User login
Radiotherapy planning scans reveal breast cancer patients’ CVD risk
Radiotherapy planning scans may be a rich untapped source of information for estimating the risk of cardiovascular disease (CVD) in breast cancer patients, a large study suggests.

Researchers found that breast cancer patients with a coronary artery calcifications (CAC) score exceeding 400 had nearly four times the adjusted risk of fatal and nonfatal CVD events when compared with patients who had a CAC score of 0.
Patients with scores exceeding 400 also had more than eight times the risk of coronary heart disease events. The associations were especially strong in the subset of patients who received anthracycline-containing chemotherapy.
Helena Verkooijen, MD, PhD, of University Medical Center Utrecht (the Netherlands) presented these findings at the 12th European Breast Cancer Conference.
Dr. Verkooijen noted that, over the past 50 years, breast cancer has dramatically declined as a cause of death among breast cancer survivors, while CVD has continued to account for about 20% of the total deaths in this population.
CACs are sometimes incidentally seen in radiotherapy planning CT scans. “Right now, this information is not often used for patient stratification or informing patients about their cardiovascular risk, and this is a pity, because we know that it is an independent risk factor, and, often, the presence of calcifications can occur in the absence of other cardiovascular risk factors,” Dr. Verkooijen said.
Study details
Dr. Verkooijen and and colleagues from the Bragataston Study Group retrospectively studied 15,919 breast cancer patients who had radiotherapy planning CT scans during 2004-2016 at three Dutch institutions.
The researchers used an automated deep-learning algorithm (described in Radiology) to detect and quantify coronary calcium in planning CT scans and calculate CAC scores, classifying them into five categories.
The median follow-up was 51.6 months. Most women (70%) did not have any calcium detected in their coronary arteries (CAC score of 0), while 3% fell into the highest category (CAC score of >400).
The incidence of nonfatal and fatal CVD events increased with CAC score:
- 5.1% with a score of 0.
- 8.5% with a score of 1-10.
- 13.5% with a score of 11-100.
- 17.6% with a score of 101-400.
- 28.0% with a score greater than 400.
In analyses adjusted for age, laterality of radiation, and receipt of cardiotoxic agents – anthracyclines and trastuzumab – women with a score exceeding 400 had sharply elevated adjusted risks of CVD events (hazard ratio, 3.7), of coronary heart disease events specifically (HR, 8.2), and of death from any cause (HR, 2.8), when compared with peers who had a CAC score of 0.
On further scrutiny of CVD events, the pattern was similar regardless of whether radiation was left- or right-sided. However, the association was stronger among women who received anthracyclines as compared with counterparts who did not, with a nearly six-fold higher risk for those with highest versus lowest CAC scores.
When the women were surveyed, nearly 90% said they wanted to be informed about their CAC score and associated CVD risk, even in the absence of evidence-based risk reduction strategies.
Applying the results
“We believe that this is the first time that anyone has conducted a study on this topic on a scale like this, and we show that it is possible to relatively easily identify women at a very high risk of CVD,” Dr. Verkooijen said. “But what do we do with this information, because these scans are not made to answer this question. … This is information that we get that we haven’t really requested. I think we should only use this information when we have really shown that we can help patients reduce their risk of cardiovascular disease.”
To that end, Dr. Verkooijen and colleagues are planning additional research that will look at the potential benefit of referring high-risk patients for cardioprevention strategies and at the role of using the CAC score to personalize treatment strategies.

“This is an interesting and novel approach to predicting cardiac events for patients undergoing breast cancer treatment,” Meena S. Moran, MD, of Yale University in New Haven, Conn., commented in an interview.
The approach would likely be feasible in typical practice with widespread availability of the automated algorithm and might even alter treatment planning in real time, she said. “From the standpoint of radiation oncology, it would mean running the software to generate a CAC score, which would allow for modifications in decision-making during treatment planning, such as whether or not to include the internal mammary nodal chain in a patient who may be in the ‘gray zone’ for regional nodal radiation. For example, if a patient has a high CAC score, plus if they have received (or are receiving) cardiotoxic drugs, radiation oncologists can use that information as an additional factor to consider in the decision-making of whether or not to include the internal mammary chain, which inevitably can increase the dose delivered to the heart,” Dr. Moran elaborated.
Dr. Verkooijen’s study was supported by the Dutch Cancer Society, the European Commission, the Dutch Digestive Foundation, the Netherlands Organisation for Scientific Research, and Elekta. Dr. Verkooijen and Dr. Moran disclosed no conflicts of interest.
SOURCE: Gal R et al. EBCC-12 Virtual Congress, Abstract 7.
Radiotherapy planning scans may be a rich untapped source of information for estimating the risk of cardiovascular disease (CVD) in breast cancer patients, a large study suggests.
Researchers found that breast cancer patients with a coronary artery calcifications (CAC) score exceeding 400 had nearly four times the adjusted risk of fatal and nonfatal CVD events when compared with patients who had a CAC score of 0.
Patients with scores exceeding 400 also had more than eight times the risk of coronary heart disease events. The associations were especially strong in the subset of patients who received anthracycline-containing chemotherapy.
Helena Verkooijen, MD, PhD, of University Medical Center Utrecht (the Netherlands) presented these findings at the 12th European Breast Cancer Conference.
Dr. Verkooijen noted that, over the past 50 years, breast cancer has dramatically declined as a cause of death among breast cancer survivors, while CVD has continued to account for about 20% of the total deaths in this population.
CACs are sometimes incidentally seen in radiotherapy planning CT scans. “Right now, this information is not often used for patient stratification or informing patients about their cardiovascular risk, and this is a pity, because we know that it is an independent risk factor, and, often, the presence of calcifications can occur in the absence of other cardiovascular risk factors,” Dr. Verkooijen said.
Study details
Dr. Verkooijen and and colleagues from the Bragataston Study Group retrospectively studied 15,919 breast cancer patients who had radiotherapy planning CT scans during 2004-2016 at three Dutch institutions.
The researchers used an automated deep-learning algorithm (described in Radiology) to detect and quantify coronary calcium in planning CT scans and calculate CAC scores, classifying them into five categories.
The median follow-up was 51.6 months. Most women (70%) did not have any calcium detected in their coronary arteries (CAC score of 0), while 3% fell into the highest category (CAC score of >400).
The incidence of nonfatal and fatal CVD events increased with CAC score:
- 5.1% with a score of 0.
- 8.5% with a score of 1-10.
- 13.5% with a score of 11-100.
- 17.6% with a score of 101-400.
- 28.0% with a score greater than 400.
In analyses adjusted for age, laterality of radiation, and receipt of cardiotoxic agents – anthracyclines and trastuzumab – women with a score exceeding 400 had sharply elevated adjusted risks of CVD events (hazard ratio, 3.7), of coronary heart disease events specifically (HR, 8.2), and of death from any cause (HR, 2.8), when compared with peers who had a CAC score of 0.
On further scrutiny of CVD events, the pattern was similar regardless of whether radiation was left- or right-sided. However, the association was stronger among women who received anthracyclines as compared with counterparts who did not, with a nearly six-fold higher risk for those with highest versus lowest CAC scores.
When the women were surveyed, nearly 90% said they wanted to be informed about their CAC score and associated CVD risk, even in the absence of evidence-based risk reduction strategies.
Applying the results
“We believe that this is the first time that anyone has conducted a study on this topic on a scale like this, and we show that it is possible to relatively easily identify women at a very high risk of CVD,” Dr. Verkooijen said. “But what do we do with this information, because these scans are not made to answer this question. … This is information that we get that we haven’t really requested. I think we should only use this information when we have really shown that we can help patients reduce their risk of cardiovascular disease.”
To that end, Dr. Verkooijen and colleagues are planning additional research that will look at the potential benefit of referring high-risk patients for cardioprevention strategies and at the role of using the CAC score to personalize treatment strategies.
“This is an interesting and novel approach to predicting cardiac events for patients undergoing breast cancer treatment,” Meena S. Moran, MD, of Yale University in New Haven, Conn., commented in an interview.
The approach would likely be feasible in typical practice with widespread availability of the automated algorithm and might even alter treatment planning in real time, she said. “From the standpoint of radiation oncology, it would mean running the software to generate a CAC score, which would allow for modifications in decision-making during treatment planning, such as whether or not to include the internal mammary nodal chain in a patient who may be in the ‘gray zone’ for regional nodal radiation. For example, if a patient has a high CAC score, plus if they have received (or are receiving) cardiotoxic drugs, radiation oncologists can use that information as an additional factor to consider in the decision-making of whether or not to include the internal mammary chain, which inevitably can increase the dose delivered to the heart,” Dr. Moran elaborated.
Dr. Verkooijen’s study was supported by the Dutch Cancer Society, the European Commission, the Dutch Digestive Foundation, the Netherlands Organisation for Scientific Research, and Elekta. Dr. Verkooijen and Dr. Moran disclosed no conflicts of interest.
SOURCE: Gal R et al. EBCC-12 Virtual Congress, Abstract 7.
Radiotherapy planning scans may be a rich untapped source of information for estimating the risk of cardiovascular disease (CVD) in breast cancer patients, a large study suggests.
Researchers found that breast cancer patients with a coronary artery calcifications (CAC) score exceeding 400 had nearly four times the adjusted risk of fatal and nonfatal CVD events when compared with patients who had a CAC score of 0.
Patients with scores exceeding 400 also had more than eight times the risk of coronary heart disease events. The associations were especially strong in the subset of patients who received anthracycline-containing chemotherapy.
Helena Verkooijen, MD, PhD, of University Medical Center Utrecht (the Netherlands) presented these findings at the 12th European Breast Cancer Conference.
Dr. Verkooijen noted that, over the past 50 years, breast cancer has dramatically declined as a cause of death among breast cancer survivors, while CVD has continued to account for about 20% of the total deaths in this population.
CACs are sometimes incidentally seen in radiotherapy planning CT scans. “Right now, this information is not often used for patient stratification or informing patients about their cardiovascular risk, and this is a pity, because we know that it is an independent risk factor, and, often, the presence of calcifications can occur in the absence of other cardiovascular risk factors,” Dr. Verkooijen said.
Study details
Dr. Verkooijen and and colleagues from the Bragataston Study Group retrospectively studied 15,919 breast cancer patients who had radiotherapy planning CT scans during 2004-2016 at three Dutch institutions.
The researchers used an automated deep-learning algorithm (described in Radiology) to detect and quantify coronary calcium in planning CT scans and calculate CAC scores, classifying them into five categories.
The median follow-up was 51.6 months. Most women (70%) did not have any calcium detected in their coronary arteries (CAC score of 0), while 3% fell into the highest category (CAC score of >400).
The incidence of nonfatal and fatal CVD events increased with CAC score:
- 5.1% with a score of 0.
- 8.5% with a score of 1-10.
- 13.5% with a score of 11-100.
- 17.6% with a score of 101-400.
- 28.0% with a score greater than 400.
In analyses adjusted for age, laterality of radiation, and receipt of cardiotoxic agents – anthracyclines and trastuzumab – women with a score exceeding 400 had sharply elevated adjusted risks of CVD events (hazard ratio, 3.7), of coronary heart disease events specifically (HR, 8.2), and of death from any cause (HR, 2.8), when compared with peers who had a CAC score of 0.
On further scrutiny of CVD events, the pattern was similar regardless of whether radiation was left- or right-sided. However, the association was stronger among women who received anthracyclines as compared with counterparts who did not, with a nearly six-fold higher risk for those with highest versus lowest CAC scores.
When the women were surveyed, nearly 90% said they wanted to be informed about their CAC score and associated CVD risk, even in the absence of evidence-based risk reduction strategies.
Applying the results
“We believe that this is the first time that anyone has conducted a study on this topic on a scale like this, and we show that it is possible to relatively easily identify women at a very high risk of CVD,” Dr. Verkooijen said. “But what do we do with this information, because these scans are not made to answer this question. … This is information that we get that we haven’t really requested. I think we should only use this information when we have really shown that we can help patients reduce their risk of cardiovascular disease.”
To that end, Dr. Verkooijen and colleagues are planning additional research that will look at the potential benefit of referring high-risk patients for cardioprevention strategies and at the role of using the CAC score to personalize treatment strategies.
“This is an interesting and novel approach to predicting cardiac events for patients undergoing breast cancer treatment,” Meena S. Moran, MD, of Yale University in New Haven, Conn., commented in an interview.
The approach would likely be feasible in typical practice with widespread availability of the automated algorithm and might even alter treatment planning in real time, she said. “From the standpoint of radiation oncology, it would mean running the software to generate a CAC score, which would allow for modifications in decision-making during treatment planning, such as whether or not to include the internal mammary nodal chain in a patient who may be in the ‘gray zone’ for regional nodal radiation. For example, if a patient has a high CAC score, plus if they have received (or are receiving) cardiotoxic drugs, radiation oncologists can use that information as an additional factor to consider in the decision-making of whether or not to include the internal mammary chain, which inevitably can increase the dose delivered to the heart,” Dr. Moran elaborated.
Dr. Verkooijen’s study was supported by the Dutch Cancer Society, the European Commission, the Dutch Digestive Foundation, the Netherlands Organisation for Scientific Research, and Elekta. Dr. Verkooijen and Dr. Moran disclosed no conflicts of interest.
SOURCE: Gal R et al. EBCC-12 Virtual Congress, Abstract 7.
FROM EBCC-12 VIRTUAL CONFERENCE

INR fails to predict bleeding in patients with cirrhosis
International normalized ratio (INR) does not predict periprocedural bleeding in patients with cirrhosis, according to a meta-analysis of 29 studies.
This finding should deter the common practice of delivering blood products to cirrhotic patients with an elevated INR, reported lead author Alexander J. Kovalic, MD, of Novant Forsyth Medical Center in Winston Salem, N.C., and colleagues.
“INR measurement among cirrhotic patients is important in MELD [Model for End-Stage Liver Disease] prognostication and assessment of underlying hepatic synthetic function, however the INR alone does not capture the complicated interplay of anticoagulant and procoagulant deficiencies present in cirrhotic coagulopathy,” Dr. Kovalic and colleagues wrote in Alimentary Pharmacology & Therapeutics. “Yet, the ‘correction’ of these aberrancies among peripheral coagulation tests remains common ... even in modern practice, and not uncommonly occurs in the periprocedural setting.”
According to investigators, addressing INR with blood transfusion can have a litany of negative effects. Beyond the risks faced by all patient populations, increasing blood volume in those with cirrhosis can increase portal venous pressure, thereby raising risks of portal gastropathy or variceal hemorrhage. In addition, giving plasma products to patients with cirrhotic coagulopathy may further disrupt the balance between anticoagulants and procoagulants, potentially triggering disseminated intravascular coagulation.
Dr. Kovalic and colleagues noted that the lack of correlation between peripheral coagulation tests and bleeding risk has been a longstanding subject of investigation, citing studies from as early as 1981.
To add further weight to this body of evidence, the investigators conducted a systematic review and meta-analysis involving 13,276 patients with cirrhosis who underwent various procedures between 1999 and 2019. Primary outcomes included periprocedural bleeding events and the association between preprocedural INR and periprocedural bleeding events. Secondary outcomes included mortality, quantity of blood and/or plasma products used, and relationship between preprocedural platelet count and periprocedural bleeding events.
The analysis showed that preprocedural INR was not significantly associated with periprocedural bleeding events (pooled odds ratio, 1.52; 95% confidence interval, 0.99-2.33; P = .06), a finding that held across INR threshold subgroups. Similarly, no significant difference was found between mean INR of patients who had bleeding events versus that of those who did not (pooled mean difference, 0.05; 95% CI, 0.03-0.13; P = .23).
