User login
Academic Hospitalist Academy Helps Hospitalists Map Career Path

With more than 44,000 hospitalists nationwide, HM continues to grow and change faster than any other medical specialty. That change can be dizzying for academic hospitalists, especially those at the beginning of their careers.
Academic Hospitalist Academy (www.academichospitalist.org), now in its sixth year, helps academic hospitalists map out a rewarding and productive career path in education and scholarship. The academy helps hospitalists:
- Learn how to be effective teachers;
- Understand the process necessary to create and disseminate scholarly work;
- Become aware of the basics of promotion within an academic institution;
- Ascertain the skills necessary to be an asset to their academic institutions;
- Engage the skills necessary to actively participate in a mentor-mentee relationship;
- Understand the business drivers of healthcare; and
- Learn the basics of quality improvement and patient safety.
Academic Hospitalist Academy is an intensive, four-day program that provides a diverse array of learning formats, including didactic sessions, small-group exercises, and skill-building breakout sessions, all facilitated by leaders in the field, with small faculty-to-student ratios. The agenda also includes time for networking activities.
According to a 2013 survey of academy attendees, 100% rated it positively and 99% said they would recommend it to their colleagues.
Tuition is $2,250 for registration before Oct. 13 and $2,500 thereafter.
Academic Hospitalist Academy is co-sponsored by SHM, the Society of General Internal Medicine and the Association of Chiefs and Leaders of General Internal Medicine.
With more than 44,000 hospitalists nationwide, HM continues to grow and change faster than any other medical specialty. That change can be dizzying for academic hospitalists, especially those at the beginning of their careers.
Academic Hospitalist Academy (www.academichospitalist.org), now in its sixth year, helps academic hospitalists map out a rewarding and productive career path in education and scholarship. The academy helps hospitalists:
- Learn how to be effective teachers;
- Understand the process necessary to create and disseminate scholarly work;
- Become aware of the basics of promotion within an academic institution;
- Ascertain the skills necessary to be an asset to their academic institutions;
- Engage the skills necessary to actively participate in a mentor-mentee relationship;
- Understand the business drivers of healthcare; and
- Learn the basics of quality improvement and patient safety.
Academic Hospitalist Academy is an intensive, four-day program that provides a diverse array of learning formats, including didactic sessions, small-group exercises, and skill-building breakout sessions, all facilitated by leaders in the field, with small faculty-to-student ratios. The agenda also includes time for networking activities.
According to a 2013 survey of academy attendees, 100% rated it positively and 99% said they would recommend it to their colleagues.
Tuition is $2,250 for registration before Oct. 13 and $2,500 thereafter.
Academic Hospitalist Academy is co-sponsored by SHM, the Society of General Internal Medicine and the Association of Chiefs and Leaders of General Internal Medicine.
With more than 44,000 hospitalists nationwide, HM continues to grow and change faster than any other medical specialty. That change can be dizzying for academic hospitalists, especially those at the beginning of their careers.
Academic Hospitalist Academy (www.academichospitalist.org), now in its sixth year, helps academic hospitalists map out a rewarding and productive career path in education and scholarship. The academy helps hospitalists:
- Learn how to be effective teachers;
- Understand the process necessary to create and disseminate scholarly work;
- Become aware of the basics of promotion within an academic institution;
- Ascertain the skills necessary to be an asset to their academic institutions;
- Engage the skills necessary to actively participate in a mentor-mentee relationship;
- Understand the business drivers of healthcare; and
- Learn the basics of quality improvement and patient safety.
Academic Hospitalist Academy is an intensive, four-day program that provides a diverse array of learning formats, including didactic sessions, small-group exercises, and skill-building breakout sessions, all facilitated by leaders in the field, with small faculty-to-student ratios. The agenda also includes time for networking activities.
According to a 2013 survey of academy attendees, 100% rated it positively and 99% said they would recommend it to their colleagues.
Tuition is $2,250 for registration before Oct. 13 and $2,500 thereafter.
Academic Hospitalist Academy is co-sponsored by SHM, the Society of General Internal Medicine and the Association of Chiefs and Leaders of General Internal Medicine.
