c) Are separated couples and those divorced and remarried a pastoral reality in your particular Church? Can you approximate a percentage? How do you deal with this situation in appropriate pastoral programmes? (sic)
d) In all the above cases, how do the baptized live in this irregular situation? Are they aware of it? Are they simply indifferent? Do they feel marginalized or suffer from the impossibility of receiving the sacraments?
f) Could a simplification of canonical practice in recognizing a declaration of nullity of the marriage bond provide a positive contribution to solving the problems of the persons involved? If yes, what form would it take?
Does a ministry exist to attend to these cases? Describe this pastoral ministry? Do such programmes exist on the national and diocesan levels? How is God’s mercy proclaimed to separated couples and those divorced and remarried, and how does the Church put into practice her support for them in their journey of faith?
On Unions of Persons of the Same Sex
a) Is there a law in your country recognizing civil unions for people of the same-sex and equating it in some way to marriage?
b) What is the attitude of the local and particular Churches towards both the State as the promoter of civil unions between persons of the same sex and the people involved in this type of union?
c) What pastoral attention can be given to people who have chosen to live in these types of union?
In the case of unions of persons of the same sex who have adopted children, what can be done pastorally in light of transmitting the faith?
The Education of Children in Irregular Marriages
a) What is the estimated proportion of children and adolescents in these cases, as regards children who are born and raised in regularly constituted families?
b) How do parents in these situations approach the Church? What do they ask? Do they request the sacraments only or do they also want catechesis and the general teaching of religion?
c) How do the particular Churches attempt to meet the needs of the parents of these children to provide them with a Christian education?
Source: Pastoral Challenges to the Family in the Context of Evangelization
A secular view of marriage
A secular view of marriage has been advanced by economists Betsey Stevenson, Ph.D., and Justin Wolfers, Ph.D., who describe the extent to which marriage is shaped by economic forces. "Productive marriage" is based on a division of labor. In the earlier part of the 20th century in Western countries, school, education, and the emerging TV and magazine markets illustrated how women could be good homemakers and men could be good providers. The liberation of women through education and access to birth control changed the playing field. Prior to this, college-educated women were the least likely to marry. Since the 1960s and 1970s, educated women could prevent pregnancy and support themselves, and found little use for the previous productive model of marriage.
Men, also, did not see educated, financially independent women as suitable marriage partners. The high divorce rate among those who married in the1970s reflected discontent with this model of the productive marriage.
In contrast, Dr. Stevenson and Dr. Wolfers write, "hedonic marriage" occurs when people who marry are of similar age, educational background, and perhaps occupation. The hedonic marriage better suits educated women who seek a companion, and it thrives when time and resources are available to enjoy companionable life. Same-sex marriages make sense when considered in this broad frame. Supporting this concept is the fact that couples who have married in recent years are more likely to stay together than were their parents’ generation. Of course, this discourse is only relevant in parts of the world in which women have access to birth control and opportunities for education, work, and social standing.
Romance and marriage
The question of romance in marriage is the hardest for psychiatrists, as scientists, to address. Romance has always been around, sometimes present in marriages and sometimes not. Romance is thought to be both essential and nonessential to marriage, depending on the purpose of the marriage. A good discussion by Dr. Henry Grunebaum can be found an article titled "Thinking about romantic/erotic love" in the Journal of Marital and Family Therapy(1997;23:295-307). His main points are that we do not have control over our feelings of romantic/erotic love, that these feelings occur relatively infrequently during most people’s lives, that being with a partner whom one loves, is valued and regarded as a good, that it sometimes conflicts with other values and goods, and lastly that although love is regarded as one essential basis for marriage, other qualities and capacities are important in sustaining a long-term relationship such as a marriage. He concludes with, "What makes matters even more challenging is the fact that we ask a great deal of marriage, of any serious intimate relationship. Perhaps the greatest demand we make is that it should combine passion and stability, romance and monogamy, transports of tenderness and excitement from the person who will also perform the many mundane tasks of daily living. In other words, meld everyday love with romantic/erotic love." He offers suggestions for discussion and guidelines for therapists.
Applying all of this in our work
As family psychiatrists, we can allow couples and families a therapeutic space to discuss the meaning and assumptions in their marriage. We can discuss the frame of the marriage: Is it sacred, secular, or postmodern? In this way, we can provide a context to the current struggles that couples and families might have.
To begin, we can ask about the past. We can say, "People get married for different reasons. What were your reasons? Do you consider your marriage to be a sacred or a secular? What does this mean to you?"
Delving deeper and focusing more on the present, "What is your current experience of your marriage? How do your expectations differ now than from your expectations in the past? What is the role of romance in your marriage?
What type of marriage did you want when you began this marriage? Is there romance in your marriage? What kind of marriage do you want now?
Focusing on going forward we can ask: "What works well in your marriage/family? What are your strengths? What needs to change in your marriage?"
In the late 1970s, postmodernism emerged in the world. Postmodernism stands in contrast to the "modern" or scientific view that touts a singularity of truth and a singular view of the world. Social construction is a type of postmodern theory that states that truth, reality, and knowledge are based in the social context of that particular person. Inevitably, postmodernism affects how we think about and conceptualize marriage. Postmodernism and marriage will be the subject of the next column.
I would like to thank Peter Chaloner, M.A., LL.B, B.A. (Honors), and Dip. Theo., for his comments and corrections.
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals" (New York: Routledge, 2013).
Throughout history, views of marriage have evolved as societies change. Since the 6th century, the Roman Catholic Church has played a prominent role in thinking and developing our ideas about marriage and family. In October, the church sent out a document that included a questionnaire to its bishops around the world to find out what Catholics think about the "modern family." The Vatican sent out the document in preparation for the Synod of Bishops on the Family, which is slated for October 2014. Before we get the results, let’s review how society has reflected on marriage and family.
Historically, marriages often were strategic alliances between families. It was common for marriage to be between first and second cousins in order to strengthen family ties. Polygamy has been common throughout history and continues in many communities to this day.
Monogamy is also found throughout history, but in 1215, the Catholic Church decreed that partners had to publicly post notices of an impending marriage in a local parish to cut down on the number of invalid marriages. Until the 1500s, the Catholic Church accepted a couple’s word that they had exchanged marriage vows, with no witnesses or corroborating evidence needed. In the 1500s, with the rise in Protestantism, marriage became a civil matter rather than a sacrament. By 1639, states such as Massachusetts began requiring marriage licenses, and by the 19th century, marriage licenses were common in the United States.
Marriage through the ages
Here is a listing of the way in which marriage has been conceptualized over the years:
Arranged alliances: A strategic alliance between families.
Family ties: Keeping alliances within the family; the majority of all marriages throughout history were between first and second cousins.
Polygamy: A phenomenon that has been common throughout history.
Babies optional: In many early cultures, men could dissolve a marriage or take another wife if a woman was infertile. However, the early Christian church was a trailblazer in arguing that marriage was not contingent upon producing offspring.
Monogamy: This practice became the guiding principle for Western marriages between the 6th and 9th centuries because of the church.
Sacred vs. secular: In 1215, the Roman Catholic Church decreed that partners had to publicly post notices, or banns, of an impending marriage in a local parish in order to cut down on the number of invalid marriages. Until the 1500s, the church accepted a couple’s word that they had exchanged marriage vows, with no witnesses or corroborating evidence needed.
Civil marriage: By 1639, states such as Massachusetts began requiring marriage licenses and, by the 19th century, marriage licenses were common in the United States.
Romance: By the 1900s, mutual attraction became important.
Market economics: Families historically controlled access to inheritance of agricultural land, but with the spread of a market economy, it becomes possible for people to marry outside of this inheritance.
Women’s equality: About 50 years ago, in Western countries, women and men began to have equal rights and responsibilities. Instead of being about unique, gender-based roles, most partners conceived of their unions in terms of flexible divisions of labor, companionship, and mutual sexual attraction.
Same-sex marriages: One of the reasons for the stunningly rapid increase in acceptance of same-sex marriage is because heterosexuals have completely changed their notion that all marriages are between a man and a woman, notes Stephanie Coontz, Ph.D. "We now believe marriage is based on love, mutual sexual attraction, equality, and a flexible division of labor."
Source: Adapted from "Marriage, a History: From Obedience to Intimacy, or How Love Conquered Marriage," (New York: Viking, 2005), by Dr. Coontz.