Preprocedural platelet count was also a poor predictor of periprocedural bleeding, with a pooled odds ratio of 1.24 (95% CI, 0.55-2.77; P = .60), although the investigators noted that platelet count thresholds varied widely across studies, from 30 to 150 × 109/L. When studies were stratified by procedural bleeding risk or procedure type, subgroup effects were no longer significant. Other secondary endpoints were incalculable because of insufficient data.
“Hopefully, these findings will spark initiation of more large-scale, higher-quality studies ... to reinforce minimizing administration of fresh frozen plasma for inappropriate correction of INR, which carries a multitude of adverse effects among cirrhotic [patients],” the investigators concluded.

According to Stephen H. Caldwell, MD, of the University of Virginia in Charlottesville, “The present paper augments accumulating literature over the past 15 years that INR should be discarded as a measure of procedure-related bleeding risk.”
Dr. Caldwell pointed out that “bleeding in cirrhosis is usually related to portal hypertension not with impaired hemostasis, with the occasional exception of hyperfibrinolysis, which is very different from a prolonged INR.”
He went on to suggest that the present findings should dissuade clinicians from a practice that, for some, is reflexive rather than evidence based.
“It’s remarkable how many medical practices become entrenched based on hand-me-down teaching during our early training years, and remain so for many years beyond as we disperse into various medical and surgical fields,” Dr. Caldwell said. “These learned approaches to common problems can clearly persist for generations despite overwhelming evidence to the contrary that usually evolve slowly and well-insulated within subspecialties or sub-subspecialties, and hence take several generations of training to diffuse into the wider practice of medical care for common problems. These may become matters of expedience in decision-making, much like the old antibiotic conundrum of ‘no-think-a-cillin,’ as critics referred to over-use of broad spectrum antibiotics. And so it has been with the INR.”The investigators disclosed relationships with AbbVie, Eisai, Gilead, and others. Dr. Caldwell disclosed research support from Daiichi concerning the potential role of anticoagulation therapy in preventing cirrhosis progression.
SOURCE: Kovalic AJ et al. Aliment Pharmacol Ther. 2020 Sep 10. doi: 10.1111/apt.16078.
International normalized ratio (INR) does not predict periprocedural bleeding in patients with cirrhosis, according to a meta-analysis of 29 studies.
This finding should deter the common practice of delivering blood products to cirrhotic patients with an elevated INR, reported lead author Alexander J. Kovalic, MD, of Novant Forsyth Medical Center in Winston Salem, N.C., and colleagues.
“INR measurement among cirrhotic patients is important in MELD [Model for End-Stage Liver Disease] prognostication and assessment of underlying hepatic synthetic function, however the INR alone does not capture the complicated interplay of anticoagulant and procoagulant deficiencies present in cirrhotic coagulopathy,” Dr. Kovalic and colleagues wrote in Alimentary Pharmacology & Therapeutics. “Yet, the ‘correction’ of these aberrancies among peripheral coagulation tests remains common ... even in modern practice, and not uncommonly occurs in the periprocedural setting.”
According to investigators, addressing INR with blood transfusion can have a litany of negative effects. Beyond the risks faced by all patient populations, increasing blood volume in those with cirrhosis can increase portal venous pressure, thereby raising risks of portal gastropathy or variceal hemorrhage. In addition, giving plasma products to patients with cirrhotic coagulopathy may further disrupt the balance between anticoagulants and procoagulants, potentially triggering disseminated intravascular coagulation.
Dr. Kovalic and colleagues noted that the lack of correlation between peripheral coagulation tests and bleeding risk has been a longstanding subject of investigation, citing studies from as early as 1981.
To add further weight to this body of evidence, the investigators conducted a systematic review and meta-analysis involving 13,276 patients with cirrhosis who underwent various procedures between 1999 and 2019. Primary outcomes included periprocedural bleeding events and the association between preprocedural INR and periprocedural bleeding events. Secondary outcomes included mortality, quantity of blood and/or plasma products used, and relationship between preprocedural platelet count and periprocedural bleeding events.
The analysis showed that preprocedural INR was not significantly associated with periprocedural bleeding events (pooled odds ratio, 1.52; 95% confidence interval, 0.99-2.33; P = .06), a finding that held across INR threshold subgroups. Similarly, no significant difference was found between mean INR of patients who had bleeding events versus that of those who did not (pooled mean difference, 0.05; 95% CI, 0.03-0.13; P = .23).
Preprocedural platelet count was also a poor predictor of periprocedural bleeding, with a pooled odds ratio of 1.24 (95% CI, 0.55-2.77; P = .60), although the investigators noted that platelet count thresholds varied widely across studies, from 30 to 150 × 109/L. When studies were stratified by procedural bleeding risk or procedure type, subgroup effects were no longer significant. Other secondary endpoints were incalculable because of insufficient data.
“Hopefully, these findings will spark initiation of more large-scale, higher-quality studies ... to reinforce minimizing administration of fresh frozen plasma for inappropriate correction of INR, which carries a multitude of adverse effects among cirrhotic [patients],” the investigators concluded.
According to Stephen H. Caldwell, MD, of the University of Virginia in Charlottesville, “The present paper augments accumulating literature over the past 15 years that INR should be discarded as a measure of procedure-related bleeding risk.”
Dr. Caldwell pointed out that “bleeding in cirrhosis is usually related to portal hypertension not with impaired hemostasis, with the occasional exception of hyperfibrinolysis, which is very different from a prolonged INR.”
He went on to suggest that the present findings should dissuade clinicians from a practice that, for some, is reflexive rather than evidence based.
“It’s remarkable how many medical practices become entrenched based on hand-me-down teaching during our early training years, and remain so for many years beyond as we disperse into various medical and surgical fields,” Dr. Caldwell said. “These learned approaches to common problems can clearly persist for generations despite overwhelming evidence to the contrary that usually evolve slowly and well-insulated within subspecialties or sub-subspecialties, and hence take several generations of training to diffuse into the wider practice of medical care for common problems. These may become matters of expedience in decision-making, much like the old antibiotic conundrum of ‘no-think-a-cillin,’ as critics referred to over-use of broad spectrum antibiotics. And so it has been with the INR.”The investigators disclosed relationships with AbbVie, Eisai, Gilead, and others. Dr. Caldwell disclosed research support from Daiichi concerning the potential role of anticoagulation therapy in preventing cirrhosis progression.
SOURCE: Kovalic AJ et al. Aliment Pharmacol Ther. 2020 Sep 10. doi: 10.1111/apt.16078.
International normalized ratio (INR) does not predict periprocedural bleeding in patients with cirrhosis, according to a meta-analysis of 29 studies.
This finding should deter the common practice of delivering blood products to cirrhotic patients with an elevated INR, reported lead author Alexander J. Kovalic, MD, of Novant Forsyth Medical Center in Winston Salem, N.C., and colleagues.
“INR measurement among cirrhotic patients is important in MELD [Model for End-Stage Liver Disease] prognostication and assessment of underlying hepatic synthetic function, however the INR alone does not capture the complicated interplay of anticoagulant and procoagulant deficiencies present in cirrhotic coagulopathy,” Dr. Kovalic and colleagues wrote in Alimentary Pharmacology & Therapeutics. “Yet, the ‘correction’ of these aberrancies among peripheral coagulation tests remains common ... even in modern practice, and not uncommonly occurs in the periprocedural setting.”
According to investigators, addressing INR with blood transfusion can have a litany of negative effects. Beyond the risks faced by all patient populations, increasing blood volume in those with cirrhosis can increase portal venous pressure, thereby raising risks of portal gastropathy or variceal hemorrhage. In addition, giving plasma products to patients with cirrhotic coagulopathy may further disrupt the balance between anticoagulants and procoagulants, potentially triggering disseminated intravascular coagulation.
Dr. Kovalic and colleagues noted that the lack of correlation between peripheral coagulation tests and bleeding risk has been a longstanding subject of investigation, citing studies from as early as 1981.
To add further weight to this body of evidence, the investigators conducted a systematic review and meta-analysis involving 13,276 patients with cirrhosis who underwent various procedures between 1999 and 2019. Primary outcomes included periprocedural bleeding events and the association between preprocedural INR and periprocedural bleeding events. Secondary outcomes included mortality, quantity of blood and/or plasma products used, and relationship between preprocedural platelet count and periprocedural bleeding events.
The analysis showed that preprocedural INR was not significantly associated with periprocedural bleeding events (pooled odds ratio, 1.52; 95% confidence interval, 0.99-2.33; P = .06), a finding that held across INR threshold subgroups. Similarly, no significant difference was found between mean INR of patients who had bleeding events versus that of those who did not (pooled mean difference, 0.05; 95% CI, 0.03-0.13; P = .23).
Preprocedural platelet count was also a poor predictor of periprocedural bleeding, with a pooled odds ratio of 1.24 (95% CI, 0.55-2.77; P = .60), although the investigators noted that platelet count thresholds varied widely across studies, from 30 to 150 × 109/L. When studies were stratified by procedural bleeding risk or procedure type, subgroup effects were no longer significant. Other secondary endpoints were incalculable because of insufficient data.
“Hopefully, these findings will spark initiation of more large-scale, higher-quality studies ... to reinforce minimizing administration of fresh frozen plasma for inappropriate correction of INR, which carries a multitude of adverse effects among cirrhotic [patients],” the investigators concluded.
According to Stephen H. Caldwell, MD, of the University of Virginia in Charlottesville, “The present paper augments accumulating literature over the past 15 years that INR should be discarded as a measure of procedure-related bleeding risk.”
Dr. Caldwell pointed out that “bleeding in cirrhosis is usually related to portal hypertension not with impaired hemostasis, with the occasional exception of hyperfibrinolysis, which is very different from a prolonged INR.”
He went on to suggest that the present findings should dissuade clinicians from a practice that, for some, is reflexive rather than evidence based.
“It’s remarkable how many medical practices become entrenched based on hand-me-down teaching during our early training years, and remain so for many years beyond as we disperse into various medical and surgical fields,” Dr. Caldwell said. “These learned approaches to common problems can clearly persist for generations despite overwhelming evidence to the contrary that usually evolve slowly and well-insulated within subspecialties or sub-subspecialties, and hence take several generations of training to diffuse into the wider practice of medical care for common problems. These may become matters of expedience in decision-making, much like the old antibiotic conundrum of ‘no-think-a-cillin,’ as critics referred to over-use of broad spectrum antibiotics. And so it has been with the INR.”The investigators disclosed relationships with AbbVie, Eisai, Gilead, and others. Dr. Caldwell disclosed research support from Daiichi concerning the potential role of anticoagulation therapy in preventing cirrhosis progression.
SOURCE: Kovalic AJ et al. Aliment Pharmacol Ther. 2020 Sep 10. doi: 10.1111/apt.16078.
FROM ALIMENTARY PHARMACOLOGY & THERAPEUTICS

EMPEROR-Reduced: Empagliflozin’s HFrEF benefit holds steady on top of sacubitril/valsartan
The latest drug shown to benefit patients with heart failure with reduced ejection fraction, the SGLT2 inhibitor empagliflozin, works just as well when added on top of a second major agent used to treat these patients, the renin-angiotensin system–inhibiting combination of sacubitril/valsartan, based on a post-hoc analysis of data from the EMPEROR-Reduced trial.

“When there are two very effective treatments, it’s common for people to ask: Which should I use?’ The goal of my presentation was to emphasize that the answer is both. We shouldn’t choose between neprilysin inhibition [sacubitril inhibits the enzyme neprilysin] and SGLT2 [sodium-glucose transporter 2] inhibition; we should use both,” said Milton Packer, MD at the virtual annual meeting of the Heart Failure Society of America.
EMPEROR-Reduced had the primary goal of testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in patients with heart failure with reduced ejection fraction (HFrEF). The results showed that adding this drug on top of standard treatments led to a 25% relative cut in the study’s primary efficacy endpoint, compared with placebo, and had this effect regardless of whether or not patients also had type 2 diabetes (N Engl J Med. 2020 Aug 29. doi: 10.1056/NEJMoa2022190).
Among the 3,730 patients enrolled in the trial, 727 (19%) were on sacubitril/valsartan (Entresto) at entry, which gave Dr. Packer the data to perform the analysis he reported. He presented the study’s three major endpoints as well as a quality of life analysis that compared the performance of empagliflozin in patients who were on sacubitril/valsartan at baseline with the other study patients, who were either on a different type of renin-angiotensin system (RAS) blocker (roughly 70% of study patients) or on no RAS inhibition (about 10% of patients).
The results showed no statistically significant indication of an interaction, suggesting that patients with sacubitril/valsartan on board had just as good response to empagliflozin as patients who were not on this combination. The landmark PARADIGM-HF trial proved several years ago that treatment of HFrEF patients with sacubitril/valsartan led to significantly better outcomes than did treatment with another form of RAS inhibition (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
For example, EMPEROR-Reduced’s primary endpoint, the combined rate of cardiovascular death or hospitalization for heart failure, fell by 36% relative to placebo in patients who received empagliflozin on top of sacubitril/valsartan, and by 23% relative to placebo among the remaining patients who received empagliflozin on top of a different type of RAS inhibitor drug or no RAS inhibition.
“Background treatment with sacubitril/valsartan did not diminish, and may have enhanced the efficacy of empagliflozin,” concluded Dr. Packer. Further analyses also showed that concurrent sacubitril/valsartan had no statistically significant impact on empagliflozin’s ability to reduce the rate of total heart failure hospitalizations, or to slow progressive loss of renal function, compared with placebo. The fourth efficacy analysis Dr. Packer presented showed that empagliflozin was also as effective for improving a quality-of-life measure in patients compared with placebo regardless of the type of RAS inhibition used. For all four outcomes, the point-estimate of empagliflozin’s benefit was higher when used along with sacubitril/valsartan.
Brian L. Claggett, PhD, a biostatistician at Brigham and Women’s Hospital and Harvard Medical School in Boston, designated discussant for the report, disagreed with Dr. Packer’s suggestion that the efficacy of empagliflozin may have been greater when administered against a background of sacubitril/valsartan. From a statistical perspective, there is no basis to suggest that patients did better when they were on both drugs, he cautioned. But Dr. Claggett acknowledged that the new analyses suggested that empagliflozin’s benefit wasn’t compromised by concurrent sacubitril/valsartan use. He also highlighted the value of more fully documenting the safety and efficacy of a new drug when used as part of “comprehensive therapy” with the established drugs that a patient may concurrently receive.
Dr. Packer also presented several measures of treatment safety that all showed similar rates of adverse effects between the empagliflozin and placebo recipients regardless of background RAS inhibition. A notable finding was that the incidence of hypokalemia was 5.9% in patients on empagliflozin and sacubitril/valsartan and 7.5% among patients on empagliflozin and a different type of RAS inhibition.
EMPEROR-Reduced was funded by Boehringer Ingelheim and Eli Lilly, the companies that market empagliflozin. Dr. Packer has received personal fees from Boehringer Ingelheim and Eli Lilly and from several other companies. Dr. Claggett has been a consultant to Amgen, AO Biome, Biogen, Corvia, Myokardia, and Novartis.
The latest drug shown to benefit patients with heart failure with reduced ejection fraction, the SGLT2 inhibitor empagliflozin, works just as well when added on top of a second major agent used to treat these patients, the renin-angiotensin system–inhibiting combination of sacubitril/valsartan, based on a post-hoc analysis of data from the EMPEROR-Reduced trial.
“When there are two very effective treatments, it’s common for people to ask: Which should I use?’ The goal of my presentation was to emphasize that the answer is both. We shouldn’t choose between neprilysin inhibition [sacubitril inhibits the enzyme neprilysin] and SGLT2 [sodium-glucose transporter 2] inhibition; we should use both,” said Milton Packer, MD at the virtual annual meeting of the Heart Failure Society of America.