Hospital Medicine Upcoming Events, Meetings, Symposiums
Safety and Brazilian Hospital
Medicine 2014
August 6-8
Rio de Janeiro, Brazil
SHM’s Glycemic Control Program Informational Webinar
August 14, 2 p.m.
https://www4.gotomeeting.com/register/907579183
Palliative Medicine and Supportive Oncology 2014, The 17th International Symposium
September 18-20
Green Valley Ranch, Las Vegas
Society of OB/GYN Hospitalists Annual Clinical Meeting OB/GYN Hospitalists: Recognition, Response, Results
September 18-20
Embassy Suites Downtown, Denver
www.societyofobgynhospitalists.com
Academic Hospitalist Academy
October 20-23
Inverness Hotel and Conference
Center, Englewood, Colo.
Adult Hospital Medicine Boot Camp
October 1-5
The Westin Peachtree Plaza, Atlanta, Ga.
SHM Leadership Academy
November 3-6
Hilton Hawaiian Village Waikiki Beach Resort, Honolulu
www.hospitalmedicine.org/leadership
Hospital Medicine 2015
March 29-April 1, 2015
Gaylord National Resort & Convention Center, National Harbor, Md.
Safety and Brazilian Hospital
Medicine 2014
August 6-8
Rio de Janeiro, Brazil
SHM’s Glycemic Control Program Informational Webinar
August 14, 2 p.m.
https://www4.gotomeeting.com/register/907579183
Palliative Medicine and Supportive Oncology 2014, The 17th International Symposium
September 18-20
Green Valley Ranch, Las Vegas
Society of OB/GYN Hospitalists Annual Clinical Meeting OB/GYN Hospitalists: Recognition, Response, Results
September 18-20
Embassy Suites Downtown, Denver
www.societyofobgynhospitalists.com
Academic Hospitalist Academy
October 20-23
Inverness Hotel and Conference
Center, Englewood, Colo.
Adult Hospital Medicine Boot Camp
October 1-5
The Westin Peachtree Plaza, Atlanta, Ga.
SHM Leadership Academy
November 3-6
Hilton Hawaiian Village Waikiki Beach Resort, Honolulu
www.hospitalmedicine.org/leadership
Hospital Medicine 2015
March 29-April 1, 2015
Gaylord National Resort & Convention Center, National Harbor, Md.
Safety and Brazilian Hospital
Medicine 2014
August 6-8
Rio de Janeiro, Brazil
SHM’s Glycemic Control Program Informational Webinar
August 14, 2 p.m.
https://www4.gotomeeting.com/register/907579183
Palliative Medicine and Supportive Oncology 2014, The 17th International Symposium
September 18-20
Green Valley Ranch, Las Vegas
Society of OB/GYN Hospitalists Annual Clinical Meeting OB/GYN Hospitalists: Recognition, Response, Results
September 18-20
Embassy Suites Downtown, Denver
www.societyofobgynhospitalists.com
Academic Hospitalist Academy
October 20-23
Inverness Hotel and Conference
Center, Englewood, Colo.
Adult Hospital Medicine Boot Camp
October 1-5
The Westin Peachtree Plaza, Atlanta, Ga.
SHM Leadership Academy
November 3-6
Hilton Hawaiian Village Waikiki Beach Resort, Honolulu
www.hospitalmedicine.org/leadership
Hospital Medicine 2015
March 29-April 1, 2015
Gaylord National Resort & Convention Center, National Harbor, Md.
Suctioning Neonates at Birth: Time to Change Our Approach
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing
after wiping or suctioning
Kelleher et al1 studied neonates born after at least 35 weeks gestation, excluding those who had major congenital anomalies or were non-vigorous (depressed muscle tone or respiration, heart rate <100 beats/min, or both) and born into meconium-stained amniotic fluid, as well as those whom they anticipated would need advanced resuscitation. Neonates were randomly assigned to receive either oronasopharyngeal suctioning with a bulb syringe or wiping of the face and mouth with a towel, starting immediately after the umbilical cord was cut and lasting as long as needed while in the delivery room. The primary outcome was the mean respiratory rate in the first 24 hours after birth. The predefined range of clinical equivalence between the 2 groups was a respiratory rate within 4 breaths/min.
Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning,
but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best
if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
…..
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing
after wiping or suctioning
Kelleher et al1 studied neonates born after at least 35 weeks gestation, excluding those who had major congenital anomalies or were non-vigorous (depressed muscle tone or respiration, heart rate <100 beats/min, or both) and born into meconium-stained amniotic fluid, as well as those whom they anticipated would need advanced resuscitation. Neonates were randomly assigned to receive either oronasopharyngeal suctioning with a bulb syringe or wiping of the face and mouth with a towel, starting immediately after the umbilical cord was cut and lasting as long as needed while in the delivery room. The primary outcome was the mean respiratory rate in the first 24 hours after birth. The predefined range of clinical equivalence between the 2 groups was a respiratory rate within 4 breaths/min.
Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning,
but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best
if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
…..
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing
after wiping or suctioning
Kelleher et al1 studied neonates born after at least 35 weeks gestation, excluding those who had major congenital anomalies or were non-vigorous (depressed muscle tone or respiration, heart rate <100 beats/min, or both) and born into meconium-stained amniotic fluid, as well as those whom they anticipated would need advanced resuscitation. Neonates were randomly assigned to receive either oronasopharyngeal suctioning with a bulb syringe or wiping of the face and mouth with a towel, starting immediately after the umbilical cord was cut and lasting as long as needed while in the delivery room. The primary outcome was the mean respiratory rate in the first 24 hours after birth. The predefined range of clinical equivalence between the 2 groups was a respiratory rate within 4 breaths/min.
Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning,
but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best
if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
…..
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
Suctioning neonates at birth: Time to change our approach
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing after wiping or suctioning

Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning, but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing after wiping or suctioning
Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning, but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Stop suctioning neonates at birth. There is no benefit to this practice, and it can cause bradycardia and apnea. Instead, wipe the baby’s mouth and nose with a towel to clear excess secretions and stimulate respiration.1
Strength of recommendation
B: Based on a single randomized equivalency trial.
Kelleher J, Bhat, R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
Illustrative case
A healthy neonate is born through clear amniotic fluid with no meconium. She is vigorous and has no major congenital anomalies. Does she need oronasopharyngeal suctioning?
No, she does not need suctioning. Although it is still standard practice to perform oronasopharyngeal suctioning with a bulb syringe immediately after delivery, multiple studies have found no benefit to routine suctioning.2-7 Guidelines from the Neonatal Resuscitation Program (NRP) and other organizations recommend against the practice, even for neonates born through meconium-stained amniotic fluid.8,9 Suctioning is done because some clinicians believe it reduces the risk of aspiration, especially if there is meconium, and to stimulate breathing, but the evidence suggests that suctioning can stimulate the vagus nerve, which can lead to bradycardia.2 Studies that compared babies who did and didn’t receive suctioning found that those who received it had lower Apgar scores and oxygen saturation levels.2-4
Wiping the neonate’s mouth and nose with a towel is an alternative to suctioning, but until now no trials have compared the outcomes of these 2 methods. Kelleher et al1 conducted an equivalency trial to determine if wiping the mouth and nose is as effective as oronasopharyngeal suctioning.
STUDY SUMMARY: No difference in breathing after wiping or suctioning
Of 506 neonates randomized, 15 were excluded because they were not vigorous and had meconium-stained fluid, and 3 were excluded when their parents withdrew consent. Baseline characteristics for the 2 groups—including maternal age, presence of chronic medical conditions, and body mass index; vaginal vs cesarean delivery; umbilical artery pH; and neonatal sex, ethnic origin, and birth weight—were similar.
In the first 24 hours after birth, the average respiratory rate in the wiping group was 51 breaths/min (standard deviation [SD] ± 8) vs 50 breaths/min (SD ± 6) in the suctioning group. There was no difference in respiratory rates between the 2 groups at 1, 8, or 16 hours after birth. There was also no difference between the 2 groups in Apgar scores or need for advanced resuscitation. More neonates in the wiping group than in the suctioning group were admitted to the neonatal intensive care unit (45 of 246 [18%] vs 30 of 242 [12%]; P=.07), but the study was not powered to assess this outcome.
WHAT'S NEW: Wiping is as effective as suctioning, but there are no adverse effects
This study gives us evidence that wiping the face, mouth, and nose is equivalent to suctioning newborns at delivery, and it supports the NRP recommendation against routine suctioning in vigorous neonates born at term. Wiping avoids the potential adverse effects on the respiratory mucosa, bradycardia, and lower Apgar scores associated with suctioning via bulb syringes.