A sacred view of marriage
The Catholic position throughout history has been that marriage is one of the seven sacraments bestowed by Christ. This questionnaire is an attempt by the Vatican to understand more about "mixed or interreligious marriages; the single-parent family; polygamy; marriages with the consequent problem of a dowry, sometimes understood as the purchase price of the woman; the caste system; a culture of noncommitment and a presumption that the marriage bond can be temporary; forms of feminism hostile to the Church; migration and the reformulation of the very concept of the family; relativist pluralism in the conception of marriage; the influence of the media on popular culture in its understanding of marriage and family life; underlying trends of thought in legislative proposals which devalue the idea of permanence and faithfulness in the marriage covenant; an increase in the practice of surrogate motherhood (wombs for hire); and new interpretations of what is considered a human right."
Thirty-nine questions are on the questionnaire. Questions 4, 5, and 6 are of most interest to family psychiatrists. Deserving of admiration is its concern for families in migration and for the mistreatment of women.
The terms "regular" and "irregular," used in the questionnaire, are canonical terms unrelated to what actually happens in any given society. It should also be explained that Catholics who married always had to declare that they would welcome such children as God happened to send along, recognizing that he might choose not to send any. A decision to refuse to accept the possibility of children invalidated the marriage vows and constitutes grounds for annulment.
Excerpts from the Vatican document
Questions 4, 5, and 6 of the Vatican’s questionnaire seem aimed at gathering data on different kinds of families. Here are those three questions:
Pastoral Care in Certain Difficult Marital Situations
a) Is cohabitation ad experimentum a pastoral reality in your particular Church? Can you approximate a percentage?
b) Do unions which are not recognized either religiously or civilly exist? Are reliable statistics available?
c) Are separated couples and those divorced and remarried a pastoral reality in your particular Church? Can you approximate a percentage? How do you deal with this situation in appropriate pastoral programmes? (sic)
d) In all the above cases, how do the baptized live in this irregular situation? Are they aware of it? Are they simply indifferent? Do they feel marginalized or suffer from the impossibility of receiving the sacraments?
f) Could a simplification of canonical practice in recognizing a declaration of nullity of the marriage bond provide a positive contribution to solving the problems of the persons involved? If yes, what form would it take?
Does a ministry exist to attend to these cases? Describe this pastoral ministry? Do such programmes exist on the national and diocesan levels? How is God’s mercy proclaimed to separated couples and those divorced and remarried, and how does the Church put into practice her support for them in their journey of faith?
On Unions of Persons of the Same Sex
a) Is there a law in your country recognizing civil unions for people of the same-sex and equating it in some way to marriage?
b) What is the attitude of the local and particular Churches towards both the State as the promoter of civil unions between persons of the same sex and the people involved in this type of union?
c) What pastoral attention can be given to people who have chosen to live in these types of union?
In the case of unions of persons of the same sex who have adopted children, what can be done pastorally in light of transmitting the faith?
The Education of Children in Irregular Marriages
a) What is the estimated proportion of children and adolescents in these cases, as regards children who are born and raised in regularly constituted families?
b) How do parents in these situations approach the Church? What do they ask? Do they request the sacraments only or do they also want catechesis and the general teaching of religion?
c) How do the particular Churches attempt to meet the needs of the parents of these children to provide them with a Christian education?
Source: Pastoral Challenges to the Family in the Context of Evangelization
A secular view of marriage
A secular view of marriage has been advanced by economists Betsey Stevenson, Ph.D., and Justin Wolfers, Ph.D., who describe the extent to which marriage is shaped by economic forces. "Productive marriage" is based on a division of labor. In the earlier part of the 20th century in Western countries, school, education, and the emerging TV and magazine markets illustrated how women could be good homemakers and men could be good providers. The liberation of women through education and access to birth control changed the playing field. Prior to this, college-educated women were the least likely to marry. Since the 1960s and 1970s, educated women could prevent pregnancy and support themselves, and found little use for the previous productive model of marriage.
Men, also, did not see educated, financially independent women as suitable marriage partners. The high divorce rate among those who married in the1970s reflected discontent with this model of the productive marriage.
In contrast, Dr. Stevenson and Dr. Wolfers write, "hedonic marriage" occurs when people who marry are of similar age, educational background, and perhaps occupation. The hedonic marriage better suits educated women who seek a companion, and it thrives when time and resources are available to enjoy companionable life. Same-sex marriages make sense when considered in this broad frame. Supporting this concept is the fact that couples who have married in recent years are more likely to stay together than were their parents’ generation. Of course, this discourse is only relevant in parts of the world in which women have access to birth control and opportunities for education, work, and social standing.
Romance and marriage
The question of romance in marriage is the hardest for psychiatrists, as scientists, to address. Romance has always been around, sometimes present in marriages and sometimes not. Romance is thought to be both essential and nonessential to marriage, depending on the purpose of the marriage. A good discussion by Dr. Henry Grunebaum can be found an article titled "Thinking about romantic/erotic love" in the Journal of Marital and Family Therapy(1997;23:295-307). His main points are that we do not have control over our feelings of romantic/erotic love, that these feelings occur relatively infrequently during most people’s lives, that being with a partner whom one loves, is valued and regarded as a good, that it sometimes conflicts with other values and goods, and lastly that although love is regarded as one essential basis for marriage, other qualities and capacities are important in sustaining a long-term relationship such as a marriage. He concludes with, "What makes matters even more challenging is the fact that we ask a great deal of marriage, of any serious intimate relationship. Perhaps the greatest demand we make is that it should combine passion and stability, romance and monogamy, transports of tenderness and excitement from the person who will also perform the many mundane tasks of daily living. In other words, meld everyday love with romantic/erotic love." He offers suggestions for discussion and guidelines for therapists.
Applying all of this in our work
As family psychiatrists, we can allow couples and families a therapeutic space to discuss the meaning and assumptions in their marriage. We can discuss the frame of the marriage: Is it sacred, secular, or postmodern? In this way, we can provide a context to the current struggles that couples and families might have.
To begin, we can ask about the past. We can say, "People get married for different reasons. What were your reasons? Do you consider your marriage to be a sacred or a secular? What does this mean to you?"
Delving deeper and focusing more on the present, "What is your current experience of your marriage? How do your expectations differ now than from your expectations in the past? What is the role of romance in your marriage?
What type of marriage did you want when you began this marriage? Is there romance in your marriage? What kind of marriage do you want now?
Focusing on going forward we can ask: "What works well in your marriage/family? What are your strengths? What needs to change in your marriage?"
In the late 1970s, postmodernism emerged in the world. Postmodernism stands in contrast to the "modern" or scientific view that touts a singularity of truth and a singular view of the world. Social construction is a type of postmodern theory that states that truth, reality, and knowledge are based in the social context of that particular person. Inevitably, postmodernism affects how we think about and conceptualize marriage. Postmodernism and marriage will be the subject of the next column.
I would like to thank Peter Chaloner, M.A., LL.B, B.A. (Honors), and Dip. Theo., for his comments and corrections.
Dr. Heru is with the department of psychiatry at the University of Colorado at Denver, Aurora. She is editor of the recently published book, "Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals" (New York: Routledge, 2013).

Creams and patches can replace narcotics for skin pain
LAS VEGAS – A topical mixture of amitriptyline and ketamine controls pain in a variety of skin conditions, even when more traditional options fail, according to Dr. Mark Davis, chair of the division of clinical dermatology at the Mayo Clinic in Rochester, Minn.
"We are getting patients off systemic narcotics with these mixtures," he said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Lidocaine patches are allowing leg ulcer patients to drop narcotics, too, and are greatly helping those with erythromelalgia, an often-misdiagnosed condition involving intermittent and excruciating, burning pain in the feet, hands, and sometimes ears. "To have something topical [for such pain] is terrific," Dr. Davis said.

The Mayo Clinic uses topical amitriptyline and ketamine for brachioradial pruritus, erythromelalgia, rectogenital and perineal pain, and other localized skin pain recalcitrant to oral medications and other standard approaches. Dr. Davis and his colleagues recently published several reviews and retrospective studies on the use of topical pain relievers, including a recent article showing that more than half the patients who used topical amitriptyline-ketamine for pain reported substantial or complete relief (Pain Physician 2012;15:485-8).
Pharmaceutical companies are working to bring the combination to market, but it’s not yet available commercially, so Mayo Clinic dermatologists have their pharmacists compound it in two strengths – 2% amitriptyline and either 0.5% or 5% ketamine – using Lipoderm cream as the base, according to Dr. Davis. Patients apply the mixture three times daily. Why it works isn’t clear; the drugs have different and perhaps synergistic effects on skin pain.