EMPEROR-Reduced had the primary goal of testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in patients with heart failure with reduced ejection fraction (HFrEF). The results showed that adding this drug on top of standard treatments led to a 25% relative cut in the study’s primary efficacy endpoint, compared with placebo, and had this effect regardless of whether or not patients also had type 2 diabetes (N Engl J Med. 2020 Aug 29. doi: 10.1056/NEJMoa2022190).
Among the 3,730 patients enrolled in the trial, 727 (19%) were on sacubitril/valsartan (Entresto) at entry, which gave Dr. Packer the data to perform the analysis he reported. He presented the study’s three major endpoints as well as a quality of life analysis that compared the performance of empagliflozin in patients who were on sacubitril/valsartan at baseline with the other study patients, who were either on a different type of renin-angiotensin system (RAS) blocker (roughly 70% of study patients) or on no RAS inhibition (about 10% of patients).
The results showed no statistically significant indication of an interaction, suggesting that patients with sacubitril/valsartan on board had just as good response to empagliflozin as patients who were not on this combination. The landmark PARADIGM-HF trial proved several years ago that treatment of HFrEF patients with sacubitril/valsartan led to significantly better outcomes than did treatment with another form of RAS inhibition (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
For example, EMPEROR-Reduced’s primary endpoint, the combined rate of cardiovascular death or hospitalization for heart failure, fell by 36% relative to placebo in patients who received empagliflozin on top of sacubitril/valsartan, and by 23% relative to placebo among the remaining patients who received empagliflozin on top of a different type of RAS inhibitor drug or no RAS inhibition.
“Background treatment with sacubitril/valsartan did not diminish, and may have enhanced the efficacy of empagliflozin,” concluded Dr. Packer. Further analyses also showed that concurrent sacubitril/valsartan had no statistically significant impact on empagliflozin’s ability to reduce the rate of total heart failure hospitalizations, or to slow progressive loss of renal function, compared with placebo. The fourth efficacy analysis Dr. Packer presented showed that empagliflozin was also as effective for improving a quality-of-life measure in patients compared with placebo regardless of the type of RAS inhibition used. For all four outcomes, the point-estimate of empagliflozin’s benefit was higher when used along with sacubitril/valsartan.
Brian L. Claggett, PhD, a biostatistician at Brigham and Women’s Hospital and Harvard Medical School in Boston, designated discussant for the report, disagreed with Dr. Packer’s suggestion that the efficacy of empagliflozin may have been greater when administered against a background of sacubitril/valsartan. From a statistical perspective, there is no basis to suggest that patients did better when they were on both drugs, he cautioned. But Dr. Claggett acknowledged that the new analyses suggested that empagliflozin’s benefit wasn’t compromised by concurrent sacubitril/valsartan use. He also highlighted the value of more fully documenting the safety and efficacy of a new drug when used as part of “comprehensive therapy” with the established drugs that a patient may concurrently receive.
Dr. Packer also presented several measures of treatment safety that all showed similar rates of adverse effects between the empagliflozin and placebo recipients regardless of background RAS inhibition. A notable finding was that the incidence of hypokalemia was 5.9% in patients on empagliflozin and sacubitril/valsartan and 7.5% among patients on empagliflozin and a different type of RAS inhibition.
EMPEROR-Reduced was funded by Boehringer Ingelheim and Eli Lilly, the companies that market empagliflozin. Dr. Packer has received personal fees from Boehringer Ingelheim and Eli Lilly and from several other companies. Dr. Claggett has been a consultant to Amgen, AO Biome, Biogen, Corvia, Myokardia, and Novartis.
The latest drug shown to benefit patients with heart failure with reduced ejection fraction, the SGLT2 inhibitor empagliflozin, works just as well when added on top of a second major agent used to treat these patients, the renin-angiotensin system–inhibiting combination of sacubitril/valsartan, based on a post-hoc analysis of data from the EMPEROR-Reduced trial.
“When there are two very effective treatments, it’s common for people to ask: Which should I use?’ The goal of my presentation was to emphasize that the answer is both. We shouldn’t choose between neprilysin inhibition [sacubitril inhibits the enzyme neprilysin] and SGLT2 [sodium-glucose transporter 2] inhibition; we should use both,” said Milton Packer, MD at the virtual annual meeting of the Heart Failure Society of America.
EMPEROR-Reduced had the primary goal of testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in patients with heart failure with reduced ejection fraction (HFrEF). The results showed that adding this drug on top of standard treatments led to a 25% relative cut in the study’s primary efficacy endpoint, compared with placebo, and had this effect regardless of whether or not patients also had type 2 diabetes (N Engl J Med. 2020 Aug 29. doi: 10.1056/NEJMoa2022190).
Among the 3,730 patients enrolled in the trial, 727 (19%) were on sacubitril/valsartan (Entresto) at entry, which gave Dr. Packer the data to perform the analysis he reported. He presented the study’s three major endpoints as well as a quality of life analysis that compared the performance of empagliflozin in patients who were on sacubitril/valsartan at baseline with the other study patients, who were either on a different type of renin-angiotensin system (RAS) blocker (roughly 70% of study patients) or on no RAS inhibition (about 10% of patients).
The results showed no statistically significant indication of an interaction, suggesting that patients with sacubitril/valsartan on board had just as good response to empagliflozin as patients who were not on this combination. The landmark PARADIGM-HF trial proved several years ago that treatment of HFrEF patients with sacubitril/valsartan led to significantly better outcomes than did treatment with another form of RAS inhibition (N Engl J Med. 2014 Sep 11;371[11]:993-1004).
For example, EMPEROR-Reduced’s primary endpoint, the combined rate of cardiovascular death or hospitalization for heart failure, fell by 36% relative to placebo in patients who received empagliflozin on top of sacubitril/valsartan, and by 23% relative to placebo among the remaining patients who received empagliflozin on top of a different type of RAS inhibitor drug or no RAS inhibition.
“Background treatment with sacubitril/valsartan did not diminish, and may have enhanced the efficacy of empagliflozin,” concluded Dr. Packer. Further analyses also showed that concurrent sacubitril/valsartan had no statistically significant impact on empagliflozin’s ability to reduce the rate of total heart failure hospitalizations, or to slow progressive loss of renal function, compared with placebo. The fourth efficacy analysis Dr. Packer presented showed that empagliflozin was also as effective for improving a quality-of-life measure in patients compared with placebo regardless of the type of RAS inhibition used. For all four outcomes, the point-estimate of empagliflozin’s benefit was higher when used along with sacubitril/valsartan.
Brian L. Claggett, PhD, a biostatistician at Brigham and Women’s Hospital and Harvard Medical School in Boston, designated discussant for the report, disagreed with Dr. Packer’s suggestion that the efficacy of empagliflozin may have been greater when administered against a background of sacubitril/valsartan. From a statistical perspective, there is no basis to suggest that patients did better when they were on both drugs, he cautioned. But Dr. Claggett acknowledged that the new analyses suggested that empagliflozin’s benefit wasn’t compromised by concurrent sacubitril/valsartan use. He also highlighted the value of more fully documenting the safety and efficacy of a new drug when used as part of “comprehensive therapy” with the established drugs that a patient may concurrently receive.
Dr. Packer also presented several measures of treatment safety that all showed similar rates of adverse effects between the empagliflozin and placebo recipients regardless of background RAS inhibition. A notable finding was that the incidence of hypokalemia was 5.9% in patients on empagliflozin and sacubitril/valsartan and 7.5% among patients on empagliflozin and a different type of RAS inhibition.
EMPEROR-Reduced was funded by Boehringer Ingelheim and Eli Lilly, the companies that market empagliflozin. Dr. Packer has received personal fees from Boehringer Ingelheim and Eli Lilly and from several other companies. Dr. Claggett has been a consultant to Amgen, AO Biome, Biogen, Corvia, Myokardia, and Novartis.
FROM HFSA 2020
PPIs associated with diabetes risk, but questions remain
Regular use of proton pump inhibitors (PPIs) is associated with an increased risk of type 2 diabetes, according to a large prospective analysis of the Nurses’ Health Study. The results follow on other studies suggesting other potential adverse effects of PPIs such as dementia, kidney damage, and micronutrient deficiencies.
The authors, led by Jinqiu Yuan and Changhua Zhang of Sun Yat-sen University (Guangdong, China), call for regular blood glucose testing and diabetes screening for patients on long-term PPIs. But not all are convinced. “I think that’s a strong recommendation from the available data and it’s unclear how that would be put into practice. I think instead practitioners should adhere to best practices, which emphasize using the lowest effective dose of PPIs for patients with appropriate indications,” David Leiman, MD, MSHP, assistant professor of medicine at Duke University, Durham, N.C. said in an interview.
“Overall, the data from the study can be classified as provocative results that I think may warrant further study,” he added. Randomized, controlled trials or many more observational studies would be required to establish causality between PPI use and diabetes risk, and in any case the findings of the current study don’t warrant a change in practice, Dr. Leiman said, noting that the study’s design makes it likely that much or all of the observed associations were due to confounding.
The study appeared online Sept. 28 in Gut.
The researchers analyzed data from 80,500 women from the Nurses’ Health Study, 95,550 women from the Nurses’ Health Study II, and 28,639 men from the Health Professionals Follow-up Study (HPFS), with a median follow-up time of 12 years in NHS and NHS2 and 9.8 years in HPFS.
The absolute risk of diabetes was 7.44 per 1,000 person-years in PPI users versus 4.32 among nonusers. After adjustment for lagging PPI use for 2 years and stratification by age and study period, PPI use was associated with a 74% increased risk of diabetes (hazard ratio , 1.74; 95% confidence interval, 1.37-2.20). Multivariable adjustment for demographic factors, lifestyle habits, comorbidities, and use of other medications and clinical indications for PPI use attenuated the association but did not eliminate it (HR, 1.24; 95% CI, 1.17-1.31).
There was no statistically significant association in the HPFS group (HR, 1.12; 95% CI, 0.91-1.38), possibly because of the smaller sample size.
At 1 year, the number needed to harm with PPIs was 318.9 (95% CI, 285.2-385.0). At 2 years it was 170.8 (95% CI, 150.8-209.7) and at 3 years it was 77.3 (95% CI, 66.8-97.0).
At 0-2 years, PPI use was associated with a 5% increase in diabetes risk (HR, 1.05; 95% CI, 0.93-1.19). More than 2 years of use was associated with higher risk (HR, 1.26; 95% CI, 1.18-1.35).
There was also an association between stopping PPI use and a decreased risk of diabetes: Compared with current PPI users, those who had stopped within the past 2 years had a 17% reduction in risk (HR, 0.83; 95% CI, 0.70-0.98), and those who had stopped more than 2 years previously had a 19% reduction (HR, 0.81; 95% CI, 0.76-0.86).
The researchers also examined diabetes risk associated with use of H2 receptor agonists (H2RAs), since the drugs share clinical indications with PPIs. H2RA use was also associated with a higher risk of diabetes (adjusted HR, 1.14; 95% CI, 1.07-1.23).
The researchers suggested that the fact that the less potent H2RA inhibitors had a less pronounced association with diabetes risk supports the idea that acid suppression may be related to diabetes pathogenesis.
The authors also suggest that changes to the gut microbiota may underlie increased risk. PPI use has been shown to reduce gut microbiome diversity and alter its phenotype. Such changes could lead to weight gain, metabolic syndrome, and chronic liver disease, which could in turn heighten risk.
The study is limited by its observational nature, and lacked detailed information on dosage, frequency, and indications for PPI use.
SOURCE: Yuan J et al. Gut. 2020 Sep 28. doi: 10.1136/gutjnl-2020-322557.
Regular use of proton pump inhibitors (PPIs) is associated with an increased risk of type 2 diabetes, according to a large prospective analysis of the Nurses’ Health Study. The results follow on other studies suggesting other potential adverse effects of PPIs such as dementia, kidney damage, and micronutrient deficiencies.
The authors, led by Jinqiu Yuan and Changhua Zhang of Sun Yat-sen University (Guangdong, China), call for regular blood glucose testing and diabetes screening for patients on long-term PPIs. But not all are convinced. “I think that’s a strong recommendation from the available data and it’s unclear how that would be put into practice. I think instead practitioners should adhere to best practices, which emphasize using the lowest effective dose of PPIs for patients with appropriate indications,” David Leiman, MD, MSHP, assistant professor of medicine at Duke University, Durham, N.C. said in an interview.
“Overall, the data from the study can be classified as provocative results that I think may warrant further study,” he added. Randomized, controlled trials or many more observational studies would be required to establish causality between PPI use and diabetes risk, and in any case the findings of the current study don’t warrant a change in practice, Dr. Leiman said, noting that the study’s design makes it likely that much or all of the observed associations were due to confounding.
The study appeared online Sept. 28 in Gut.
The researchers analyzed data from 80,500 women from the Nurses’ Health Study, 95,550 women from the Nurses’ Health Study II, and 28,639 men from the Health Professionals Follow-up Study (HPFS), with a median follow-up time of 12 years in NHS and NHS2 and 9.8 years in HPFS.
The absolute risk of diabetes was 7.44 per 1,000 person-years in PPI users versus 4.32 among nonusers. After adjustment for lagging PPI use for 2 years and stratification by age and study period, PPI use was associated with a 74% increased risk of diabetes (hazard ratio , 1.74; 95% confidence interval, 1.37-2.20). Multivariable adjustment for demographic factors, lifestyle habits, comorbidities, and use of other medications and clinical indications for PPI use attenuated the association but did not eliminate it (HR, 1.24; 95% CI, 1.17-1.31).
There was no statistically significant association in the HPFS group (HR, 1.12; 95% CI, 0.91-1.38), possibly because of the smaller sample size.
At 1 year, the number needed to harm with PPIs was 318.9 (95% CI, 285.2-385.0). At 2 years it was 170.8 (95% CI, 150.8-209.7) and at 3 years it was 77.3 (95% CI, 66.8-97.0).
At 0-2 years, PPI use was associated with a 5% increase in diabetes risk (HR, 1.05; 95% CI, 0.93-1.19). More than 2 years of use was associated with higher risk (HR, 1.26; 95% CI, 1.18-1.35).
There was also an association between stopping PPI use and a decreased risk of diabetes: Compared with current PPI users, those who had stopped within the past 2 years had a 17% reduction in risk (HR, 0.83; 95% CI, 0.70-0.98), and those who had stopped more than 2 years previously had a 19% reduction (HR, 0.81; 95% CI, 0.76-0.86).
The researchers also examined diabetes risk associated with use of H2 receptor agonists (H2RAs), since the drugs share clinical indications with PPIs. H2RA use was also associated with a higher risk of diabetes (adjusted HR, 1.14; 95% CI, 1.07-1.23).
The researchers suggested that the fact that the less potent H2RA inhibitors had a less pronounced association with diabetes risk supports the idea that acid suppression may be related to diabetes pathogenesis.
The authors also suggest that changes to the gut microbiota may underlie increased risk. PPI use has been shown to reduce gut microbiome diversity and alter its phenotype. Such changes could lead to weight gain, metabolic syndrome, and chronic liver disease, which could in turn heighten risk.
The study is limited by its observational nature, and lacked detailed information on dosage, frequency, and indications for PPI use.
SOURCE: Yuan J et al. Gut. 2020 Sep 28. doi: 10.1136/gutjnl-2020-322557.
Regular use of proton pump inhibitors (PPIs) is associated with an increased risk of type 2 diabetes, according to a large prospective analysis of the Nurses’ Health Study. The results follow on other studies suggesting other potential adverse effects of PPIs such as dementia, kidney damage, and micronutrient deficiencies.