CAVEATS: Wiping is not best if a neonate’s airway is obstructed
This study looked only at neonates born after 35 weeks’ gestation who did not have meconium-stained amniotic fluid or congenital abnormalities. Also, NRP guidelines do recommend clearing the airways with a bulb syringe or suction catheter if airway obstruction is evident or positive-pressure ventilation is required.8
Another caveat ... In this study,1 there were 98 treatment crossovers: 64 of the 246 neonates in the wiping group received suctioning, and 34 of the 242 neonates in the suctioning group received wiping. However, this was not likely to change the study’s overall conclusion because a per-treatment analysis also found that wiping and suctioning were equivalent.
CHALLENGES TO IMPLEMENTATION: “We’ve always done it this way”
Practice patterns in a delivery room can be difficult to change. As we work on improving our delivery room environment and changing ingrained habits, the evidence from this study should help support the use of wiping in place of suctioning. The transition from suctioning to wiping also would be facilitated by having easily accessible towels designated for wiping.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
1. Kelleher J, Bhat R, Salas AA, et al. Oronasopharyngeal suction versus wiping of the mouth and nose at birth: a randomised equivalency trial. Lancet. 2013;382:326-330.
2. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest. 2006;61:9-14.
3. Gungor S, Teksoz E, Ceyhan T, et al. Oronasopharyngeal suction versus no suction in normal, term and vaginally born infants: a prospective randomized controlled trial. Aust N Z J Obstet Gynaecol. 2005;45:453-456.
4. Carrasco M, Martell M, Estol PC. Oronasopharyngeal suction at birth: effects on arterial oxygen saturation. J Pediatr. 1997;130:832-834.
5. Estol PC, Piriz H, Basalo S, et al. Oro-naso-pharyngeal suction at birth: effects on respiratory adaptation of normal term vaginally born infants. J Perinat Med. 1992;20:297-305.
6. Wiswell TE, Gannon CM, Jacob J, et al. Delivery room management of the apparently vigorous meconium-stained neonate: results of the multicenter, international collaborative trial. Pediatrics. 2000;105(1 pt 1):1-7.
7. Vain NE, Szyld EG, Prudent LM, et al. Oropharyngeal and nasopharyngeal suctioning of meconium-stained neonates before delivery of their shoulders: multicentre, randomized controlled trial. Lancet. 2004;364:597-602.
8. Kattwinkel J, Perlman JM, Aziz K, et al. Part 15: neonatal resuscitation: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 suppl 3):S909-S919.
9. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Pediatrics. 2010;126:e1319-1344.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
Alliance to Advance Patient Nutrition Earns National Recognition
Last year, SHM was one of a number of healthcare and nutrition organizations to join the new Alliance to Advance Patient Nutrition campaign to address nutrition issues for hospitalized patients. In June, the Alliance was honored with the public relations industry’s most distinguished award recognizing the very best campaigns in PR: the Silver Anvil. The award was bestowed by the Public Relations Society of America, and CooperKatz, the firm that launched the campaign, accepted the award on behalf of the team.
The launch of the Alliance was awarded the outstanding public service campaign for 2013.
Last year, SHM was one of a number of healthcare and nutrition organizations to join the new Alliance to Advance Patient Nutrition campaign to address nutrition issues for hospitalized patients. In June, the Alliance was honored with the public relations industry’s most distinguished award recognizing the very best campaigns in PR: the Silver Anvil. The award was bestowed by the Public Relations Society of America, and CooperKatz, the firm that launched the campaign, accepted the award on behalf of the team.
The launch of the Alliance was awarded the outstanding public service campaign for 2013.
Last year, SHM was one of a number of healthcare and nutrition organizations to join the new Alliance to Advance Patient Nutrition campaign to address nutrition issues for hospitalized patients. In June, the Alliance was honored with the public relations industry’s most distinguished award recognizing the very best campaigns in PR: the Silver Anvil. The award was bestowed by the Public Relations Society of America, and CooperKatz, the firm that launched the campaign, accepted the award on behalf of the team.
The launch of the Alliance was awarded the outstanding public service campaign for 2013.
Choosing Wisely Case Competition Deadline Is September 9
Are you helping your hospital choose wisely? You could receive thousands of dollars in return for your good work in providing high-value care to hospitalized patients through SHM’s Choosing Wisely case study competition.
SHM will be awarding a total of $20,000 to hospitalists who submit winning case studies illustrating their implementation of the Choosing Wisely principles published by SHM in 2013. Grand prize winners for both adult and pediatric HM will receive $4,000 each, and three honorable mention winners in both categories will each receive $2,000.
But don’t wait long. The deadline for submissions is September 9. For information and submission forms, visit www.hospitalmedicine.org/choosingwisely.