"I try to get people to use it [the product] on small parts of the body, such as the hands and feet, and, in patients with brachioradial pruritus, both arms," said Dr. Davis. "I’ve never used it any more extensively than that; I am afraid patients would absorb too much ketamine," he said.
Of more than 1,000 Mayo Clinic patients who have tried the combination, "I’d say less than 1% has told me that they’ve ever had a side effect," he said. "I’ve had just two or three patients tell me they’ve gotten nightmares," a known effect of ketamine. "This is a product that has great promise," he noted.
Meanwhile, some erythromelalgia patients at the Mayo Clinic have been able to walk again after applying lidocaine patches to their feet, and the clinicians there consider the patches first-line treatment for the condition. "Many patients are well controlled just by using [the patches], and I don’t think I’ve come across any side effects in the hundreds of patients I’ve treated," Dr. Davis said. In the inherited form of the disease, which accounts for perhaps 5% of cases, erythromelalgia is caused by a genetic sodium channel glitch that keeps nerves in the skin firing once they are stimulated.
Lidocaine patches also are "really useful for patients with bad, painful ulcers; I use [them] over whatever wound care I am using," Dr. Davis noted. Sometimes these patients can discontinue, or at least reduce, their use of narcotics, he said.
Lidocaine helps with debridement, too. "For leg ulcers, our nurses take 4 x 4-inch gauze and soak it in lidocaine 4% solution, and leave it on the ulcer for about 20 minutes. We are usually able to debride those ulcers [after that] even if they were very painful to start," he said.
Dr. Davis has no relevant disclosures. SDEF and this news organization are owned by Frontline Medical Communications.
LAS VEGAS – A topical mixture of amitriptyline and ketamine controls pain in a variety of skin conditions, even when more traditional options fail, according to Dr. Mark Davis, chair of the division of clinical dermatology at the Mayo Clinic in Rochester, Minn.
"We are getting patients off systemic narcotics with these mixtures," he said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Lidocaine patches are allowing leg ulcer patients to drop narcotics, too, and are greatly helping those with erythromelalgia, an often-misdiagnosed condition involving intermittent and excruciating, burning pain in the feet, hands, and sometimes ears. "To have something topical [for such pain] is terrific," Dr. Davis said.
The Mayo Clinic uses topical amitriptyline and ketamine for brachioradial pruritus, erythromelalgia, rectogenital and perineal pain, and other localized skin pain recalcitrant to oral medications and other standard approaches. Dr. Davis and his colleagues recently published several reviews and retrospective studies on the use of topical pain relievers, including a recent article showing that more than half the patients who used topical amitriptyline-ketamine for pain reported substantial or complete relief (Pain Physician 2012;15:485-8).
Pharmaceutical companies are working to bring the combination to market, but it’s not yet available commercially, so Mayo Clinic dermatologists have their pharmacists compound it in two strengths – 2% amitriptyline and either 0.5% or 5% ketamine – using Lipoderm cream as the base, according to Dr. Davis. Patients apply the mixture three times daily. Why it works isn’t clear; the drugs have different and perhaps synergistic effects on skin pain.
"I try to get people to use it [the product] on small parts of the body, such as the hands and feet, and, in patients with brachioradial pruritus, both arms," said Dr. Davis. "I’ve never used it any more extensively than that; I am afraid patients would absorb too much ketamine," he said.
Of more than 1,000 Mayo Clinic patients who have tried the combination, "I’d say less than 1% has told me that they’ve ever had a side effect," he said. "I’ve had just two or three patients tell me they’ve gotten nightmares," a known effect of ketamine. "This is a product that has great promise," he noted.
Meanwhile, some erythromelalgia patients at the Mayo Clinic have been able to walk again after applying lidocaine patches to their feet, and the clinicians there consider the patches first-line treatment for the condition. "Many patients are well controlled just by using [the patches], and I don’t think I’ve come across any side effects in the hundreds of patients I’ve treated," Dr. Davis said. In the inherited form of the disease, which accounts for perhaps 5% of cases, erythromelalgia is caused by a genetic sodium channel glitch that keeps nerves in the skin firing once they are stimulated.
Lidocaine patches also are "really useful for patients with bad, painful ulcers; I use [them] over whatever wound care I am using," Dr. Davis noted. Sometimes these patients can discontinue, or at least reduce, their use of narcotics, he said.
Lidocaine helps with debridement, too. "For leg ulcers, our nurses take 4 x 4-inch gauze and soak it in lidocaine 4% solution, and leave it on the ulcer for about 20 minutes. We are usually able to debride those ulcers [after that] even if they were very painful to start," he said.
Dr. Davis has no relevant disclosures. SDEF and this news organization are owned by Frontline Medical Communications.
LAS VEGAS – A topical mixture of amitriptyline and ketamine controls pain in a variety of skin conditions, even when more traditional options fail, according to Dr. Mark Davis, chair of the division of clinical dermatology at the Mayo Clinic in Rochester, Minn.
"We are getting patients off systemic narcotics with these mixtures," he said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
Lidocaine patches are allowing leg ulcer patients to drop narcotics, too, and are greatly helping those with erythromelalgia, an often-misdiagnosed condition involving intermittent and excruciating, burning pain in the feet, hands, and sometimes ears. "To have something topical [for such pain] is terrific," Dr. Davis said.
The Mayo Clinic uses topical amitriptyline and ketamine for brachioradial pruritus, erythromelalgia, rectogenital and perineal pain, and other localized skin pain recalcitrant to oral medications and other standard approaches. Dr. Davis and his colleagues recently published several reviews and retrospective studies on the use of topical pain relievers, including a recent article showing that more than half the patients who used topical amitriptyline-ketamine for pain reported substantial or complete relief (Pain Physician 2012;15:485-8).
Pharmaceutical companies are working to bring the combination to market, but it’s not yet available commercially, so Mayo Clinic dermatologists have their pharmacists compound it in two strengths – 2% amitriptyline and either 0.5% or 5% ketamine – using Lipoderm cream as the base, according to Dr. Davis. Patients apply the mixture three times daily. Why it works isn’t clear; the drugs have different and perhaps synergistic effects on skin pain.
"I try to get people to use it [the product] on small parts of the body, such as the hands and feet, and, in patients with brachioradial pruritus, both arms," said Dr. Davis. "I’ve never used it any more extensively than that; I am afraid patients would absorb too much ketamine," he said.
Of more than 1,000 Mayo Clinic patients who have tried the combination, "I’d say less than 1% has told me that they’ve ever had a side effect," he said. "I’ve had just two or three patients tell me they’ve gotten nightmares," a known effect of ketamine. "This is a product that has great promise," he noted.
Meanwhile, some erythromelalgia patients at the Mayo Clinic have been able to walk again after applying lidocaine patches to their feet, and the clinicians there consider the patches first-line treatment for the condition. "Many patients are well controlled just by using [the patches], and I don’t think I’ve come across any side effects in the hundreds of patients I’ve treated," Dr. Davis said. In the inherited form of the disease, which accounts for perhaps 5% of cases, erythromelalgia is caused by a genetic sodium channel glitch that keeps nerves in the skin firing once they are stimulated.
Lidocaine patches also are "really useful for patients with bad, painful ulcers; I use [them] over whatever wound care I am using," Dr. Davis noted. Sometimes these patients can discontinue, or at least reduce, their use of narcotics, he said.
Lidocaine helps with debridement, too. "For leg ulcers, our nurses take 4 x 4-inch gauze and soak it in lidocaine 4% solution, and leave it on the ulcer for about 20 minutes. We are usually able to debride those ulcers [after that] even if they were very painful to start," he said.
Dr. Davis has no relevant disclosures. SDEF and this news organization are owned by Frontline Medical Communications.
EXPERT ANALYSIS FROM THE SDEF LAS VEGAS DERMATOLOGY SEMINAR

Zinc oxide
Zinc is a trace element, and it is not synthesized by the human body. The element was identified in the 1960s as being essential for human health and development. Zinc is a cofactor in more than 300 enzymes necessary for cell function. In the dermatologic realm, zinc deficiency has been associated with skin alterations, delayed wound healing, and hair loss.