The authors, led by Jinqiu Yuan and Changhua Zhang of Sun Yat-sen University (Guangdong, China), call for regular blood glucose testing and diabetes screening for patients on long-term PPIs. But not all are convinced. “I think that’s a strong recommendation from the available data and it’s unclear how that would be put into practice. I think instead practitioners should adhere to best practices, which emphasize using the lowest effective dose of PPIs for patients with appropriate indications,” David Leiman, MD, MSHP, assistant professor of medicine at Duke University, Durham, N.C. said in an interview.
“Overall, the data from the study can be classified as provocative results that I think may warrant further study,” he added. Randomized, controlled trials or many more observational studies would be required to establish causality between PPI use and diabetes risk, and in any case the findings of the current study don’t warrant a change in practice, Dr. Leiman said, noting that the study’s design makes it likely that much or all of the observed associations were due to confounding.
The study appeared online Sept. 28 in Gut.
The researchers analyzed data from 80,500 women from the Nurses’ Health Study, 95,550 women from the Nurses’ Health Study II, and 28,639 men from the Health Professionals Follow-up Study (HPFS), with a median follow-up time of 12 years in NHS and NHS2 and 9.8 years in HPFS.
The absolute risk of diabetes was 7.44 per 1,000 person-years in PPI users versus 4.32 among nonusers. After adjustment for lagging PPI use for 2 years and stratification by age and study period, PPI use was associated with a 74% increased risk of diabetes (hazard ratio , 1.74; 95% confidence interval, 1.37-2.20). Multivariable adjustment for demographic factors, lifestyle habits, comorbidities, and use of other medications and clinical indications for PPI use attenuated the association but did not eliminate it (HR, 1.24; 95% CI, 1.17-1.31).
There was no statistically significant association in the HPFS group (HR, 1.12; 95% CI, 0.91-1.38), possibly because of the smaller sample size.
At 1 year, the number needed to harm with PPIs was 318.9 (95% CI, 285.2-385.0). At 2 years it was 170.8 (95% CI, 150.8-209.7) and at 3 years it was 77.3 (95% CI, 66.8-97.0).
At 0-2 years, PPI use was associated with a 5% increase in diabetes risk (HR, 1.05; 95% CI, 0.93-1.19). More than 2 years of use was associated with higher risk (HR, 1.26; 95% CI, 1.18-1.35).
There was also an association between stopping PPI use and a decreased risk of diabetes: Compared with current PPI users, those who had stopped within the past 2 years had a 17% reduction in risk (HR, 0.83; 95% CI, 0.70-0.98), and those who had stopped more than 2 years previously had a 19% reduction (HR, 0.81; 95% CI, 0.76-0.86).
The researchers also examined diabetes risk associated with use of H2 receptor agonists (H2RAs), since the drugs share clinical indications with PPIs. H2RA use was also associated with a higher risk of diabetes (adjusted HR, 1.14; 95% CI, 1.07-1.23).
The researchers suggested that the fact that the less potent H2RA inhibitors had a less pronounced association with diabetes risk supports the idea that acid suppression may be related to diabetes pathogenesis.
The authors also suggest that changes to the gut microbiota may underlie increased risk. PPI use has been shown to reduce gut microbiome diversity and alter its phenotype. Such changes could lead to weight gain, metabolic syndrome, and chronic liver disease, which could in turn heighten risk.
The study is limited by its observational nature, and lacked detailed information on dosage, frequency, and indications for PPI use.
SOURCE: Yuan J et al. Gut. 2020 Sep 28. doi: 10.1136/gutjnl-2020-322557.
FROM GUT
Study highlights differences between White and Latino patients with psoriasis
in the same studies, according to new data presented at the virtual Skin of Color Update 2020.
“Our findings demonstrate that, though White psoriasis patients may have higher severity in certain body regions such as the trunk, axilla, and groin areas, Latino psoriasis patients have a greater distribution of involvement, particularly in their upper limbs,” reported Alyssa G. Ashbaugh, a third-year medical student at the University of California, Irvine.
The study also found that psoriasis had a greater adverse impact on well-being, as measured with the Dermatology Life Quality Index (DLQI). At entry into the trials from which these patients were drawn, the higher DLQI score, significantly lower quality of life, was nearly two times higher (13.78 vs. 7.31; P = .01) among the Latino patients, compared with White patients.
This is not the first study to show a greater negative impact from psoriasis on Latinos than Whites, according to Ms. Ashbaugh. For example, Latinos had the worse quality of life at baseline by DLQI score than White, Asians, or Black participants in a trial of etanercept that enrolled more than 2000 patients.
In this retrospective chart review, patient characteristics were evaluated in all 21 Latino patients enrolled in psoriasis clinical trials at the University of California, Irvine, in a recent period. They were matched by age and gender to an equal number of White patients participating in the same trials.
The mean age at diagnosis of psoriasis was older in the Latino group than in the White population (42.4 vs. 35.6 years; P = .20), but the difference did not reach statistical significance. The proportion of patients with severe disease on investigator global assessment was also greater but not significantly different in the Latino group, compared with the White group, respectively (42.9% vs. 28.6%; P = .10).
However, differences in the patterns of disease did reach significance. This included a lower mean Psoriasis Assessment Severity Index score of the trunk, axilla, and groin in Latinos (4.74 vs. 9.73; P = .02). But compared with White participants, Latinos had a higher mean percentage of body surface area involvement in the upper limbs (4.78 vs. 1.85; P = .004) and a higher percentage of total body surface area involvement (20.50 vs. 10.03; P = .02).
“While White patients were found to have lived many more years with psoriasis, it is important for future studies to examine whether this is due to earlier onset or delayed diagnosis, given the fact that minorities are less likely to have access to a dermatologist,” reported Ms. Ashbaugh, who performed this work under the guidance of the senior author, Natasha Mesinkovska, MD, PhD, with the department of dermatology, University of California, Irvine.
Overall, the study suggested that body surface coverage and severity is not similarly distributed in Latinos relative to Whites. Although Ms. Ashbaugh conceded that the small sample size and retrospective design of this study are important limitations, she believes that her study, along with previously published studies that suggest psoriasis characteristics may differ meaningfully by race or ethnicity, raises issues that should be explored in future studies designed to confirm differences and whether those differences should affect management.
Other studies have suggested “there are notable differences in the presentation of psoriasis between racial and ethnic groups with the Latino population often presenting to physicians with more severe psoriasis and increased body surface area involvement,” Ms. Ashbaugh noted. Although this appears to be one of the first studies to examine psoriasis characteristics in Latinos relative to Whites, she believes this is an area ripe for further analysis.
Psoriasis “is not a rare occurrence” in non-White populations even if U.S. data suggest that the prevalence in “people of color is lower than that of psoriasis in the U.S. white population,” Amy McMichael, MD, chair of the department of dermatology, Wake Forest Baptist Medical Center, Winston-Salem, N.C., commented in an interview after the meeting. She agreed that it cannot be assumed that psoriasis in skin of color has the same manifestations or responds to treatment in the same way as in White patients.
“Studies have suggested that lesion thickness and, often, extent of disease can be worse in patients of color. Few studies to date have examined the efficacy of treatments and impact of disease in these populations,” she said.
One exception was a study Dr. McMichael and colleagues published last year on the efficacy and safety of the interleukin-17 receptor A antagonist brodalumab for psoriasis in patients of color. The study showed that Black, Latino, and Asian patients participating in the AMAGINE-2 and AMAGINE-3 trials achieved similar outcomes as White participants.
“We published this study because this is one of the first, if not the first, to have enough patients of color to actually draw conclusions about the efficacy of the biologic as well as the patient-reported outcomes,” she explained.
Like the author of the evaluation of Latino patients undertaken at the University of California, Irvine, Dr. McMichael said studies of psoriasis specific to patients of color are needed.
“We cannot assume all patients of color will have the same outcomes as their Caucasian counterparts. It is imperative to include those of color in future psoriasis treatment trials in order to determine the efficacy of new medications,” she added, specifically calling for collection of data on patient-reported outcomes.
Ms. Ashbaugh has no relevant financial relationships to disclose. Dr. McMichael’s disclosures included serving as an investigator and/or consultant for companies that included Allergan, Procter & Gamble, Johnson & Johnson, and Aclaris.
in the same studies, according to new data presented at the virtual Skin of Color Update 2020.
“Our findings demonstrate that, though White psoriasis patients may have higher severity in certain body regions such as the trunk, axilla, and groin areas, Latino psoriasis patients have a greater distribution of involvement, particularly in their upper limbs,” reported Alyssa G. Ashbaugh, a third-year medical student at the University of California, Irvine.
The study also found that psoriasis had a greater adverse impact on well-being, as measured with the Dermatology Life Quality Index (DLQI). At entry into the trials from which these patients were drawn, the higher DLQI score, significantly lower quality of life, was nearly two times higher (13.78 vs. 7.31; P = .01) among the Latino patients, compared with White patients.
This is not the first study to show a greater negative impact from psoriasis on Latinos than Whites, according to Ms. Ashbaugh. For example, Latinos had the worse quality of life at baseline by DLQI score than White, Asians, or Black participants in a trial of etanercept that enrolled more than 2000 patients.
In this retrospective chart review, patient characteristics were evaluated in all 21 Latino patients enrolled in psoriasis clinical trials at the University of California, Irvine, in a recent period. They were matched by age and gender to an equal number of White patients participating in the same trials.
The mean age at diagnosis of psoriasis was older in the Latino group than in the White population (42.4 vs. 35.6 years; P = .20), but the difference did not reach statistical significance. The proportion of patients with severe disease on investigator global assessment was also greater but not significantly different in the Latino group, compared with the White group, respectively (42.9% vs. 28.6%; P = .10).
However, differences in the patterns of disease did reach significance. This included a lower mean Psoriasis Assessment Severity Index score of the trunk, axilla, and groin in Latinos (4.74 vs. 9.73; P = .02). But compared with White participants, Latinos had a higher mean percentage of body surface area involvement in the upper limbs (4.78 vs. 1.85; P = .004) and a higher percentage of total body surface area involvement (20.50 vs. 10.03; P = .02).
“While White patients were found to have lived many more years with psoriasis, it is important for future studies to examine whether this is due to earlier onset or delayed diagnosis, given the fact that minorities are less likely to have access to a dermatologist,” reported Ms. Ashbaugh, who performed this work under the guidance of the senior author, Natasha Mesinkovska, MD, PhD, with the department of dermatology, University of California, Irvine.
Overall, the study suggested that body surface coverage and severity is not similarly distributed in Latinos relative to Whites. Although Ms. Ashbaugh conceded that the small sample size and retrospective design of this study are important limitations, she believes that her study, along with previously published studies that suggest psoriasis characteristics may differ meaningfully by race or ethnicity, raises issues that should be explored in future studies designed to confirm differences and whether those differences should affect management.
Other studies have suggested “there are notable differences in the presentation of psoriasis between racial and ethnic groups with the Latino population often presenting to physicians with more severe psoriasis and increased body surface area involvement,” Ms. Ashbaugh noted. Although this appears to be one of the first studies to examine psoriasis characteristics in Latinos relative to Whites, she believes this is an area ripe for further analysis.
Psoriasis “is not a rare occurrence” in non-White populations even if U.S. data suggest that the prevalence in “people of color is lower than that of psoriasis in the U.S. white population,” Amy McMichael, MD, chair of the department of dermatology, Wake Forest Baptist Medical Center, Winston-Salem, N.C., commented in an interview after the meeting. She agreed that it cannot be assumed that psoriasis in skin of color has the same manifestations or responds to treatment in the same way as in White patients.
“Studies have suggested that lesion thickness and, often, extent of disease can be worse in patients of color. Few studies to date have examined the efficacy of treatments and impact of disease in these populations,” she said.
One exception was a study Dr. McMichael and colleagues published last year on the efficacy and safety of the interleukin-17 receptor A antagonist brodalumab for psoriasis in patients of color. The study showed that Black, Latino, and Asian patients participating in the AMAGINE-2 and AMAGINE-3 trials achieved similar outcomes as White participants.
“We published this study because this is one of the first, if not the first, to have enough patients of color to actually draw conclusions about the efficacy of the biologic as well as the patient-reported outcomes,” she explained.
Like the author of the evaluation of Latino patients undertaken at the University of California, Irvine, Dr. McMichael said studies of psoriasis specific to patients of color are needed.
“We cannot assume all patients of color will have the same outcomes as their Caucasian counterparts. It is imperative to include those of color in future psoriasis treatment trials in order to determine the efficacy of new medications,” she added, specifically calling for collection of data on patient-reported outcomes.
Ms. Ashbaugh has no relevant financial relationships to disclose. Dr. McMichael’s disclosures included serving as an investigator and/or consultant for companies that included Allergan, Procter & Gamble, Johnson & Johnson, and Aclaris.
in the same studies, according to new data presented at the virtual Skin of Color Update 2020.
“Our findings demonstrate that, though White psoriasis patients may have higher severity in certain body regions such as the trunk, axilla, and groin areas, Latino psoriasis patients have a greater distribution of involvement, particularly in their upper limbs,” reported Alyssa G. Ashbaugh, a third-year medical student at the University of California, Irvine.
The study also found that psoriasis had a greater adverse impact on well-being, as measured with the Dermatology Life Quality Index (DLQI). At entry into the trials from which these patients were drawn, the higher DLQI score, significantly lower quality of life, was nearly two times higher (13.78 vs. 7.31; P = .01) among the Latino patients, compared with White patients.
This is not the first study to show a greater negative impact from psoriasis on Latinos than Whites, according to Ms. Ashbaugh. For example, Latinos had the worse quality of life at baseline by DLQI score than White, Asians, or Black participants in a trial of etanercept that enrolled more than 2000 patients.
In this retrospective chart review, patient characteristics were evaluated in all 21 Latino patients enrolled in psoriasis clinical trials at the University of California, Irvine, in a recent period. They were matched by age and gender to an equal number of White patients participating in the same trials.
The mean age at diagnosis of psoriasis was older in the Latino group than in the White population (42.4 vs. 35.6 years; P = .20), but the difference did not reach statistical significance. The proportion of patients with severe disease on investigator global assessment was also greater but not significantly different in the Latino group, compared with the White group, respectively (42.9% vs. 28.6%; P = .10).
However, differences in the patterns of disease did reach significance. This included a lower mean Psoriasis Assessment Severity Index score of the trunk, axilla, and groin in Latinos (4.74 vs. 9.73; P = .02). But compared with White participants, Latinos had a higher mean percentage of body surface area involvement in the upper limbs (4.78 vs. 1.85; P = .004) and a higher percentage of total body surface area involvement (20.50 vs. 10.03; P = .02).
“While White patients were found to have lived many more years with psoriasis, it is important for future studies to examine whether this is due to earlier onset or delayed diagnosis, given the fact that minorities are less likely to have access to a dermatologist,” reported Ms. Ashbaugh, who performed this work under the guidance of the senior author, Natasha Mesinkovska, MD, PhD, with the department of dermatology, University of California, Irvine.
Overall, the study suggested that body surface coverage and severity is not similarly distributed in Latinos relative to Whites. Although Ms. Ashbaugh conceded that the small sample size and retrospective design of this study are important limitations, she believes that her study, along with previously published studies that suggest psoriasis characteristics may differ meaningfully by race or ethnicity, raises issues that should be explored in future studies designed to confirm differences and whether those differences should affect management.
Other studies have suggested “there are notable differences in the presentation of psoriasis between racial and ethnic groups with the Latino population often presenting to physicians with more severe psoriasis and increased body surface area involvement,” Ms. Ashbaugh noted. Although this appears to be one of the first studies to examine psoriasis characteristics in Latinos relative to Whites, she believes this is an area ripe for further analysis.