Are you helping your hospital choose wisely? You could receive thousands of dollars in return for your good work in providing high-value care to hospitalized patients through SHM’s Choosing Wisely case study competition.
SHM will be awarding a total of $20,000 to hospitalists who submit winning case studies illustrating their implementation of the Choosing Wisely principles published by SHM in 2013. Grand prize winners for both adult and pediatric HM will receive $4,000 each, and three honorable mention winners in both categories will each receive $2,000.
But don’t wait long. The deadline for submissions is September 9. For information and submission forms, visit www.hospitalmedicine.org/choosingwisely.
Are you helping your hospital choose wisely? You could receive thousands of dollars in return for your good work in providing high-value care to hospitalized patients through SHM’s Choosing Wisely case study competition.
SHM will be awarding a total of $20,000 to hospitalists who submit winning case studies illustrating their implementation of the Choosing Wisely principles published by SHM in 2013. Grand prize winners for both adult and pediatric HM will receive $4,000 each, and three honorable mention winners in both categories will each receive $2,000.
But don’t wait long. The deadline for submissions is September 9. For information and submission forms, visit www.hospitalmedicine.org/choosingwisely.
Society of Hospital Medicine’s 2015 Fellows Class Applications Welcome
Don’t wait until the last minute to apply for the Fellow and Senior Fellow in Hospital Medicine designation. Start your application today at www.hospitalmedicine.org/fellows.
The FHM and SFHM designation are open to all hospitalists, not just physicians. Physician assistants, nurse practitioners, and practice administrators are all eligible candidates for Fellow status. All inductees will be recognized at a plenary session at HM15 in National Harbor, Md.
The deadline for the 2015 class of Fellows is Jan. 9, 2015.
Don’t wait until the last minute to apply for the Fellow and Senior Fellow in Hospital Medicine designation. Start your application today at www.hospitalmedicine.org/fellows.
The FHM and SFHM designation are open to all hospitalists, not just physicians. Physician assistants, nurse practitioners, and practice administrators are all eligible candidates for Fellow status. All inductees will be recognized at a plenary session at HM15 in National Harbor, Md.
The deadline for the 2015 class of Fellows is Jan. 9, 2015.
Don’t wait until the last minute to apply for the Fellow and Senior Fellow in Hospital Medicine designation. Start your application today at www.hospitalmedicine.org/fellows.
The FHM and SFHM designation are open to all hospitalists, not just physicians. Physician assistants, nurse practitioners, and practice administrators are all eligible candidates for Fellow status. All inductees will be recognized at a plenary session at HM15 in National Harbor, Md.
The deadline for the 2015 class of Fellows is Jan. 9, 2015.
Common Coding Mistakes Hospitalists Should Avoid

Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
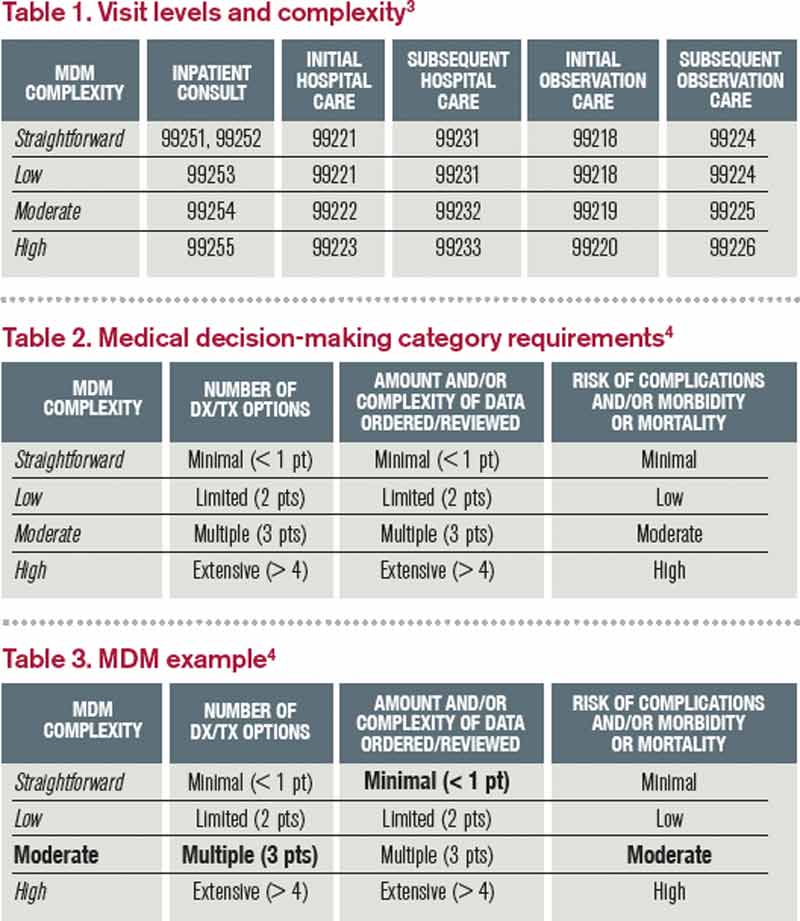
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Society of Hospital Medicine Accepting Pre-Orders for 2014 HM Report
How does your HM group’s productivity stack up against others on productivity? How about compensation? These are the questions that can guide major business decisions for a hospital medicine group, and SHM’s State of Hospital Medicine Report, published every two years, can answer them. The 2014 issue is now available for pre-order and delivery in September.