Zinc oxide (ZnO) is a metal oxide that also has a broad profile in dermatology. It is perhaps best known as a physical sunscreen ingredient. ZnO and titanium dioxide (TiO2) have long been used in this manner. Both ZnO and TiO2 also have been increasingly used to replace large-particle compounds in numerous cosmetics and sunscreens. These two compounds have demonstrated effective protection against UV-induced damage, providing stronger protection against UV radiation while leaving less white residue than previous generations of physical sunscreens.
Particles of ZnO in earlier sunscreens were found to be too large to penetrate the stratum corneum and, thus, were deemed biologically inactive (J. Am. Acad. Dermatol. 1999;40:85-90). However, in novel nanoparticle form, such metal oxides absorb UV radiation, leading to photocatalysis and the release of reactive oxygen species (Australas. J. Dermatol. 2011;52:1-6). Indeed, nanoparticles exhibit new physiochemical properties as a result of increased surface area as compared to large-form products, and the potential adverse effects of the novel nanoparticle formulations in sunscreens cannot be adequately extrapolated from the effects of older-generation larger-particle skin care products (J. Drugs Dermatol. 2010;9:475-81; Int. J. Dermatol. 2011;50:247-54. The relative safety of ZnO nanoparticles will be discussed in a future column. The focus in this column will be a brief comparison with TiO2 and other indications for ZnO.
ZnO and TiO2
While numerous studies explore both TiO2 and ZnO, the latter is noted for greater versatility within the dermatologic armamentarium. In addition, ZnO is less photoactive and is associated with a lower refractive index in visible light than TiO2 (1.9 vs. 2.6, respectively) (J. Am. Acad. Dermatol. 1999;40:85-90); therefore, TiO2 appears whiter and is more difficult to incorporate into transparent products.
Another important difference is the spectrum of action. That is, only avobenzone (butyl methoxydibenzoylmethane) and ZnO are approved in the United States for broad-spectrum protection against UVA wavelengths greater than 360 nm, because TiO2 has been shown to be effective only against UV wavelengths less than 360 nm (UVA is 320-400 nm). In a study by Beasley and Meyer, TiO2 delivered neither the same level of UVA attenuation nor protection from UVA to human skin as did photostabilized formulations of avobenzone or ZnO. Therefore, TiO2 is not a suitable substitute for avobenzone and ZnO for strong UVA protection (Am. J. Clin. Dermatol. 2010;11:413-21).
Indications beyond photoprotection
More than 20 years ago, Hughes and McLean showed that a ZnO tape was effective in dressing fingertip and soft tissue injuries that were resistant to healing (Arch. Emerg. Med. 1988;5:223-7). More recently, Parboteeah and Brown demonstrated the efficacy of treating recalcitrant venous leg ulcers with ZnO paste bandages (Br. J. Nurs. 2008;17:S30, S32, S34-6). In addition, Treadwell has shown that the weekly application of ZnO compression dressings to surgical wounds of the lower leg promotes healing (Dermatol. Surg. 2011;37:166-7).
Micronized zinc oxide is included in a 4% hydroquinone/10% L-ascorbic acid treatment system recently found (in a small study of 34 females) to be effective in alleviating early signs of photodamage in normal to oily skin. Thirty patients, with minimal or mild facial photodamage and hyperpigmentation, completed the 12-week treatment regimen. All the participants were satisfied with the appearance of their skin after the study, with median scores for all assessment parameters significantly improved compared with baseline (J. Drugs Dermatol. 2011;10:1455-61). ZnO also is an active ingredient in formulations intended to support the healing of perianal eczema (Hautarzt. 2010;61:33-8).
A 2001 report on a series of blinded, randomized clinical trials conducted by Baldwin et al. showed that clinical benefits were derived from the continuous topical administration of a ZnO/petrolatum formulation in a diaper introduced at that time. The first study was undertaken to verify that the ZnO/petrolatum formulation was indeed transferred from the diaper to the child’s skin. Stratum corneum (SC) samples were analyzed from each child after the wearing of a single diaper for 3 hours or multiple diapers for 24 hours. The results indicated effective transfer, with ZnO increasing in the SC from 4.2 mcg/cm2 at 3 hours to more than 8 mcg/cm2 at 24 hours.
The second study of the formulation, in an adult arm model, assessed the prevention of irritation and SC damage induced by sodium laureth sulfate. The investigators found that the ZnO/petrolatum combination yielded significant reductions in SC damage and erythema. The third study, a 4-week trial in which 268 infants were assessed, considered the effects of the formulation on erythema and diaper rash. Half of the infants wore the test diaper and half used a control diaper lacking the ZnO/petrolatum product. Significant reductions in erythema and diaper rash were indeed observed in the test group (J. Eur. Acad. Dermatol. Venereol. 2001;15 Suppl 1:5-11).
A 2009 study showed that an unmedicated ZnO/petrolatum paste was effective in restoring the properties of the skin, allowing for balanced transepidermal water loss and water retention by SC previously compromised by diaper dermatitis. This skin condition affects approximately 50% of infants and a small percentage of the bedridden elderly (Int. J. Cosmet. Sci. 2009;31:369-74).
In 2010, a study that assessed the effectiveness of topical ZnO ointment using the rabbit ear hypertrophic scar model showed that the application of 40% ZnO significantly reduced clinical scar hypertrophy scores at 6 weeks compared with placebo. The researchers concluded that these results may suggest clinical applications for ZnO in the treatment of hypertrophic scars in humans (Burns 2010;36:1027-35). In addition, ZnO has demonstrated antibacterial properties, with nanoparticles exhibiting more potent antibacterial activity than bulk ZnO (Sci. Technol. Adv. Mater. 2008;9:1-7).
Products
ZnO is a key ingredient in calamine lotion, an antipruritic compound used to treat various mild conditions such as bites and stings from insects, eczema, poison ivy, rashes, and sunburn. It is also available over the counter in ointment or suppository form for healing hemorrhoids and fissures. In addition, ZnO is used widely in baby powders, barrier creams, moisturizers, antiseptic ointments, antidandruff shampoos, athletic bandage tape, and, of course, sunscreens.
Conclusion
ZnO is a versatile inorganic metal oxide with multiple indications in dermatology. Consequently, it is included in a wide array of skin care products, including shampoos, moisturizers, and sunscreens. Its use in nanoparticle form, along with the similar use of its physical sunscreen counterpart TiO2, represents one of the many subjects debated within the larger context of sunscreen use. The next edition of this column will focus on the relative safety of zinc oxide nanoparticles.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook "Cosmetic Dermatology: Principles and Practice" (McGraw-Hill, April 2002), and a book for consumers, "The Skin Type Solution" (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001 and joined the editorial advisory board in 2004. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.
This column, "Cosmeceutical Critique," appears regularly in Skin & Allergy News, a publication of Frontline Medical News.
Zinc is a trace element, and it is not synthesized by the human body. The element was identified in the 1960s as being essential for human health and development. Zinc is a cofactor in more than 300 enzymes necessary for cell function. In the dermatologic realm, zinc deficiency has been associated with skin alterations, delayed wound healing, and hair loss.
Zinc oxide (ZnO) is a metal oxide that also has a broad profile in dermatology. It is perhaps best known as a physical sunscreen ingredient. ZnO and titanium dioxide (TiO2) have long been used in this manner. Both ZnO and TiO2 also have been increasingly used to replace large-particle compounds in numerous cosmetics and sunscreens. These two compounds have demonstrated effective protection against UV-induced damage, providing stronger protection against UV radiation while leaving less white residue than previous generations of physical sunscreens.
Particles of ZnO in earlier sunscreens were found to be too large to penetrate the stratum corneum and, thus, were deemed biologically inactive (J. Am. Acad. Dermatol. 1999;40:85-90). However, in novel nanoparticle form, such metal oxides absorb UV radiation, leading to photocatalysis and the release of reactive oxygen species (Australas. J. Dermatol. 2011;52:1-6). Indeed, nanoparticles exhibit new physiochemical properties as a result of increased surface area as compared to large-form products, and the potential adverse effects of the novel nanoparticle formulations in sunscreens cannot be adequately extrapolated from the effects of older-generation larger-particle skin care products (J. Drugs Dermatol. 2010;9:475-81; Int. J. Dermatol. 2011;50:247-54. The relative safety of ZnO nanoparticles will be discussed in a future column. The focus in this column will be a brief comparison with TiO2 and other indications for ZnO.