Psoriasis “is not a rare occurrence” in non-White populations even if U.S. data suggest that the prevalence in “people of color is lower than that of psoriasis in the U.S. white population,” Amy McMichael, MD, chair of the department of dermatology, Wake Forest Baptist Medical Center, Winston-Salem, N.C., commented in an interview after the meeting. She agreed that it cannot be assumed that psoriasis in skin of color has the same manifestations or responds to treatment in the same way as in White patients.
“Studies have suggested that lesion thickness and, often, extent of disease can be worse in patients of color. Few studies to date have examined the efficacy of treatments and impact of disease in these populations,” she said.
One exception was a study Dr. McMichael and colleagues published last year on the efficacy and safety of the interleukin-17 receptor A antagonist brodalumab for psoriasis in patients of color. The study showed that Black, Latino, and Asian patients participating in the AMAGINE-2 and AMAGINE-3 trials achieved similar outcomes as White participants.
“We published this study because this is one of the first, if not the first, to have enough patients of color to actually draw conclusions about the efficacy of the biologic as well as the patient-reported outcomes,” she explained.
Like the author of the evaluation of Latino patients undertaken at the University of California, Irvine, Dr. McMichael said studies of psoriasis specific to patients of color are needed.
“We cannot assume all patients of color will have the same outcomes as their Caucasian counterparts. It is imperative to include those of color in future psoriasis treatment trials in order to determine the efficacy of new medications,” she added, specifically calling for collection of data on patient-reported outcomes.
Ms. Ashbaugh has no relevant financial relationships to disclose. Dr. McMichael’s disclosures included serving as an investigator and/or consultant for companies that included Allergan, Procter & Gamble, Johnson & Johnson, and Aclaris.
FROM SOC 2020
The Other Pandemic: Addiction
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
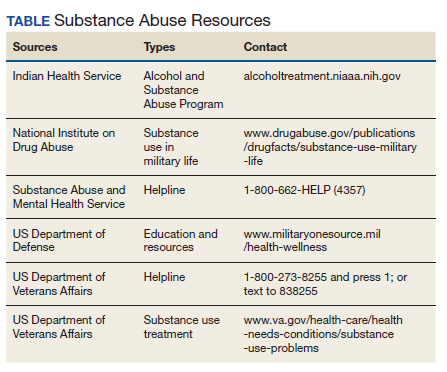
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417

HM20 Virtual: Key takeaways for the pediatric hospitalist
The HM20 Virtual conference in August was filled with excellent content that can be applied by all hospitalists. This article summarizes key concepts and takeaways for the pediatric hospitalist.
Racism and bias in medicine
HM20 Virtual session: Structural Racism and Bias in Hospital Medicine During Two Pandemics
Presenters: Nathan Chomilo, MD, FAAP, and Benji K. Mathews, MD, SFHM

Dr. Nathan Chomilo, of HealthPartners in Minneapolis, opened the session sharing how racial disparities were a symptom of racism. The presenters explained how structural racism has been propagated in medicine with the Hospital Survey and Construction Act of 1964 that allowed segregated hospitals, as well as the racism that exists within the “hidden curriculum.”
Dr. Chomilo discussed how personal experiences of racism can lead to worse health outcomes, including depression, obesity, and overall poor health. Dr. Mathews, also of HealthPartners, discussed how implicit biases can be addressed at the individual level, the organizational level, and simultaneously at both levels to create an antiracist culture. He presented strategies to mitigate individual biases; recognizing when biases may be triggered, checking biases at the door, connecting with others from different backgrounds as equals, and practicing antiracism by being an active bystander. Dr. Chomilo concluded the session by sharing that we can all grow by addressing racism at “our houses” (health care systems, medical schools, payer systems) with the goal to create an antiracist system.
Key takeaways
- Racial disparities are a symptom of structural racism that has been propagated in medicine for centuries.
- Addressing implicit biases at the individual level, organization level, and simultaneously at both levels can help leaders model and promote an antiracism culture.
HM20 Virtual session: When Grief and Crises Intersect: Perspectives of a Black Physician in the Time of Two Pandemics
Presenter: Kimberly Manning, MD, FACP, FAAP
Dr. Kimberly Manning, of Emory University in Atlanta, discussed the dual pandemics of COVID-19 and the racism that we are currently experiencing and tried to describe the unique perspective of Black Americans. Though it is easy to see that COVID-19 is a pandemic, racism is not always seen in this way. Dr. Manning demonstrated that, when a pandemic is defined as “that which occurs over a wide geographic area and affects a high proportion of the population,” racism is absolutely a pandemic. Black Americans have been disproportionately affected by COVID-19. Dr. Manning said we often hear that we are in unprecedented times but as far as racism is concerned, there is nothing new about this. She shared stories of personal milestones and how each of these instances, though marked by something beautiful, was also marked by something truly awful. Each time she had a reason to smile, there was something awful going on in the country that showed how racism was still present. Dr. Manning described that, though these were her stories, all Black Americans can recount the same stories, emotions, and feelings of grief.
Dr. Manning concluded by sharing how we can “Do The Work” to combat the pandemic of racism: broaden our funds of knowledge, remember that people are grieving, explore our implicit biases, be brave bystanders, and avoid performative allyship
Key takeaways
- Though the COVID19 pandemic is unprecedented, the pandemic of racism is not.
- We must “Do The Work” to combat everyday racism and to be cognizant of what our Black colleagues are going through every day.
Immigrant hospitalist challenges
HM20 Virtual session: The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19
Presenters: Manpreet S. Malik, MD, FHM, and Benji K. Mathews, MD, SFHM
Dr. Malik of Emory University in Atlanta, and Dr. Mathews of HealthPartners, opened this session by sharing their personal stories as immigrant physicians in the United States. Dr. Malik noted that physicians born outside the United States make up 29% of U.S. physicians, and 32% of hospitalists are international medical graduates.
The presenters revealed the structural hurdles immigrant physicians face, including lack of empowerment until achieving permanent residency status; limited leadership, administrative, and academic roles; concerns for job security and financial stability; and experiencing micro- and macroaggressions at work. The presenters shared a framework for a developmental orientation inclined toward cultural competency beginning with denial, followed by polarization, progressing to minimization, advancing to acceptance, and culminating in adaptation.
They concluded the session by stressing the importance of advocacy for immigrant physicians and encouraged colleagues to become engaged in efforts within their professional organizations.
Key takeaway
- Immigrant physicians experience structural challenges to their professional advancement because of their residency status.
Learner supervision
HM20 Virtual session: Call Me Maybe: Balancing Resident Autonomy With Sensible Supervision
Presenter: Daniel Steinberg, MD, SFHM, FACP

Dr. Steinberg, based at Mount Sinai in New York, explained that resident supervision is driven by three factors: what residents need, what residents want, and what the supervisor can provide. Although data is mixed as to whether supervision improves patient outcomes, supervision is essential for patient care and resident education. Dr. Steinberg showcased several relevant medical education studies related to supervision and focused on a key question: Do you trust the resident? The review of medical education literature discussed the meaning and development of trust, oral case presentations to determine trust, and the influence of supervisor experience.
Key takeaways
- Resident supervision is driven by what residents need, what residents want, and what the supervisor can provide.
- Trust can be determined from direct supervision, oral presentations, and remote access of electronic medical records, but is also influenced by attending experience and style.
Balancing personal and professional life
HM20 Virtual session: Being a Hospitalist and a Parent: Balancing Roles With Grace
Presenters: Heather E. Nye, MD, PhD, SFHM, and David Alfandre, MD, MSPH
Dr. Nye of the University of California, San Francisco, and Dr. Alfandre of New York University shared their challenges as hospitalists, parents, and partners before and during the COVID-19 pandemic. They described their feelings of guilt during the pandemic related to increasing their families’ infection risks, as well as the gratitude they felt for having stable jobs during the crisis. They shared solutions that worked for their families, including cooperating with their partners, expressing their scheduling needs, and negotiating to meet those needs with their employers.
Dr. Nye and Dr. Alfandre recommended staying connected with others for help, including partners, institutions, neighbors, and colleagues. They also recommended supporting, sharing, collaborating, and connecting with their partners and colleagues to maintain a balanced professional and personal life.
Key takeaway:
- Stay connected and support, collaborate, and share with your colleagues and partner at home.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s. Dr. Doraiswamy is an assistant professor of medicine and pediatrics and a med-peds hospitalist at The Ohio State University and Nationwide Children’s Hospital, both in Columbus. Dr. Tantoco is an academic med-peds hospitalist practicing in Northwestern Memorial Hospital, Chicago, and Ann & Robert H. Lurie Children’s Hospital of Chicago.
The HM20 Virtual conference in August was filled with excellent content that can be applied by all hospitalists. This article summarizes key concepts and takeaways for the pediatric hospitalist.
Racism and bias in medicine
HM20 Virtual session: Structural Racism and Bias in Hospital Medicine During Two Pandemics
Presenters: Nathan Chomilo, MD, FAAP, and Benji K. Mathews, MD, SFHM
Dr. Nathan Chomilo, of HealthPartners in Minneapolis, opened the session sharing how racial disparities were a symptom of racism. The presenters explained how structural racism has been propagated in medicine with the Hospital Survey and Construction Act of 1964 that allowed segregated hospitals, as well as the racism that exists within the “hidden curriculum.”
Dr. Chomilo discussed how personal experiences of racism can lead to worse health outcomes, including depression, obesity, and overall poor health. Dr. Mathews, also of HealthPartners, discussed how implicit biases can be addressed at the individual level, the organizational level, and simultaneously at both levels to create an antiracist culture. He presented strategies to mitigate individual biases; recognizing when biases may be triggered, checking biases at the door, connecting with others from different backgrounds as equals, and practicing antiracism by being an active bystander. Dr. Chomilo concluded the session by sharing that we can all grow by addressing racism at “our houses” (health care systems, medical schools, payer systems) with the goal to create an antiracist system.
Key takeaways
- Racial disparities are a symptom of structural racism that has been propagated in medicine for centuries.
- Addressing implicit biases at the individual level, organization level, and simultaneously at both levels can help leaders model and promote an antiracism culture.
HM20 Virtual session: When Grief and Crises Intersect: Perspectives of a Black Physician in the Time of Two Pandemics
Presenter: Kimberly Manning, MD, FACP, FAAP
Dr. Kimberly Manning, of Emory University in Atlanta, discussed the dual pandemics of COVID-19 and the racism that we are currently experiencing and tried to describe the unique perspective of Black Americans. Though it is easy to see that COVID-19 is a pandemic, racism is not always seen in this way. Dr. Manning demonstrated that, when a pandemic is defined as “that which occurs over a wide geographic area and affects a high proportion of the population,” racism is absolutely a pandemic. Black Americans have been disproportionately affected by COVID-19. Dr. Manning said we often hear that we are in unprecedented times but as far as racism is concerned, there is nothing new about this. She shared stories of personal milestones and how each of these instances, though marked by something beautiful, was also marked by something truly awful. Each time she had a reason to smile, there was something awful going on in the country that showed how racism was still present. Dr. Manning described that, though these were her stories, all Black Americans can recount the same stories, emotions, and feelings of grief.
Dr. Manning concluded by sharing how we can “Do The Work” to combat the pandemic of racism: broaden our funds of knowledge, remember that people are grieving, explore our implicit biases, be brave bystanders, and avoid performative allyship
Key takeaways
- Though the COVID19 pandemic is unprecedented, the pandemic of racism is not.
- We must “Do The Work” to combat everyday racism and to be cognizant of what our Black colleagues are going through every day.
Immigrant hospitalist challenges
HM20 Virtual session: The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19
Presenters: Manpreet S. Malik, MD, FHM, and Benji K. Mathews, MD, SFHM
Dr. Malik of Emory University in Atlanta, and Dr. Mathews of HealthPartners, opened this session by sharing their personal stories as immigrant physicians in the United States. Dr. Malik noted that physicians born outside the United States make up 29% of U.S. physicians, and 32% of hospitalists are international medical graduates.
The presenters revealed the structural hurdles immigrant physicians face, including lack of empowerment until achieving permanent residency status; limited leadership, administrative, and academic roles; concerns for job security and financial stability; and experiencing micro- and macroaggressions at work. The presenters shared a framework for a developmental orientation inclined toward cultural competency beginning with denial, followed by polarization, progressing to minimization, advancing to acceptance, and culminating in adaptation.
They concluded the session by stressing the importance of advocacy for immigrant physicians and encouraged colleagues to become engaged in efforts within their professional organizations.
Key takeaway
- Immigrant physicians experience structural challenges to their professional advancement because of their residency status.
Learner supervision
HM20 Virtual session: Call Me Maybe: Balancing Resident Autonomy With Sensible Supervision
Presenter: Daniel Steinberg, MD, SFHM, FACP
Dr. Steinberg, based at Mount Sinai in New York, explained that resident supervision is driven by three factors: what residents need, what residents want, and what the supervisor can provide. Although data is mixed as to whether supervision improves patient outcomes, supervision is essential for patient care and resident education. Dr. Steinberg showcased several relevant medical education studies related to supervision and focused on a key question: Do you trust the resident? The review of medical education literature discussed the meaning and development of trust, oral case presentations to determine trust, and the influence of supervisor experience.
Key takeaways
- Resident supervision is driven by what residents need, what residents want, and what the supervisor can provide.
- Trust can be determined from direct supervision, oral presentations, and remote access of electronic medical records, but is also influenced by attending experience and style.
Balancing personal and professional life
HM20 Virtual session: Being a Hospitalist and a Parent: Balancing Roles With Grace
Presenters: Heather E. Nye, MD, PhD, SFHM, and David Alfandre, MD, MSPH
Dr. Nye of the University of California, San Francisco, and Dr. Alfandre of New York University shared their challenges as hospitalists, parents, and partners before and during the COVID-19 pandemic. They described their feelings of guilt during the pandemic related to increasing their families’ infection risks, as well as the gratitude they felt for having stable jobs during the crisis. They shared solutions that worked for their families, including cooperating with their partners, expressing their scheduling needs, and negotiating to meet those needs with their employers.
Dr. Nye and Dr. Alfandre recommended staying connected with others for help, including partners, institutions, neighbors, and colleagues. They also recommended supporting, sharing, collaborating, and connecting with their partners and colleagues to maintain a balanced professional and personal life.
Key takeaway:
- Stay connected and support, collaborate, and share with your colleagues and partner at home.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s. Dr. Doraiswamy is an assistant professor of medicine and pediatrics and a med-peds hospitalist at The Ohio State University and Nationwide Children’s Hospital, both in Columbus. Dr. Tantoco is an academic med-peds hospitalist practicing in Northwestern Memorial Hospital, Chicago, and Ann & Robert H. Lurie Children’s Hospital of Chicago.
The HM20 Virtual conference in August was filled with excellent content that can be applied by all hospitalists. This article summarizes key concepts and takeaways for the pediatric hospitalist.
Racism and bias in medicine
HM20 Virtual session: Structural Racism and Bias in Hospital Medicine During Two Pandemics
Presenters: Nathan Chomilo, MD, FAAP, and Benji K. Mathews, MD, SFHM
Dr. Nathan Chomilo, of HealthPartners in Minneapolis, opened the session sharing how racial disparities were a symptom of racism. The presenters explained how structural racism has been propagated in medicine with the Hospital Survey and Construction Act of 1964 that allowed segregated hospitals, as well as the racism that exists within the “hidden curriculum.”