To order, visit www.hospitalmedicine.org/survey.
How does your HM group’s productivity stack up against others on productivity? How about compensation? These are the questions that can guide major business decisions for a hospital medicine group, and SHM’s State of Hospital Medicine Report, published every two years, can answer them. The 2014 issue is now available for pre-order and delivery in September.
To order, visit www.hospitalmedicine.org/survey.
How does your HM group’s productivity stack up against others on productivity? How about compensation? These are the questions that can guide major business decisions for a hospital medicine group, and SHM’s State of Hospital Medicine Report, published every two years, can answer them. The 2014 issue is now available for pre-order and delivery in September.
To order, visit www.hospitalmedicine.org/survey.
Society of Hospital Medicine’s New Membership Ambassador Program Perks
Do you know someone who should be a part of the HM movement but hasn’t joined SHM? Now you can both win: Your colleague can enjoy all the benefits of SHM membership, and you can receive credits against your future dues. Plus, you’ll get the chance to win a free registration to HM15.
Now through December 31, all active SHM members can earn dues credits and special recognition for recruiting new physician, allied health, or affiliate members. Active members will be eligible for:
- A $35 credit toward 2015-2016 dues when recruiting one new member;
- A $50 credit toward 2015-2016 dues when recruiting two to four new members;
- A $75 credit toward 2015-2016 dues when recruiting five to nine new members; or
- A $125 credit toward 2015-2016 dues when recruiting 10+ new members.
For EVERY member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to Hospital Medicine 2015 in National Harbor, Md.
For details, visit www.hospitalmedicine.org/membership.
Do you know someone who should be a part of the HM movement but hasn’t joined SHM? Now you can both win: Your colleague can enjoy all the benefits of SHM membership, and you can receive credits against your future dues. Plus, you’ll get the chance to win a free registration to HM15.
Now through December 31, all active SHM members can earn dues credits and special recognition for recruiting new physician, allied health, or affiliate members. Active members will be eligible for:
- A $35 credit toward 2015-2016 dues when recruiting one new member;
- A $50 credit toward 2015-2016 dues when recruiting two to four new members;
- A $75 credit toward 2015-2016 dues when recruiting five to nine new members; or
- A $125 credit toward 2015-2016 dues when recruiting 10+ new members.
For EVERY member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to Hospital Medicine 2015 in National Harbor, Md.
For details, visit www.hospitalmedicine.org/membership.
Do you know someone who should be a part of the HM movement but hasn’t joined SHM? Now you can both win: Your colleague can enjoy all the benefits of SHM membership, and you can receive credits against your future dues. Plus, you’ll get the chance to win a free registration to HM15.
Now through December 31, all active SHM members can earn dues credits and special recognition for recruiting new physician, allied health, or affiliate members. Active members will be eligible for:
- A $35 credit toward 2015-2016 dues when recruiting one new member;
- A $50 credit toward 2015-2016 dues when recruiting two to four new members;
- A $75 credit toward 2015-2016 dues when recruiting five to nine new members; or
- A $125 credit toward 2015-2016 dues when recruiting 10+ new members.
For EVERY member recruited, individuals will receive one entry into a grand prize drawing to receive complimentary registration to Hospital Medicine 2015 in National Harbor, Md.
For details, visit www.hospitalmedicine.org/membership.