ZnO and TiO2
While numerous studies explore both TiO2 and ZnO, the latter is noted for greater versatility within the dermatologic armamentarium. In addition, ZnO is less photoactive and is associated with a lower refractive index in visible light than TiO2 (1.9 vs. 2.6, respectively) (J. Am. Acad. Dermatol. 1999;40:85-90); therefore, TiO2 appears whiter and is more difficult to incorporate into transparent products.
Another important difference is the spectrum of action. That is, only avobenzone (butyl methoxydibenzoylmethane) and ZnO are approved in the United States for broad-spectrum protection against UVA wavelengths greater than 360 nm, because TiO2 has been shown to be effective only against UV wavelengths less than 360 nm (UVA is 320-400 nm). In a study by Beasley and Meyer, TiO2 delivered neither the same level of UVA attenuation nor protection from UVA to human skin as did photostabilized formulations of avobenzone or ZnO. Therefore, TiO2 is not a suitable substitute for avobenzone and ZnO for strong UVA protection (Am. J. Clin. Dermatol. 2010;11:413-21).
Indications beyond photoprotection
More than 20 years ago, Hughes and McLean showed that a ZnO tape was effective in dressing fingertip and soft tissue injuries that were resistant to healing (Arch. Emerg. Med. 1988;5:223-7). More recently, Parboteeah and Brown demonstrated the efficacy of treating recalcitrant venous leg ulcers with ZnO paste bandages (Br. J. Nurs. 2008;17:S30, S32, S34-6). In addition, Treadwell has shown that the weekly application of ZnO compression dressings to surgical wounds of the lower leg promotes healing (Dermatol. Surg. 2011;37:166-7).
Micronized zinc oxide is included in a 4% hydroquinone/10% L-ascorbic acid treatment system recently found (in a small study of 34 females) to be effective in alleviating early signs of photodamage in normal to oily skin. Thirty patients, with minimal or mild facial photodamage and hyperpigmentation, completed the 12-week treatment regimen. All the participants were satisfied with the appearance of their skin after the study, with median scores for all assessment parameters significantly improved compared with baseline (J. Drugs Dermatol. 2011;10:1455-61). ZnO also is an active ingredient in formulations intended to support the healing of perianal eczema (Hautarzt. 2010;61:33-8).
A 2001 report on a series of blinded, randomized clinical trials conducted by Baldwin et al. showed that clinical benefits were derived from the continuous topical administration of a ZnO/petrolatum formulation in a diaper introduced at that time. The first study was undertaken to verify that the ZnO/petrolatum formulation was indeed transferred from the diaper to the child’s skin. Stratum corneum (SC) samples were analyzed from each child after the wearing of a single diaper for 3 hours or multiple diapers for 24 hours. The results indicated effective transfer, with ZnO increasing in the SC from 4.2 mcg/cm2 at 3 hours to more than 8 mcg/cm2 at 24 hours.
The second study of the formulation, in an adult arm model, assessed the prevention of irritation and SC damage induced by sodium laureth sulfate. The investigators found that the ZnO/petrolatum combination yielded significant reductions in SC damage and erythema. The third study, a 4-week trial in which 268 infants were assessed, considered the effects of the formulation on erythema and diaper rash. Half of the infants wore the test diaper and half used a control diaper lacking the ZnO/petrolatum product. Significant reductions in erythema and diaper rash were indeed observed in the test group (J. Eur. Acad. Dermatol. Venereol. 2001;15 Suppl 1:5-11).
A 2009 study showed that an unmedicated ZnO/petrolatum paste was effective in restoring the properties of the skin, allowing for balanced transepidermal water loss and water retention by SC previously compromised by diaper dermatitis. This skin condition affects approximately 50% of infants and a small percentage of the bedridden elderly (Int. J. Cosmet. Sci. 2009;31:369-74).
In 2010, a study that assessed the effectiveness of topical ZnO ointment using the rabbit ear hypertrophic scar model showed that the application of 40% ZnO significantly reduced clinical scar hypertrophy scores at 6 weeks compared with placebo. The researchers concluded that these results may suggest clinical applications for ZnO in the treatment of hypertrophic scars in humans (Burns 2010;36:1027-35). In addition, ZnO has demonstrated antibacterial properties, with nanoparticles exhibiting more potent antibacterial activity than bulk ZnO (Sci. Technol. Adv. Mater. 2008;9:1-7).
Products
ZnO is a key ingredient in calamine lotion, an antipruritic compound used to treat various mild conditions such as bites and stings from insects, eczema, poison ivy, rashes, and sunburn. It is also available over the counter in ointment or suppository form for healing hemorrhoids and fissures. In addition, ZnO is used widely in baby powders, barrier creams, moisturizers, antiseptic ointments, antidandruff shampoos, athletic bandage tape, and, of course, sunscreens.
Conclusion
ZnO is a versatile inorganic metal oxide with multiple indications in dermatology. Consequently, it is included in a wide array of skin care products, including shampoos, moisturizers, and sunscreens. Its use in nanoparticle form, along with the similar use of its physical sunscreen counterpart TiO2, represents one of the many subjects debated within the larger context of sunscreen use. The next edition of this column will focus on the relative safety of zinc oxide nanoparticles.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook "Cosmetic Dermatology: Principles and Practice" (McGraw-Hill, April 2002), and a book for consumers, "The Skin Type Solution" (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001 and joined the editorial advisory board in 2004. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.
This column, "Cosmeceutical Critique," appears regularly in Skin & Allergy News, a publication of Frontline Medical News.
Zinc is a trace element, and it is not synthesized by the human body. The element was identified in the 1960s as being essential for human health and development. Zinc is a cofactor in more than 300 enzymes necessary for cell function. In the dermatologic realm, zinc deficiency has been associated with skin alterations, delayed wound healing, and hair loss.
Zinc oxide (ZnO) is a metal oxide that also has a broad profile in dermatology. It is perhaps best known as a physical sunscreen ingredient. ZnO and titanium dioxide (TiO2) have long been used in this manner. Both ZnO and TiO2 also have been increasingly used to replace large-particle compounds in numerous cosmetics and sunscreens. These two compounds have demonstrated effective protection against UV-induced damage, providing stronger protection against UV radiation while leaving less white residue than previous generations of physical sunscreens.
Particles of ZnO in earlier sunscreens were found to be too large to penetrate the stratum corneum and, thus, were deemed biologically inactive (J. Am. Acad. Dermatol. 1999;40:85-90). However, in novel nanoparticle form, such metal oxides absorb UV radiation, leading to photocatalysis and the release of reactive oxygen species (Australas. J. Dermatol. 2011;52:1-6). Indeed, nanoparticles exhibit new physiochemical properties as a result of increased surface area as compared to large-form products, and the potential adverse effects of the novel nanoparticle formulations in sunscreens cannot be adequately extrapolated from the effects of older-generation larger-particle skin care products (J. Drugs Dermatol. 2010;9:475-81; Int. J. Dermatol. 2011;50:247-54. The relative safety of ZnO nanoparticles will be discussed in a future column. The focus in this column will be a brief comparison with TiO2 and other indications for ZnO.
ZnO and TiO2
While numerous studies explore both TiO2 and ZnO, the latter is noted for greater versatility within the dermatologic armamentarium. In addition, ZnO is less photoactive and is associated with a lower refractive index in visible light than TiO2 (1.9 vs. 2.6, respectively) (J. Am. Acad. Dermatol. 1999;40:85-90); therefore, TiO2 appears whiter and is more difficult to incorporate into transparent products.
Another important difference is the spectrum of action. That is, only avobenzone (butyl methoxydibenzoylmethane) and ZnO are approved in the United States for broad-spectrum protection against UVA wavelengths greater than 360 nm, because TiO2 has been shown to be effective only against UV wavelengths less than 360 nm (UVA is 320-400 nm). In a study by Beasley and Meyer, TiO2 delivered neither the same level of UVA attenuation nor protection from UVA to human skin as did photostabilized formulations of avobenzone or ZnO. Therefore, TiO2 is not a suitable substitute for avobenzone and ZnO for strong UVA protection (Am. J. Clin. Dermatol. 2010;11:413-21).
Indications beyond photoprotection
More than 20 years ago, Hughes and McLean showed that a ZnO tape was effective in dressing fingertip and soft tissue injuries that were resistant to healing (Arch. Emerg. Med. 1988;5:223-7). More recently, Parboteeah and Brown demonstrated the efficacy of treating recalcitrant venous leg ulcers with ZnO paste bandages (Br. J. Nurs. 2008;17:S30, S32, S34-6). In addition, Treadwell has shown that the weekly application of ZnO compression dressings to surgical wounds of the lower leg promotes healing (Dermatol. Surg. 2011;37:166-7).