Dr. Chomilo discussed how personal experiences of racism can lead to worse health outcomes, including depression, obesity, and overall poor health. Dr. Mathews, also of HealthPartners, discussed how implicit biases can be addressed at the individual level, the organizational level, and simultaneously at both levels to create an antiracist culture. He presented strategies to mitigate individual biases; recognizing when biases may be triggered, checking biases at the door, connecting with others from different backgrounds as equals, and practicing antiracism by being an active bystander. Dr. Chomilo concluded the session by sharing that we can all grow by addressing racism at “our houses” (health care systems, medical schools, payer systems) with the goal to create an antiracist system.
Key takeaways
- Racial disparities are a symptom of structural racism that has been propagated in medicine for centuries.
- Addressing implicit biases at the individual level, organization level, and simultaneously at both levels can help leaders model and promote an antiracism culture.
HM20 Virtual session: When Grief and Crises Intersect: Perspectives of a Black Physician in the Time of Two Pandemics
Presenter: Kimberly Manning, MD, FACP, FAAP
Dr. Kimberly Manning, of Emory University in Atlanta, discussed the dual pandemics of COVID-19 and the racism that we are currently experiencing and tried to describe the unique perspective of Black Americans. Though it is easy to see that COVID-19 is a pandemic, racism is not always seen in this way. Dr. Manning demonstrated that, when a pandemic is defined as “that which occurs over a wide geographic area and affects a high proportion of the population,” racism is absolutely a pandemic. Black Americans have been disproportionately affected by COVID-19. Dr. Manning said we often hear that we are in unprecedented times but as far as racism is concerned, there is nothing new about this. She shared stories of personal milestones and how each of these instances, though marked by something beautiful, was also marked by something truly awful. Each time she had a reason to smile, there was something awful going on in the country that showed how racism was still present. Dr. Manning described that, though these were her stories, all Black Americans can recount the same stories, emotions, and feelings of grief.
Dr. Manning concluded by sharing how we can “Do The Work” to combat the pandemic of racism: broaden our funds of knowledge, remember that people are grieving, explore our implicit biases, be brave bystanders, and avoid performative allyship
Key takeaways
- Though the COVID19 pandemic is unprecedented, the pandemic of racism is not.
- We must “Do The Work” to combat everyday racism and to be cognizant of what our Black colleagues are going through every day.
Immigrant hospitalist challenges
HM20 Virtual session: The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19
Presenters: Manpreet S. Malik, MD, FHM, and Benji K. Mathews, MD, SFHM
Dr. Malik of Emory University in Atlanta, and Dr. Mathews of HealthPartners, opened this session by sharing their personal stories as immigrant physicians in the United States. Dr. Malik noted that physicians born outside the United States make up 29% of U.S. physicians, and 32% of hospitalists are international medical graduates.
The presenters revealed the structural hurdles immigrant physicians face, including lack of empowerment until achieving permanent residency status; limited leadership, administrative, and academic roles; concerns for job security and financial stability; and experiencing micro- and macroaggressions at work. The presenters shared a framework for a developmental orientation inclined toward cultural competency beginning with denial, followed by polarization, progressing to minimization, advancing to acceptance, and culminating in adaptation.
They concluded the session by stressing the importance of advocacy for immigrant physicians and encouraged colleagues to become engaged in efforts within their professional organizations.
Key takeaway
- Immigrant physicians experience structural challenges to their professional advancement because of their residency status.
Learner supervision
HM20 Virtual session: Call Me Maybe: Balancing Resident Autonomy With Sensible Supervision
Presenter: Daniel Steinberg, MD, SFHM, FACP
Dr. Steinberg, based at Mount Sinai in New York, explained that resident supervision is driven by three factors: what residents need, what residents want, and what the supervisor can provide. Although data is mixed as to whether supervision improves patient outcomes, supervision is essential for patient care and resident education. Dr. Steinberg showcased several relevant medical education studies related to supervision and focused on a key question: Do you trust the resident? The review of medical education literature discussed the meaning and development of trust, oral case presentations to determine trust, and the influence of supervisor experience.
Key takeaways
- Resident supervision is driven by what residents need, what residents want, and what the supervisor can provide.
- Trust can be determined from direct supervision, oral presentations, and remote access of electronic medical records, but is also influenced by attending experience and style.
Balancing personal and professional life
HM20 Virtual session: Being a Hospitalist and a Parent: Balancing Roles With Grace
Presenters: Heather E. Nye, MD, PhD, SFHM, and David Alfandre, MD, MSPH
Dr. Nye of the University of California, San Francisco, and Dr. Alfandre of New York University shared their challenges as hospitalists, parents, and partners before and during the COVID-19 pandemic. They described their feelings of guilt during the pandemic related to increasing their families’ infection risks, as well as the gratitude they felt for having stable jobs during the crisis. They shared solutions that worked for their families, including cooperating with their partners, expressing their scheduling needs, and negotiating to meet those needs with their employers.
Dr. Nye and Dr. Alfandre recommended staying connected with others for help, including partners, institutions, neighbors, and colleagues. They also recommended supporting, sharing, collaborating, and connecting with their partners and colleagues to maintain a balanced professional and personal life.
Key takeaway:
- Stay connected and support, collaborate, and share with your colleagues and partner at home.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s. Dr. Doraiswamy is an assistant professor of medicine and pediatrics and a med-peds hospitalist at The Ohio State University and Nationwide Children’s Hospital, both in Columbus. Dr. Tantoco is an academic med-peds hospitalist practicing in Northwestern Memorial Hospital, Chicago, and Ann & Robert H. Lurie Children’s Hospital of Chicago.
Erythematous Abdominal Nodule
The Diagnosis: Foreign Body Reaction With Sinus Tract
A delayed foreign body reaction is a rare complication of retained temporary pacing wires following cardiovascular surgery. These epicardial pacing wires are important for the management of postoperative arrhythmia and normally are removed by external traction after normal rhythm has been re-established. However, it is not uncommon for these wires to be cut at the skin surface in the setting of difficult removal, as retained pacing wires generally are viewed as benign.1 These reactions often take years after placement of the pacing wire to present themselves and most often resolve with either complete removal of the wire or resection of the distal end.2
Our patient was referred to dermatology and underwent a shave biopsy. Results were consistent with chronic inflammatory granulation tissue. Bacterial tissue culture grew Staphylococcus epidermidis. Cultures for acid-fast bacilli and fungi were negative. The patient was referred to cardiothoracic surgery. Computed tomography identified a retained temporary pacing wire extending to the base of the lesion. The lesion was excised and the distal aspect of the pacing wire was removed, which resulted in resolution of the nodule.
The differential diagnosis includes pyoderma gangrenosum, nodular basal cell carcinoma, Sister Mary Joseph nodule, and pyogenic granuloma. Pyoderma gangrenosum is a neutrophilic dermatosis that presents as a rapidly progressing, painful, necrotic ulcer. It is classically associated with inflammatory bowel disease and other systemic diseases but also can occur in isolation.3
Nodular basal cell carcinomas often develop in chronically sun-exposed areas of the body. Morphologically, they present as pink, pearl appearing papules with rolled borders and overlying arborizing telangiectasia. Nodular basal cell carcinomas may present with recurrent bleeding but typically do not have continuous drainage.4
Sister Mary Joseph nodule represents a periumbilical lymphatic metastasis from an underlying (usually intra-abdominal) malignancy. It typically presents as an umbilical or periumbilical nodule measuring 0.5 to 15 cm in diameter. The nodules often are painful and discharge a serous fluid. It is estimated that they are present in 1% to 3% of cases of abdominopelvic malignancy, but Sister Mary Joseph nodules also have been reported in several other types of solid organ tumors.5
Pyogenic granuloma is a benign vascular lesion that classically develops rapidly over the course of a few weeks. It often presents as a single red, moist, friable papule with a collarette of scale and frequently is associated with pain, bleeding, and ulceration. Keratinized skin or mucosa can be affected, and pyogenic granuloma is most common in children and young adults.6
- Chung DA, Smith EE. Delayed presentation of foreign body reaction secondary to retained pacing wires. Ann Thorac Surg. 1998;66:550-551.
- Gentry WH, Hassan AA. Complications of retained epicardial pacing wires (an unusual bronchial foreign body. Ann Thorac Surg. 1993;56:1391-1393.
- Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14:225-233.
- Tanese K. Diagnosis and treatment of basal cell carcinoma. Curr Treat Options Oncol. 2019;20:13
- Tso S, Brockley J, Recica H, et al. Sister Mary Joseph's nodule: an unusual but important physical finding characteristic of widespread internal malignancy. Br J Gen Pract. 2013;63:551-552.
- Mashiah J, Hadj-Rabia S, Slodownik D, et al. Effectiveness of topical propranolol 4% gel in the treatment of pyogenic granuloma in children. J Dermatol. 2019;46:245-248.
The Diagnosis: Foreign Body Reaction With Sinus Tract
A delayed foreign body reaction is a rare complication of retained temporary pacing wires following cardiovascular surgery. These epicardial pacing wires are important for the management of postoperative arrhythmia and normally are removed by external traction after normal rhythm has been re-established. However, it is not uncommon for these wires to be cut at the skin surface in the setting of difficult removal, as retained pacing wires generally are viewed as benign.1 These reactions often take years after placement of the pacing wire to present themselves and most often resolve with either complete removal of the wire or resection of the distal end.2
Our patient was referred to dermatology and underwent a shave biopsy. Results were consistent with chronic inflammatory granulation tissue. Bacterial tissue culture grew Staphylococcus epidermidis. Cultures for acid-fast bacilli and fungi were negative. The patient was referred to cardiothoracic surgery. Computed tomography identified a retained temporary pacing wire extending to the base of the lesion. The lesion was excised and the distal aspect of the pacing wire was removed, which resulted in resolution of the nodule.
The differential diagnosis includes pyoderma gangrenosum, nodular basal cell carcinoma, Sister Mary Joseph nodule, and pyogenic granuloma. Pyoderma gangrenosum is a neutrophilic dermatosis that presents as a rapidly progressing, painful, necrotic ulcer. It is classically associated with inflammatory bowel disease and other systemic diseases but also can occur in isolation.3
Nodular basal cell carcinomas often develop in chronically sun-exposed areas of the body. Morphologically, they present as pink, pearl appearing papules with rolled borders and overlying arborizing telangiectasia. Nodular basal cell carcinomas may present with recurrent bleeding but typically do not have continuous drainage.4
Sister Mary Joseph nodule represents a periumbilical lymphatic metastasis from an underlying (usually intra-abdominal) malignancy. It typically presents as an umbilical or periumbilical nodule measuring 0.5 to 15 cm in diameter. The nodules often are painful and discharge a serous fluid. It is estimated that they are present in 1% to 3% of cases of abdominopelvic malignancy, but Sister Mary Joseph nodules also have been reported in several other types of solid organ tumors.5
Pyogenic granuloma is a benign vascular lesion that classically develops rapidly over the course of a few weeks. It often presents as a single red, moist, friable papule with a collarette of scale and frequently is associated with pain, bleeding, and ulceration. Keratinized skin or mucosa can be affected, and pyogenic granuloma is most common in children and young adults.6
The Diagnosis: Foreign Body Reaction With Sinus Tract
A delayed foreign body reaction is a rare complication of retained temporary pacing wires following cardiovascular surgery. These epicardial pacing wires are important for the management of postoperative arrhythmia and normally are removed by external traction after normal rhythm has been re-established. However, it is not uncommon for these wires to be cut at the skin surface in the setting of difficult removal, as retained pacing wires generally are viewed as benign.1 These reactions often take years after placement of the pacing wire to present themselves and most often resolve with either complete removal of the wire or resection of the distal end.2
Our patient was referred to dermatology and underwent a shave biopsy. Results were consistent with chronic inflammatory granulation tissue. Bacterial tissue culture grew Staphylococcus epidermidis. Cultures for acid-fast bacilli and fungi were negative. The patient was referred to cardiothoracic surgery. Computed tomography identified a retained temporary pacing wire extending to the base of the lesion. The lesion was excised and the distal aspect of the pacing wire was removed, which resulted in resolution of the nodule.
The differential diagnosis includes pyoderma gangrenosum, nodular basal cell carcinoma, Sister Mary Joseph nodule, and pyogenic granuloma. Pyoderma gangrenosum is a neutrophilic dermatosis that presents as a rapidly progressing, painful, necrotic ulcer. It is classically associated with inflammatory bowel disease and other systemic diseases but also can occur in isolation.3
Nodular basal cell carcinomas often develop in chronically sun-exposed areas of the body. Morphologically, they present as pink, pearl appearing papules with rolled borders and overlying arborizing telangiectasia. Nodular basal cell carcinomas may present with recurrent bleeding but typically do not have continuous drainage.4
Sister Mary Joseph nodule represents a periumbilical lymphatic metastasis from an underlying (usually intra-abdominal) malignancy. It typically presents as an umbilical or periumbilical nodule measuring 0.5 to 15 cm in diameter. The nodules often are painful and discharge a serous fluid. It is estimated that they are present in 1% to 3% of cases of abdominopelvic malignancy, but Sister Mary Joseph nodules also have been reported in several other types of solid organ tumors.5
Pyogenic granuloma is a benign vascular lesion that classically develops rapidly over the course of a few weeks. It often presents as a single red, moist, friable papule with a collarette of scale and frequently is associated with pain, bleeding, and ulceration. Keratinized skin or mucosa can be affected, and pyogenic granuloma is most common in children and young adults.6
- Chung DA, Smith EE. Delayed presentation of foreign body reaction secondary to retained pacing wires. Ann Thorac Surg. 1998;66:550-551.
- Gentry WH, Hassan AA. Complications of retained epicardial pacing wires (an unusual bronchial foreign body. Ann Thorac Surg. 1993;56:1391-1393.
- Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14:225-233.
- Tanese K. Diagnosis and treatment of basal cell carcinoma. Curr Treat Options Oncol. 2019;20:13
- Tso S, Brockley J, Recica H, et al. Sister Mary Joseph's nodule: an unusual but important physical finding characteristic of widespread internal malignancy. Br J Gen Pract. 2013;63:551-552.
- Mashiah J, Hadj-Rabia S, Slodownik D, et al. Effectiveness of topical propranolol 4% gel in the treatment of pyogenic granuloma in children. J Dermatol. 2019;46:245-248.
- Chung DA, Smith EE. Delayed presentation of foreign body reaction secondary to retained pacing wires. Ann Thorac Surg. 1998;66:550-551.
- Gentry WH, Hassan AA. Complications of retained epicardial pacing wires (an unusual bronchial foreign body. Ann Thorac Surg. 1993;56:1391-1393.
- Ahn C, Negus D, Huang W. Pyoderma gangrenosum: a review of pathogenesis and treatment. Expert Rev Clin Immunol. 2018;14:225-233.
- Tanese K. Diagnosis and treatment of basal cell carcinoma. Curr Treat Options Oncol. 2019;20:13
- Tso S, Brockley J, Recica H, et al. Sister Mary Joseph's nodule: an unusual but important physical finding characteristic of widespread internal malignancy. Br J Gen Pract. 2013;63:551-552.
- Mashiah J, Hadj-Rabia S, Slodownik D, et al. Effectiveness of topical propranolol 4% gel in the treatment of pyogenic granuloma in children. J Dermatol. 2019;46:245-248.

A 71-year-old man presented with an inflamed erythematous papule on the right subcostal region of 12 months’ duration. It began as a small pimplelike bump that slowly enlarged. The patient did not report any pain or pruritus, but the lesion intermittently drained purulent fluid. The patient had a pacemaker and a history of severe aortic stenosis for which he underwent bioprosthetic aortic valve repair approximately 3 years prior to presentation. His postoperative course was complicated by sternal wound infection and sepsis, prompting surgical replacement of the graft and the pacemaker. He then developed aortitis secondary to bacterial endocarditis with multiple associated septic emboli and is now on lifelong levofloxacin and minocycline therapy. Physical examination revealed a 1.5-cm, erythematous, soft, protuberant nodule with surrounding skin dimpling on the right subcostal region adjacent to a well-healed surgical scar. Approximately 1 to 2 mL of purulent fluid was expressed.

Experts assess infection risks for patients on biologics
In a new review, a group of infectious disease experts have summarized and made recommendations about recent findings regarding infections that can occur during treatment with an evolving set of targeted and biologic therapies for rheumatoid arthritis and psoriatic arthritis.
“We claim for the need for multicenter registries and multidisciplinary approaches, for new vaccines trials in RA and PsA, and for better defining when and how biologics can be restarted after severe infections,” lead author Olivier Lortholary, MD, of the Institut Pasteur in Paris, and his coauthors wrote in Annals of the Rheumatic Diseases.

“The take-home message is that different DMARDs [disease-modifying antirheumatic drugs], in many ways, are very similar,” said coauthor Kevin L. Winthrop, MD, MPH, professor of public health and ophthalmology at Oregon Health & Science University, Portland, in an interview. “They all have fairly similar risks when it comes to ‘classical’ or routine bacterial infections. But when you talk about opportunistic infections, you start seeing the differences between these drugs.”
The experts began by addressing the current view of the infectious risk of biologic therapies, citing a recent meta-analysis in which standard (odds ratio, 1.31; 95% confidence interval, 1.09-1.58) and high (OR, 1.90; 95% CI, 1.50-2.39) doses of biologics were associated with increased risk of serious infection. They also noted that the ‘healthy drug survivor effect’ tends to confound long-term extensions of randomized clinical trials involving biologics.
“That is largely because people who are more likely to do well or have proven themselves to do well with that infection, they tend to stay in [trials] and stay on drugs,” Dr. Winthrop said. “The ones who develop infections are more likely to drop out. You see this survival of the fittest-type situation, where healthy users dominate a cohort over time. That’s why you see incidence rates decreasing.”
In response, Arthur Kavanaugh, MD, professor of medicine in the division of rheumatology, allergy, and immunology at the University of California, San Diego, and the director of the Center for Innovative Therapy there, backed the idea of a general ‘depletion of the susceptibles’ but warned doctors to evaluate each patient and situation accordingly. “Providers need to be vigilant throughout for common infections, rarer infections, and infections at greatest risk for the individual patient based on factors like comorbidities and concomitant medications,” he said in an interview.
When considering restarting a biologic in a patient who recently suffered a serious infection, the experts prescribed no general rule and noted that it will “depend on the type of infection, on the mechanism of action of the drug, on the other available drugs for the considered disease and, of course, on the willingness of the patients to restart a drug possibly having [given] him/her a side effect.”
Assessing infection risk related to various inhibitors
Regarding infections caused by TNF-alpha inhibitors (TNFIs), the experts acknowledged a broad increase in risk for mycobacterial and fungal infections, especially tuberculosis and histoplasmosis. They added that patients on TNFIs are more prone to developing pneumonia and soft tissue infections, while smaller studies have indicated a higher risk of listeriosis, legionellosis, herpes zoster (HZ), and reactivation of chronic hepatitis B virus infection.
As for recommendations, they endorsed discontinuing TNFIs when a serious infection occurs and not restarting until after treatment and clinical response. Patients should be screened for latent tuberculosis infection (LTBI) before starting the drug, and anti-TB drugs should be presented to patients with LTBI so they do not progress to active TB.
Regarding other biologics, they cited several studies indicating that IL-6 inhibitors can increase infection risks in RA patients at a rate similar to TNFIs. Among the most common infections were pneumonia and cellulitis. In addition, although PsA patients on IL-17 inhibitors have a dose-dependent risk of mild to moderate mucocutaneous candidiasis, there was no increased risk of serious opportunistic infections like TB.
In assessing JAK inhibitors, they cited a pooled analysis that indicated pneumonia and skin and soft-tissue infections as the most common and noted the high incidence of HZ, compared with other infections. They added that abatacept (Orencia) did not appear to increase risk of infections in RA patients, such as HZ, dermatomycosis, candidiasis, or endemic mycoses. Those same patients did not see an increased overall infection risk after treatment with rituximab (Rituxan), and clinical trials containing treatment with apremilast (Otezla) reported a rare occurrence of serious infections.
Recommendation-wise, they endorsed screening for LTBI before starting IL-6 inhibitors and antiviral prophylaxis with acyclovir in particularly at-risk patients on JAK inhibitors. Age-appropriate influenza vaccinations were also recommended for rituximab, because of the development of rituximab-induced hypogammaglobulinemia.
Prediction and prevention
When it comes to predicting infections in patients on biologics, the experts wrote that it “remains a challenge.” The potential effects of pretreatment underlying disease, the lack of validated biomarkers, and the relatively low rate of infections all combine to stymie prediction. That said, they acknowledged ongoing efforts in monitoring lymphocyte subpopulation counts and immunoglobin levels, as well as a clinical score called the RABBIT Risk Score for Infections, which was validated in two separate cohorts.

“As Yogi Berra said, predictions are hard, especially about the future,” Dr. Kavanaugh said. “Discussions with your patient are always important.”
In regard to overall prevention, they acknowledged that most of their recommendations are of low evidence, except for antiviral prophylaxis for hepatitis B patients on rituximab and the aforementioned LTBI therapy in patients on TNFIs. Broadly, they advocated for all RA and PsA patients to receive a full infectious disease evaluation before the start of targeted and biologic therapies.
They also addressed vaccinations, recommending an evaluation of the patient’s immunization history and potentially planning a catch-up schedule for those in need of the influenza vaccine, a diphtheria-tetanus-pertussis booster, or the pneumococcal vaccine. More broadly, they stated that “a better response is expected if [non-live] vaccination is performed before the introduction of immunosuppressive drugs.” They added that live vaccines should be administered as soon as possible.
What rheumatologists can do
“So how do you mitigate risk?” Dr. Winthrop asked. “You have to be able to predict the risk, see what’s modifiable, and try to act on it. A lot of the risk of infection has more to do with the patient than the therapy.
“You try to minimize what you’re doing to the patient, particularly around steroids,” he said. “And then you think about screening and vaccinations. Rheumatologists need to be involved in those conversations because they’re the ones who know how these drugs interact with vaccines. A lot of the drugs might dumb down vaccine responses. Be sure to consider that and give the vaccines at times that will optimize their immunogenicity and likely efficacy.”
“Thankfully, infections are not that common,” Dr. Kavanaugh said. “Rheumatologists depend on data from trials, but more safety data comes from registry data and personal and shared experience.”
The authors declared no potential conflicts of interest.
SOURCE: Lortholary O et al. Ann Rheum Dis. 2020 Sep 22. doi: 10.1136/annrheumdis-2020-217092.
In a new review, a group of infectious disease experts have summarized and made recommendations about recent findings regarding infections that can occur during treatment with an evolving set of targeted and biologic therapies for rheumatoid arthritis and psoriatic arthritis.
“We claim for the need for multicenter registries and multidisciplinary approaches, for new vaccines trials in RA and PsA, and for better defining when and how biologics can be restarted after severe infections,” lead author Olivier Lortholary, MD, of the Institut Pasteur in Paris, and his coauthors wrote in Annals of the Rheumatic Diseases.
“The take-home message is that different DMARDs [disease-modifying antirheumatic drugs], in many ways, are very similar,” said coauthor Kevin L. Winthrop, MD, MPH, professor of public health and ophthalmology at Oregon Health & Science University, Portland, in an interview. “They all have fairly similar risks when it comes to ‘classical’ or routine bacterial infections. But when you talk about opportunistic infections, you start seeing the differences between these drugs.”
The experts began by addressing the current view of the infectious risk of biologic therapies, citing a recent meta-analysis in which standard (odds ratio, 1.31; 95% confidence interval, 1.09-1.58) and high (OR, 1.90; 95% CI, 1.50-2.39) doses of biologics were associated with increased risk of serious infection. They also noted that the ‘healthy drug survivor effect’ tends to confound long-term extensions of randomized clinical trials involving biologics.
“That is largely because people who are more likely to do well or have proven themselves to do well with that infection, they tend to stay in [trials] and stay on drugs,” Dr. Winthrop said. “The ones who develop infections are more likely to drop out. You see this survival of the fittest-type situation, where healthy users dominate a cohort over time. That’s why you see incidence rates decreasing.”
In response, Arthur Kavanaugh, MD, professor of medicine in the division of rheumatology, allergy, and immunology at the University of California, San Diego, and the director of the Center for Innovative Therapy there, backed the idea of a general ‘depletion of the susceptibles’ but warned doctors to evaluate each patient and situation accordingly. “Providers need to be vigilant throughout for common infections, rarer infections, and infections at greatest risk for the individual patient based on factors like comorbidities and concomitant medications,” he said in an interview.
When considering restarting a biologic in a patient who recently suffered a serious infection, the experts prescribed no general rule and noted that it will “depend on the type of infection, on the mechanism of action of the drug, on the other available drugs for the considered disease and, of course, on the willingness of the patients to restart a drug possibly having [given] him/her a side effect.”
Assessing infection risk related to various inhibitors
Regarding infections caused by TNF-alpha inhibitors (TNFIs), the experts acknowledged a broad increase in risk for mycobacterial and fungal infections, especially tuberculosis and histoplasmosis. They added that patients on TNFIs are more prone to developing pneumonia and soft tissue infections, while smaller studies have indicated a higher risk of listeriosis, legionellosis, herpes zoster (HZ), and reactivation of chronic hepatitis B virus infection.
As for recommendations, they endorsed discontinuing TNFIs when a serious infection occurs and not restarting until after treatment and clinical response. Patients should be screened for latent tuberculosis infection (LTBI) before starting the drug, and anti-TB drugs should be presented to patients with LTBI so they do not progress to active TB.
Regarding other biologics, they cited several studies indicating that IL-6 inhibitors can increase infection risks in RA patients at a rate similar to TNFIs. Among the most common infections were pneumonia and cellulitis. In addition, although PsA patients on IL-17 inhibitors have a dose-dependent risk of mild to moderate mucocutaneous candidiasis, there was no increased risk of serious opportunistic infections like TB.
In assessing JAK inhibitors, they cited a pooled analysis that indicated pneumonia and skin and soft-tissue infections as the most common and noted the high incidence of HZ, compared with other infections. They added that abatacept (Orencia) did not appear to increase risk of infections in RA patients, such as HZ, dermatomycosis, candidiasis, or endemic mycoses. Those same patients did not see an increased overall infection risk after treatment with rituximab (Rituxan), and clinical trials containing treatment with apremilast (Otezla) reported a rare occurrence of serious infections.
Recommendation-wise, they endorsed screening for LTBI before starting IL-6 inhibitors and antiviral prophylaxis with acyclovir in particularly at-risk patients on JAK inhibitors. Age-appropriate influenza vaccinations were also recommended for rituximab, because of the development of rituximab-induced hypogammaglobulinemia.
Prediction and prevention
When it comes to predicting infections in patients on biologics, the experts wrote that it “remains a challenge.” The potential effects of pretreatment underlying disease, the lack of validated biomarkers, and the relatively low rate of infections all combine to stymie prediction. That said, they acknowledged ongoing efforts in monitoring lymphocyte subpopulation counts and immunoglobin levels, as well as a clinical score called the RABBIT Risk Score for Infections, which was validated in two separate cohorts.
“As Yogi Berra said, predictions are hard, especially about the future,” Dr. Kavanaugh said. “Discussions with your patient are always important.”
In regard to overall prevention, they acknowledged that most of their recommendations are of low evidence, except for antiviral prophylaxis for hepatitis B patients on rituximab and the aforementioned LTBI therapy in patients on TNFIs. Broadly, they advocated for all RA and PsA patients to receive a full infectious disease evaluation before the start of targeted and biologic therapies.
They also addressed vaccinations, recommending an evaluation of the patient’s immunization history and potentially planning a catch-up schedule for those in need of the influenza vaccine, a diphtheria-tetanus-pertussis booster, or the pneumococcal vaccine. More broadly, they stated that “a better response is expected if [non-live] vaccination is performed before the introduction of immunosuppressive drugs.” They added that live vaccines should be administered as soon as possible.
What rheumatologists can do
“So how do you mitigate risk?” Dr. Winthrop asked. “You have to be able to predict the risk, see what’s modifiable, and try to act on it. A lot of the risk of infection has more to do with the patient than the therapy.
“You try to minimize what you’re doing to the patient, particularly around steroids,” he said. “And then you think about screening and vaccinations. Rheumatologists need to be involved in those conversations because they’re the ones who know how these drugs interact with vaccines. A lot of the drugs might dumb down vaccine responses. Be sure to consider that and give the vaccines at times that will optimize their immunogenicity and likely efficacy.”
“Thankfully, infections are not that common,” Dr. Kavanaugh said. “Rheumatologists depend on data from trials, but more safety data comes from registry data and personal and shared experience.”
The authors declared no potential conflicts of interest.
SOURCE: Lortholary O et al. Ann Rheum Dis. 2020 Sep 22. doi: 10.1136/annrheumdis-2020-217092.
In a new review, a group of infectious disease experts have summarized and made recommendations about recent findings regarding infections that can occur during treatment with an evolving set of targeted and biologic therapies for rheumatoid arthritis and psoriatic arthritis.
“We claim for the need for multicenter registries and multidisciplinary approaches, for new vaccines trials in RA and PsA, and for better defining when and how biologics can be restarted after severe infections,” lead author Olivier Lortholary, MD, of the Institut Pasteur in Paris, and his coauthors wrote in Annals of the Rheumatic Diseases.
“The take-home message is that different DMARDs [disease-modifying antirheumatic drugs], in many ways, are very similar,” said coauthor Kevin L. Winthrop, MD, MPH, professor of public health and ophthalmology at Oregon Health & Science University, Portland, in an interview. “They all have fairly similar risks when it comes to ‘classical’ or routine bacterial infections. But when you talk about opportunistic infections, you start seeing the differences between these drugs.”
The experts began by addressing the current view of the infectious risk of biologic therapies, citing a recent meta-analysis in which standard (odds ratio, 1.31; 95% confidence interval, 1.09-1.58) and high (OR, 1.90; 95% CI, 1.50-2.39) doses of biologics were associated with increased risk of serious infection. They also noted that the ‘healthy drug survivor effect’ tends to confound long-term extensions of randomized clinical trials involving biologics.
“That is largely because people who are more likely to do well or have proven themselves to do well with that infection, they tend to stay in [trials] and stay on drugs,” Dr. Winthrop said. “The ones who develop infections are more likely to drop out. You see this survival of the fittest-type situation, where healthy users dominate a cohort over time. That’s why you see incidence rates decreasing.”
In response, Arthur Kavanaugh, MD, professor of medicine in the division of rheumatology, allergy, and immunology at the University of California, San Diego, and the director of the Center for Innovative Therapy there, backed the idea of a general ‘depletion of the susceptibles’ but warned doctors to evaluate each patient and situation accordingly. “Providers need to be vigilant throughout for common infections, rarer infections, and infections at greatest risk for the individual patient based on factors like comorbidities and concomitant medications,” he said in an interview.
When considering restarting a biologic in a patient who recently suffered a serious infection, the experts prescribed no general rule and noted that it will “depend on the type of infection, on the mechanism of action of the drug, on the other available drugs for the considered disease and, of course, on the willingness of the patients to restart a drug possibly having [given] him/her a side effect.”
Assessing infection risk related to various inhibitors
Regarding infections caused by TNF-alpha inhibitors (TNFIs), the experts acknowledged a broad increase in risk for mycobacterial and fungal infections, especially tuberculosis and histoplasmosis. They added that patients on TNFIs are more prone to developing pneumonia and soft tissue infections, while smaller studies have indicated a higher risk of listeriosis, legionellosis, herpes zoster (HZ), and reactivation of chronic hepatitis B virus infection.