Micronized zinc oxide is included in a 4% hydroquinone/10% L-ascorbic acid treatment system recently found (in a small study of 34 females) to be effective in alleviating early signs of photodamage in normal to oily skin. Thirty patients, with minimal or mild facial photodamage and hyperpigmentation, completed the 12-week treatment regimen. All the participants were satisfied with the appearance of their skin after the study, with median scores for all assessment parameters significantly improved compared with baseline (J. Drugs Dermatol. 2011;10:1455-61). ZnO also is an active ingredient in formulations intended to support the healing of perianal eczema (Hautarzt. 2010;61:33-8).
A 2001 report on a series of blinded, randomized clinical trials conducted by Baldwin et al. showed that clinical benefits were derived from the continuous topical administration of a ZnO/petrolatum formulation in a diaper introduced at that time. The first study was undertaken to verify that the ZnO/petrolatum formulation was indeed transferred from the diaper to the child’s skin. Stratum corneum (SC) samples were analyzed from each child after the wearing of a single diaper for 3 hours or multiple diapers for 24 hours. The results indicated effective transfer, with ZnO increasing in the SC from 4.2 mcg/cm2 at 3 hours to more than 8 mcg/cm2 at 24 hours.
The second study of the formulation, in an adult arm model, assessed the prevention of irritation and SC damage induced by sodium laureth sulfate. The investigators found that the ZnO/petrolatum combination yielded significant reductions in SC damage and erythema. The third study, a 4-week trial in which 268 infants were assessed, considered the effects of the formulation on erythema and diaper rash. Half of the infants wore the test diaper and half used a control diaper lacking the ZnO/petrolatum product. Significant reductions in erythema and diaper rash were indeed observed in the test group (J. Eur. Acad. Dermatol. Venereol. 2001;15 Suppl 1:5-11).
A 2009 study showed that an unmedicated ZnO/petrolatum paste was effective in restoring the properties of the skin, allowing for balanced transepidermal water loss and water retention by SC previously compromised by diaper dermatitis. This skin condition affects approximately 50% of infants and a small percentage of the bedridden elderly (Int. J. Cosmet. Sci. 2009;31:369-74).
In 2010, a study that assessed the effectiveness of topical ZnO ointment using the rabbit ear hypertrophic scar model showed that the application of 40% ZnO significantly reduced clinical scar hypertrophy scores at 6 weeks compared with placebo. The researchers concluded that these results may suggest clinical applications for ZnO in the treatment of hypertrophic scars in humans (Burns 2010;36:1027-35). In addition, ZnO has demonstrated antibacterial properties, with nanoparticles exhibiting more potent antibacterial activity than bulk ZnO (Sci. Technol. Adv. Mater. 2008;9:1-7).
Products
ZnO is a key ingredient in calamine lotion, an antipruritic compound used to treat various mild conditions such as bites and stings from insects, eczema, poison ivy, rashes, and sunburn. It is also available over the counter in ointment or suppository form for healing hemorrhoids and fissures. In addition, ZnO is used widely in baby powders, barrier creams, moisturizers, antiseptic ointments, antidandruff shampoos, athletic bandage tape, and, of course, sunscreens.
Conclusion
ZnO is a versatile inorganic metal oxide with multiple indications in dermatology. Consequently, it is included in a wide array of skin care products, including shampoos, moisturizers, and sunscreens. Its use in nanoparticle form, along with the similar use of its physical sunscreen counterpart TiO2, represents one of the many subjects debated within the larger context of sunscreen use. The next edition of this column will focus on the relative safety of zinc oxide nanoparticles.
Dr. Baumann is chief executive officer of the Baumann Cosmetic & Research Institute in Miami Beach. She founded the cosmetic dermatology center at the University of Miami in 1997. Dr. Baumann wrote the textbook "Cosmetic Dermatology: Principles and Practice" (McGraw-Hill, April 2002), and a book for consumers, "The Skin Type Solution" (Bantam, 2006). She has contributed to the Cosmeceutical Critique column in Skin & Allergy News since January 2001 and joined the editorial advisory board in 2004. Dr. Baumann has received funding for clinical grants from Allergan, Aveeno, Avon Products, Galderma, Mary Kay, Medicis Pharmaceuticals, Neutrogena, Philosophy, Stiefel, Topix Pharmaceuticals, and Unilever.
This column, "Cosmeceutical Critique," appears regularly in Skin & Allergy News, a publication of Frontline Medical News.

The personal dimension of informed consent
Recently, a medical student assigned to my service spent a day in the outpatient office seeing patients with me. After seeing two consecutive patients who needed thyroidectomies, this student commented on the differences in how I obtained informed consent for thyroidectomy from the two patients. Why, she asked, had I spent relatively little time emphasizing the risks of the operation with one patient and so much more time discussing risks with the second patient?
In order to understand why there appeared to be such a dramatic difference between the discussions with the two patients, it is helpful to understand the different indications for surgery. The first patient had recently been diagnosed with a 2.3-cm papillary thyroid cancer. I had explained that the first step in the treatment was to remove the thyroid, and I detailed the risks to the recurrent laryngeal nerves and the parathyroid glands.
The second patient had been treated for Graves’ disease for the last 3 years. She had many cycles of hyper- and hypothyroidism and had now decided that she needed definitive treatment. Although she had discussed the option of radioactive iodine with her endocrinologist, she had a significant fear of radiation and also was hoping to become pregnant in the next several months. I had discussed the risks of thyroidectomy with this patient. However, even though the risk I quoted of having a complication from the thyroidectomy was just the same as in the first case, I deliberately spent more time discussing the ramifications of the complications and the alternatives with the second patient.
My student was initially perplexed by this description. As she correctly stated, if the risks are the same for the same operation between the two patients, why emphasize the risks so much more for the second patient, compared with the first?
To most surgeons, the reason for this difference is clear. The first patient needed to know the risks, but there were few options to total thyroidectomy as the initial step in the treatment. The second patient had the clear option of getting radioactive iodine instead of surgery. Although the risks of the surgical procedure are the same with the two operations, I felt that the second patient needed to clearly understand the alternative to surgery and to fully consider the implications of the potential complications should one occur in her case.
As I think back over this interchange with my student, it is clear that the informed consent discussion for any operation cannot be fully standardized for every patient. Even if the risks remain the same, the indications for surgery are different and, of course, the patients are different.
More than 30 years ago, Dr. C. Rollins Hanlon, then executive director of the American College of Surgeons wrote, "Both ethics and surgery are inexact disciplines, in definition, practice, and in relation to one another." The more years I have been in practice, the more I am convinced of the truth of these words. Although my two patients both needed the same operation, it was important for me to emphasize the choices that the second patient had. In so doing, I felt it was essential to ensure that in evaluating the choices, the patient fully understood the implications of the risks. Although the patient with thyroid cancer had the same risks of the procedure, she did not have a good alternative choice to surgery. The difference between these two patients, and in how I altered my discussions of the proposed thyroidectomy, reveal the personal dimension of informed consent that goes beyond a simple statement of risks.
In obtaining informed consent from my patients, I should be providing them with much more than "just the facts." Patients can (and often do) obtain the data about the risks of surgical procedures from the Internet prior to seeing me. I believe that I should be giving them something more than they could obtain from reading about the risks of a procedure. I should provide them with a context in which to consider the risks, relative to their particular condition. Even small risks may be very significant if there are alternatives that have no risks. In contrast, patients often quickly agree to high-risk operations when there is no good nonoperative alternative. As surgeons, we must be cognizant of the critical personal dimension of the informed consent process and thereby be sure to put the discussion of risks in the appropriate context to help our patients make good decisions.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Recently, a medical student assigned to my service spent a day in the outpatient office seeing patients with me. After seeing two consecutive patients who needed thyroidectomies, this student commented on the differences in how I obtained informed consent for thyroidectomy from the two patients. Why, she asked, had I spent relatively little time emphasizing the risks of the operation with one patient and so much more time discussing risks with the second patient?
In order to understand why there appeared to be such a dramatic difference between the discussions with the two patients, it is helpful to understand the different indications for surgery. The first patient had recently been diagnosed with a 2.3-cm papillary thyroid cancer. I had explained that the first step in the treatment was to remove the thyroid, and I detailed the risks to the recurrent laryngeal nerves and the parathyroid glands.
The second patient had been treated for Graves’ disease for the last 3 years. She had many cycles of hyper- and hypothyroidism and had now decided that she needed definitive treatment. Although she had discussed the option of radioactive iodine with her endocrinologist, she had a significant fear of radiation and also was hoping to become pregnant in the next several months. I had discussed the risks of thyroidectomy with this patient. However, even though the risk I quoted of having a complication from the thyroidectomy was just the same as in the first case, I deliberately spent more time discussing the ramifications of the complications and the alternatives with the second patient.
My student was initially perplexed by this description. As she correctly stated, if the risks are the same for the same operation between the two patients, why emphasize the risks so much more for the second patient, compared with the first?
To most surgeons, the reason for this difference is clear. The first patient needed to know the risks, but there were few options to total thyroidectomy as the initial step in the treatment. The second patient had the clear option of getting radioactive iodine instead of surgery. Although the risks of the surgical procedure are the same with the two operations, I felt that the second patient needed to clearly understand the alternative to surgery and to fully consider the implications of the potential complications should one occur in her case.
As I think back over this interchange with my student, it is clear that the informed consent discussion for any operation cannot be fully standardized for every patient. Even if the risks remain the same, the indications for surgery are different and, of course, the patients are different.
More than 30 years ago, Dr. C. Rollins Hanlon, then executive director of the American College of Surgeons wrote, "Both ethics and surgery are inexact disciplines, in definition, practice, and in relation to one another." The more years I have been in practice, the more I am convinced of the truth of these words. Although my two patients both needed the same operation, it was important for me to emphasize the choices that the second patient had. In so doing, I felt it was essential to ensure that in evaluating the choices, the patient fully understood the implications of the risks. Although the patient with thyroid cancer had the same risks of the procedure, she did not have a good alternative choice to surgery. The difference between these two patients, and in how I altered my discussions of the proposed thyroidectomy, reveal the personal dimension of informed consent that goes beyond a simple statement of risks.
In obtaining informed consent from my patients, I should be providing them with much more than "just the facts." Patients can (and often do) obtain the data about the risks of surgical procedures from the Internet prior to seeing me. I believe that I should be giving them something more than they could obtain from reading about the risks of a procedure. I should provide them with a context in which to consider the risks, relative to their particular condition. Even small risks may be very significant if there are alternatives that have no risks. In contrast, patients often quickly agree to high-risk operations when there is no good nonoperative alternative. As surgeons, we must be cognizant of the critical personal dimension of the informed consent process and thereby be sure to put the discussion of risks in the appropriate context to help our patients make good decisions.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Recently, a medical student assigned to my service spent a day in the outpatient office seeing patients with me. After seeing two consecutive patients who needed thyroidectomies, this student commented on the differences in how I obtained informed consent for thyroidectomy from the two patients. Why, she asked, had I spent relatively little time emphasizing the risks of the operation with one patient and so much more time discussing risks with the second patient?
In order to understand why there appeared to be such a dramatic difference between the discussions with the two patients, it is helpful to understand the different indications for surgery. The first patient had recently been diagnosed with a 2.3-cm papillary thyroid cancer. I had explained that the first step in the treatment was to remove the thyroid, and I detailed the risks to the recurrent laryngeal nerves and the parathyroid glands.
The second patient had been treated for Graves’ disease for the last 3 years. She had many cycles of hyper- and hypothyroidism and had now decided that she needed definitive treatment. Although she had discussed the option of radioactive iodine with her endocrinologist, she had a significant fear of radiation and also was hoping to become pregnant in the next several months. I had discussed the risks of thyroidectomy with this patient. However, even though the risk I quoted of having a complication from the thyroidectomy was just the same as in the first case, I deliberately spent more time discussing the ramifications of the complications and the alternatives with the second patient.
My student was initially perplexed by this description. As she correctly stated, if the risks are the same for the same operation between the two patients, why emphasize the risks so much more for the second patient, compared with the first?
To most surgeons, the reason for this difference is clear. The first patient needed to know the risks, but there were few options to total thyroidectomy as the initial step in the treatment. The second patient had the clear option of getting radioactive iodine instead of surgery. Although the risks of the surgical procedure are the same with the two operations, I felt that the second patient needed to clearly understand the alternative to surgery and to fully consider the implications of the potential complications should one occur in her case.
As I think back over this interchange with my student, it is clear that the informed consent discussion for any operation cannot be fully standardized for every patient. Even if the risks remain the same, the indications for surgery are different and, of course, the patients are different.
More than 30 years ago, Dr. C. Rollins Hanlon, then executive director of the American College of Surgeons wrote, "Both ethics and surgery are inexact disciplines, in definition, practice, and in relation to one another." The more years I have been in practice, the more I am convinced of the truth of these words. Although my two patients both needed the same operation, it was important for me to emphasize the choices that the second patient had. In so doing, I felt it was essential to ensure that in evaluating the choices, the patient fully understood the implications of the risks. Although the patient with thyroid cancer had the same risks of the procedure, she did not have a good alternative choice to surgery. The difference between these two patients, and in how I altered my discussions of the proposed thyroidectomy, reveal the personal dimension of informed consent that goes beyond a simple statement of risks.
In obtaining informed consent from my patients, I should be providing them with much more than "just the facts." Patients can (and often do) obtain the data about the risks of surgical procedures from the Internet prior to seeing me. I believe that I should be giving them something more than they could obtain from reading about the risks of a procedure. I should provide them with a context in which to consider the risks, relative to their particular condition. Even small risks may be very significant if there are alternatives that have no risks. In contrast, patients often quickly agree to high-risk operations when there is no good nonoperative alternative. As surgeons, we must be cognizant of the critical personal dimension of the informed consent process and thereby be sure to put the discussion of risks in the appropriate context to help our patients make good decisions.
Dr. Angelos is an ACS Fellow; the Linda Kohler Anderson Professor of Surgery and Surgical Ethics; chief, endocrine surgery; and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
The long view
If you can believe it, I once read a witty article about hair transplants. The authors suggested that the reporting of results should show follow-ups much longer than 6 or 12 months, since hair loss keeps on happening after transplants. What looks fine at 1 year may not look so good 10 years later.
They labeled one figure in their paper as follows: "True long-term follow-up." It was a photo of a tombstone.
Neither medical school nor residency training fosters the long view. You see a patient during a hospitalization for an acute illness. Case presentation focuses on diagnosis, pathogenesis, and treatment for the few days he or she is on the ward. You may follow the patient for at most a few months, or a year after discharge. Those discussing the case might note a prognosis in passing, but don’t give much sense of what is likely to happen to the patient over the course of years, let alone decades.
What actually happens, long after the patient goes home or the residency ends, varies much more than may seem plausible based on the snapshot you get during an acute episode.
Medical practice in the community, by contrast, is a long-haul affair. What you see when you follow patients for years can be quite unexpected.
I think of John, for instance. As a teenager, he had many bouts of widespread and debilitating atopic dermatitis. Topical therapy often failed to make a dent, leading to courses of prednisone that were followed at once by severe recurrences. Had someone asked me at the time, I would have predicted for John a life of miserable itch, and morbidity from systemic treatment.
We lost touch when John went off to college. He returned 15 years later, now all grown up, with a wife and family. He wanted to show me a mole.
"How’s your eczema been?" I asked.
"It’s hardly bothered me much the last 10 years," John said. "I just use your cream now and then."
Then there was Samantha, who developed extensive acne at age 8. With such an early start, she seemed headed for a rough adolescence. Yet her face cleared and the acne never recurred.
Felicia, on the other hand, showed up at age 32 with severe, cystic acne. She insisted this had started only 6 months before. "I never had it when I was younger," she said.
I was skeptical, and asked her to show me photos from before the outbreak. Sure enough, a picture taken a year earlier showed a completely unblemished complexion.
Then there was Caroline, who at age 9 had severe psoriasis that was hard to control. Because unpleasant scaling affected her forehead and face, classmates often made comments. I’ll never forget her answer when I asked Caroline how she responded to these remarks. She said, "I tell them, ‘At least my face they can fix!’ "
I lost track of Caroline too. (Patients call more when they’re bothered than when they’re doing well.) Her father visited me years later for issues of his own. "How is Caroline’s psoriasis?" I asked him.
"Went away," he said. "No problems anymore." I’d never have guessed.
What about patients with skin cancer? If someone gets a basal cell carcinoma at age 21 years, you would expect him to be at serious risk for getting many more and want to follow him closely.
So would I, and of course I do. But as the years roll by, many of the patients I’ve seen who fall into this category never get another skin cancer, of whatever kind.
There have been plenty of times when my own track record of anticipating the course of disease has been no better than those of the experts on sports talk radio who predict the outcome of professional football games. By the end of the season, they don’t look so expert, but they go on predicting anyway.
Predictions have consequences. Rheumatologists who prescribe biologic agents have been sending patients for skin checks "because I have a high risk of skin cancer," as do surgeons for people from whom they’ve removed a mildly dysplastic nevus. Skin checks are harmless enough, but thinking of yourself as "high risk" is not conducive to equanimity.
Chronic skin issues, like hair loss, go on for a long time. Unexpected things happen, in both directions. When you take the long view, circumspection is best.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since January 2002.
If you can believe it, I once read a witty article about hair transplants. The authors suggested that the reporting of results should show follow-ups much longer than 6 or 12 months, since hair loss keeps on happening after transplants. What looks fine at 1 year may not look so good 10 years later.
They labeled one figure in their paper as follows: "True long-term follow-up." It was a photo of a tombstone.
Neither medical school nor residency training fosters the long view. You see a patient during a hospitalization for an acute illness. Case presentation focuses on diagnosis, pathogenesis, and treatment for the few days he or she is on the ward. You may follow the patient for at most a few months, or a year after discharge. Those discussing the case might note a prognosis in passing, but don’t give much sense of what is likely to happen to the patient over the course of years, let alone decades.
What actually happens, long after the patient goes home or the residency ends, varies much more than may seem plausible based on the snapshot you get during an acute episode.
Medical practice in the community, by contrast, is a long-haul affair. What you see when you follow patients for years can be quite unexpected.
I think of John, for instance. As a teenager, he had many bouts of widespread and debilitating atopic dermatitis. Topical therapy often failed to make a dent, leading to courses of prednisone that were followed at once by severe recurrences. Had someone asked me at the time, I would have predicted for John a life of miserable itch, and morbidity from systemic treatment.
We lost touch when John went off to college. He returned 15 years later, now all grown up, with a wife and family. He wanted to show me a mole.
"How’s your eczema been?" I asked.
"It’s hardly bothered me much the last 10 years," John said. "I just use your cream now and then."
Then there was Samantha, who developed extensive acne at age 8. With such an early start, she seemed headed for a rough adolescence. Yet her face cleared and the acne never recurred.
Felicia, on the other hand, showed up at age 32 with severe, cystic acne. She insisted this had started only 6 months before. "I never had it when I was younger," she said.
I was skeptical, and asked her to show me photos from before the outbreak. Sure enough, a picture taken a year earlier showed a completely unblemished complexion.
Then there was Caroline, who at age 9 had severe psoriasis that was hard to control. Because unpleasant scaling affected her forehead and face, classmates often made comments. I’ll never forget her answer when I asked Caroline how she responded to these remarks. She said, "I tell them, ‘At least my face they can fix!’ "
I lost track of Caroline too. (Patients call more when they’re bothered than when they’re doing well.) Her father visited me years later for issues of his own. "How is Caroline’s psoriasis?" I asked him.
"Went away," he said. "No problems anymore." I’d never have guessed.
What about patients with skin cancer? If someone gets a basal cell carcinoma at age 21 years, you would expect him to be at serious risk for getting many more and want to follow him closely.
So would I, and of course I do. But as the years roll by, many of the patients I’ve seen who fall into this category never get another skin cancer, of whatever kind.
There have been plenty of times when my own track record of anticipating the course of disease has been no better than those of the experts on sports talk radio who predict the outcome of professional football games. By the end of the season, they don’t look so expert, but they go on predicting anyway.
Predictions have consequences. Rheumatologists who prescribe biologic agents have been sending patients for skin checks "because I have a high risk of skin cancer," as do surgeons for people from whom they’ve removed a mildly dysplastic nevus. Skin checks are harmless enough, but thinking of yourself as "high risk" is not conducive to equanimity.
Chronic skin issues, like hair loss, go on for a long time. Unexpected things happen, in both directions. When you take the long view, circumspection is best.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since January 2002.
If you can believe it, I once read a witty article about hair transplants. The authors suggested that the reporting of results should show follow-ups much longer than 6 or 12 months, since hair loss keeps on happening after transplants. What looks fine at 1 year may not look so good 10 years later.
They labeled one figure in their paper as follows: "True long-term follow-up." It was a photo of a tombstone.
Neither medical school nor residency training fosters the long view. You see a patient during a hospitalization for an acute illness. Case presentation focuses on diagnosis, pathogenesis, and treatment for the few days he or she is on the ward. You may follow the patient for at most a few months, or a year after discharge. Those discussing the case might note a prognosis in passing, but don’t give much sense of what is likely to happen to the patient over the course of years, let alone decades.
What actually happens, long after the patient goes home or the residency ends, varies much more than may seem plausible based on the snapshot you get during an acute episode.
Medical practice in the community, by contrast, is a long-haul affair. What you see when you follow patients for years can be quite unexpected.
I think of John, for instance. As a teenager, he had many bouts of widespread and debilitating atopic dermatitis. Topical therapy often failed to make a dent, leading to courses of prednisone that were followed at once by severe recurrences. Had someone asked me at the time, I would have predicted for John a life of miserable itch, and morbidity from systemic treatment.
We lost touch when John went off to college. He returned 15 years later, now all grown up, with a wife and family. He wanted to show me a mole.
"How’s your eczema been?" I asked.
"It’s hardly bothered me much the last 10 years," John said. "I just use your cream now and then."
Then there was Samantha, who developed extensive acne at age 8. With such an early start, she seemed headed for a rough adolescence. Yet her face cleared and the acne never recurred.
Felicia, on the other hand, showed up at age 32 with severe, cystic acne. She insisted this had started only 6 months before. "I never had it when I was younger," she said.
I was skeptical, and asked her to show me photos from before the outbreak. Sure enough, a picture taken a year earlier showed a completely unblemished complexion.
Then there was Caroline, who at age 9 had severe psoriasis that was hard to control. Because unpleasant scaling affected her forehead and face, classmates often made comments. I’ll never forget her answer when I asked Caroline how she responded to these remarks. She said, "I tell them, ‘At least my face they can fix!’ "
I lost track of Caroline too. (Patients call more when they’re bothered than when they’re doing well.) Her father visited me years later for issues of his own. "How is Caroline’s psoriasis?" I asked him.
"Went away," he said. "No problems anymore." I’d never have guessed.
What about patients with skin cancer? If someone gets a basal cell carcinoma at age 21 years, you would expect him to be at serious risk for getting many more and want to follow him closely.
So would I, and of course I do. But as the years roll by, many of the patients I’ve seen who fall into this category never get another skin cancer, of whatever kind.
There have been plenty of times when my own track record of anticipating the course of disease has been no better than those of the experts on sports talk radio who predict the outcome of professional football games. By the end of the season, they don’t look so expert, but they go on predicting anyway.
Predictions have consequences. Rheumatologists who prescribe biologic agents have been sending patients for skin checks "because I have a high risk of skin cancer," as do surgeons for people from whom they’ve removed a mildly dysplastic nevus. Skin checks are harmless enough, but thinking of yourself as "high risk" is not conducive to equanimity.
Chronic skin issues, like hair loss, go on for a long time. Unexpected things happen, in both directions. When you take the long view, circumspection is best.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years. Dr. Rockoff has contributed to the Under My Skin column in Skin & Allergy News since January 2002.

Vaginal pessaries VIDEO: Proper insertion and removal
Written and narrated by Teresa Tam, MD
For the related article, see: Pessaries for vaginal prolapse: Critical factors to successful fit and continued use Teresa Tam, MD, and Matthew Davies, MD (Surgical Techniques, December 2013)
Written and narrated by Teresa Tam, MD
For the related article, see: Pessaries for vaginal prolapse: Critical factors to successful fit and continued use Teresa Tam, MD, and Matthew Davies, MD (Surgical Techniques, December 2013)
Written and narrated by Teresa Tam, MD
For the related article, see: Pessaries for vaginal prolapse: Critical factors to successful fit and continued use Teresa Tam, MD, and Matthew Davies, MD (Surgical Techniques, December 2013)