As for recommendations, they endorsed discontinuing TNFIs when a serious infection occurs and not restarting until after treatment and clinical response. Patients should be screened for latent tuberculosis infection (LTBI) before starting the drug, and anti-TB drugs should be presented to patients with LTBI so they do not progress to active TB.
Regarding other biologics, they cited several studies indicating that IL-6 inhibitors can increase infection risks in RA patients at a rate similar to TNFIs. Among the most common infections were pneumonia and cellulitis. In addition, although PsA patients on IL-17 inhibitors have a dose-dependent risk of mild to moderate mucocutaneous candidiasis, there was no increased risk of serious opportunistic infections like TB.
In assessing JAK inhibitors, they cited a pooled analysis that indicated pneumonia and skin and soft-tissue infections as the most common and noted the high incidence of HZ, compared with other infections. They added that abatacept (Orencia) did not appear to increase risk of infections in RA patients, such as HZ, dermatomycosis, candidiasis, or endemic mycoses. Those same patients did not see an increased overall infection risk after treatment with rituximab (Rituxan), and clinical trials containing treatment with apremilast (Otezla) reported a rare occurrence of serious infections.
Recommendation-wise, they endorsed screening for LTBI before starting IL-6 inhibitors and antiviral prophylaxis with acyclovir in particularly at-risk patients on JAK inhibitors. Age-appropriate influenza vaccinations were also recommended for rituximab, because of the development of rituximab-induced hypogammaglobulinemia.
Prediction and prevention
When it comes to predicting infections in patients on biologics, the experts wrote that it “remains a challenge.” The potential effects of pretreatment underlying disease, the lack of validated biomarkers, and the relatively low rate of infections all combine to stymie prediction. That said, they acknowledged ongoing efforts in monitoring lymphocyte subpopulation counts and immunoglobin levels, as well as a clinical score called the RABBIT Risk Score for Infections, which was validated in two separate cohorts.
“As Yogi Berra said, predictions are hard, especially about the future,” Dr. Kavanaugh said. “Discussions with your patient are always important.”
In regard to overall prevention, they acknowledged that most of their recommendations are of low evidence, except for antiviral prophylaxis for hepatitis B patients on rituximab and the aforementioned LTBI therapy in patients on TNFIs. Broadly, they advocated for all RA and PsA patients to receive a full infectious disease evaluation before the start of targeted and biologic therapies.
They also addressed vaccinations, recommending an evaluation of the patient’s immunization history and potentially planning a catch-up schedule for those in need of the influenza vaccine, a diphtheria-tetanus-pertussis booster, or the pneumococcal vaccine. More broadly, they stated that “a better response is expected if [non-live] vaccination is performed before the introduction of immunosuppressive drugs.” They added that live vaccines should be administered as soon as possible.
What rheumatologists can do
“So how do you mitigate risk?” Dr. Winthrop asked. “You have to be able to predict the risk, see what’s modifiable, and try to act on it. A lot of the risk of infection has more to do with the patient than the therapy.
“You try to minimize what you’re doing to the patient, particularly around steroids,” he said. “And then you think about screening and vaccinations. Rheumatologists need to be involved in those conversations because they’re the ones who know how these drugs interact with vaccines. A lot of the drugs might dumb down vaccine responses. Be sure to consider that and give the vaccines at times that will optimize their immunogenicity and likely efficacy.”
“Thankfully, infections are not that common,” Dr. Kavanaugh said. “Rheumatologists depend on data from trials, but more safety data comes from registry data and personal and shared experience.”
The authors declared no potential conflicts of interest.
SOURCE: Lortholary O et al. Ann Rheum Dis. 2020 Sep 22. doi: 10.1136/annrheumdis-2020-217092.
FROM ANNALS OF THE RHEUMATIC DISEASES
COVID-19 risks are no higher in patients with multiple sclerosis
new U.S. data suggest. A separate study from the United Kingdom also found similar trends of rates of COVID-19 infection in patients with MS and the general population.
Both studies were presented Sept. 26 at a special session on multiple sclerosis and COVID-19 at a final “Encore” event as part of the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The U.S. data appear consistent with studies from several other countries, in that worse COVID-19 outcomes increase with age and higher disability levels, both of which would be expected from findings in the general population.
The U.S. data also show a clear effect of race in MS, with higher rates of adverse COVID-19 outcomes in Black patients, again in line with what is seen in the general population.
“I would say the results from our study and in general do not suggest that MS itself is associated with higher risks of severe COVID-19 outcomes, compared with the general population,” said Amber Salter, PhD.
Dr. Salter, who is assistant professor of biostatistics at Washington University, St. Louis, presented data from the COViMS North American registry, set up for health care providers to report persons with MS who are infected with COVID-19.
The COViMS registry so far has information on 858 patients with MS who have COVID-19 (80% verified by a positive test), as reported from 150 different health care providers in the United States and Canada. The average age was 48 years, with average disease duration of 13.6 years. MS clinical course was reported as relapsing remitting in 78%, secondary progressive in 15%, and primary progressive in 5%. Most patients (72%) were fully ambulatory, 16% could walk with assistance, and 12% were nonambulatory.
Severe COVID-19 outcomes were classified as mortality (which occurred in 5.7% of the cohort), mortality/ICU admission (13.6%) and mortality/ICU admission/hospitalization (30.2%).
Results were adjusted for many different covariates, including sex, age, smoking, MS clinical course (relapsing, progressive), disease duration, ambulation, individual comorbidities (cardiovascular disease, cerebrovascular disease, chronic kidney disease, chronic lung disease, diabetes, hypertension, morbid obesity), and disease-modifying therapy use.
In multivariable logistic regression analyses, older age, having chronic renal disease, and being nonambulatory were consistently associated with increased odds of poorer outcomes. Chronic kidney disease had the strongest association with mortality (odds ratio, 28.6; P < .001). Other factors associated with mortality included cardiovascular disease (OR, 4.35; P = .009); age (OR per 10 years, 1.91; P = .012), and male sex (OR, 2.60; P = .041).
Patients who were nonambulatory had a higher risk of mortality/ICU admission/hospitalization (OR, 3.32; P = .003). This endpoint was also increased in patients on anti-CD20 drugs, compared with other disease-modifying treatment (OR, 2.31; P = .002), consistent with results from at least two other studies.
Disease-modifying therapy in general was not associated with an increased risk of worse outcomes. “There was some concern at the outset about the effect of disease-modifying therapies on COVID-19 outcomes, but most studies have not found an increased risk of worse outcomes in patients on such drug treatments, with the possible exception of anti-CD20 drugs,” Dr. Salter said.
“Some disease-modifying therapies may actually be protective (particularly interferon) and studies are investigating whether they may have a role in the treatment of COVID-19,” she added.
“The factors in MS patients that we and others have found to be associated with worse COVID-19 outcomes may not be specific to MS. Older age is known to be a primary risk factor for worse COVID-19 outcomes in the general population, and increasing disability presumably tracks with worse general heath,” Dr. Salter commented.
“I would say the overall data are fairly reassuring for MS patents,” she concluded.
Black patients have higher risk
One worrying finding in the North American data, however, was the effect of race. “We found an independent effect of race for worse COVID-19 outcomes in MS patients,” Dr. Slater said.
Of the 858 patients in the COViMS registry, 65.7% were White and 26.1% were Black. Black individuals were more likely to be younger, never smokers, have shorter MS duration, a relapsing MS course, and have comorbidities, compared with White patients. A higher proportion of Black patients had hypertension (40.2% vs 19.5%) and morbid obesity (17% vs. 9.5%).
Results showed that mortality rates were not statistically different between White and Black patients, but Black race was associated with increased risk of mortality and/or ICU admission, compared with White patients (16.9% vs. 12.8%), and multivariate logistic regression analysis showed Black race was independently associated with mortality/ICU admission after adjustments for covariates (OR, 3.7; P = .002).
Black race was also associated with increased risk of mortality/ICU admission/hospital admission (35.8% vs. 30.2%), and after adjustment for covariates this was found to be an independent predictor (OR, 1.7; P = .04).
“This higher COVID-19 risk in Black individuals is also seen in the general population, so these results are not that surprising and it doesn’t appear to be an effect specific to MS patients,” Dr. Salter commented.
U.K. data on risk of contracting COVID-19
A U.K. study also suggested race to be an independent predictor in the risk of contracting COVID-19 in patients with MS.
The study of more than 5,000 patients with MS showed that those from a Black, Asian, and Minority Ethnic group were twice as likely to report having COVID-19 than those who were White.
The study, which was conducted during the U.K. lockdown, also found that the trend of COVID-19 infection in patients with MS is comparable with that of the U.K. general population.
Presenting the data, Afagh Garjani, MD, concluded: “During a period with strict physical distancing measures, patients with MS are not at an increased risk of contracting COVID-19.”
Dr. Garjani, a neurology clinical research fellow at the University of Nottingham, (England), explained that the COVID-19 pandemic has introduced uncertainties into the MS community, and the focus so far has been the severity of infection among people with MS who have COVID-19.
“This approach has left questions about the risk of contracting disease in people with MS unanswered, which has implications as society gradually returns to normal,” she said.
Dr. Garjani presented data from the United Kingdom MS Register (UKMSR), which has been collecting demographic and MS-related data since 2011 from patients with MS throughout the United Kingdom.
On March 17 – just before the lockdown in United Kingdom – existing participants of the UKMSR were asked to join the COVID-19 study. The study was also advertised through social media. In this ongoing study, people with MS answered a COVID-19–related survey at participation and a different follow-up survey every 2 weeks depending on whether they contracted COVID-19.
The COVID-19 study included 5,309 patients with MS. The mean age of the study population was 52.4 years, 76.1% were female, and 95.7% were White. Of the 5,309 patients, 535 (10%) reported a self-diagnosis of COVID-19. Because of limited availability of tests in the United Kingdom at the time, only 75 patents had a positive polymerase chain reaction result.
“To our knowledge, this is the largest community-based study of COVID-19 in patients with MS worldwide,” Dr. Garjani said. She presented results from the period March 23 to June 24, when the United Kingdom was in a period of lockdown with vulnerable groups encouraged to self-isolate completely.
In this MS cohort, 47% reported self-isolating at some point. Those at older age and higher Expanded Disability Status Scale (EDSS) score were more likely to have self-isolated.
The researchers did not find that patients with progressive MS or those on disease-modifying therapies in general isolated more, but patients on monoclonal antibody drugs and fingolimod were more likely to self-isolate versus those on other therapies. “This may be because there are concerns about infection with these drugs and patients on these therapies may be more concerned about contracting COVID-19,” Dr. Garjani suggested.
In terms of contracting COVID, the researchers found a reduced risk of COVID-19 (self-diagnosed) in patients with older age and higher EDSS. “This is not really surprising that these patients were more likely to self-isolate,” Dr. Garjani commented.
No association was seen between type of MS, disease duration, disease-modifying therapy in general, and risk of COVID-19. No individual drug treatment increased risk versus no therapy or versus self-injectables. But there was an increased risk of contracting the virus in patients whose race was Black, Asian, or Minority Ethnic (OR, 2.2), which is in line with findings from the general population.
“This study is unique – the denominator is all people with MS. We are looking primarily at the risk of contracting COVID-19. Other studies are focusing more on people with MS who have COVID and assessing risk of a severe COVID outcome. Our results are not contradicting the findings from those studies,” Dr. Garjani said.
The results were similar only when patients with a confirmed COVID-19 test were considered.
In terms of outcomes in those who reported COVID-19 infection, preliminary results have not shown any MS factors – such as EDSS, age, type of MS, drug therapy in general – to be associated with outcome.
“Since the COVID-19 outbreak started there has been concern among MS patients, especially among those on disease-modifying therapies, about whether they are at increased risk of infection and severe disease,” Dr. Garjani said.
“We found similar trends of rates of infection in MS patients and the general population, and no signal of increased risks in those with higher EDSS or progressive MS. The caveat is that this study was conducted in a period of lockdown, but we adjusted for self-isolating behavior in the multivariable regression analysis,” she noted.
Dr. Salter is a statistical editor for the American Heart Association journal Circulation: Cardiovascular Imaging. Dr. Garjani has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new U.S. data suggest. A separate study from the United Kingdom also found similar trends of rates of COVID-19 infection in patients with MS and the general population.
Both studies were presented Sept. 26 at a special session on multiple sclerosis and COVID-19 at a final “Encore” event as part of the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The U.S. data appear consistent with studies from several other countries, in that worse COVID-19 outcomes increase with age and higher disability levels, both of which would be expected from findings in the general population.
The U.S. data also show a clear effect of race in MS, with higher rates of adverse COVID-19 outcomes in Black patients, again in line with what is seen in the general population.
“I would say the results from our study and in general do not suggest that MS itself is associated with higher risks of severe COVID-19 outcomes, compared with the general population,” said Amber Salter, PhD.
Dr. Salter, who is assistant professor of biostatistics at Washington University, St. Louis, presented data from the COViMS North American registry, set up for health care providers to report persons with MS who are infected with COVID-19.
The COViMS registry so far has information on 858 patients with MS who have COVID-19 (80% verified by a positive test), as reported from 150 different health care providers in the United States and Canada. The average age was 48 years, with average disease duration of 13.6 years. MS clinical course was reported as relapsing remitting in 78%, secondary progressive in 15%, and primary progressive in 5%. Most patients (72%) were fully ambulatory, 16% could walk with assistance, and 12% were nonambulatory.
Severe COVID-19 outcomes were classified as mortality (which occurred in 5.7% of the cohort), mortality/ICU admission (13.6%) and mortality/ICU admission/hospitalization (30.2%).
Results were adjusted for many different covariates, including sex, age, smoking, MS clinical course (relapsing, progressive), disease duration, ambulation, individual comorbidities (cardiovascular disease, cerebrovascular disease, chronic kidney disease, chronic lung disease, diabetes, hypertension, morbid obesity), and disease-modifying therapy use.
In multivariable logistic regression analyses, older age, having chronic renal disease, and being nonambulatory were consistently associated with increased odds of poorer outcomes. Chronic kidney disease had the strongest association with mortality (odds ratio, 28.6; P < .001). Other factors associated with mortality included cardiovascular disease (OR, 4.35; P = .009); age (OR per 10 years, 1.91; P = .012), and male sex (OR, 2.60; P = .041).
Patients who were nonambulatory had a higher risk of mortality/ICU admission/hospitalization (OR, 3.32; P = .003). This endpoint was also increased in patients on anti-CD20 drugs, compared with other disease-modifying treatment (OR, 2.31; P = .002), consistent with results from at least two other studies.
Disease-modifying therapy in general was not associated with an increased risk of worse outcomes. “There was some concern at the outset about the effect of disease-modifying therapies on COVID-19 outcomes, but most studies have not found an increased risk of worse outcomes in patients on such drug treatments, with the possible exception of anti-CD20 drugs,” Dr. Salter said.
“Some disease-modifying therapies may actually be protective (particularly interferon) and studies are investigating whether they may have a role in the treatment of COVID-19,” she added.
“The factors in MS patients that we and others have found to be associated with worse COVID-19 outcomes may not be specific to MS. Older age is known to be a primary risk factor for worse COVID-19 outcomes in the general population, and increasing disability presumably tracks with worse general heath,” Dr. Salter commented.
“I would say the overall data are fairly reassuring for MS patents,” she concluded.
Black patients have higher risk
One worrying finding in the North American data, however, was the effect of race. “We found an independent effect of race for worse COVID-19 outcomes in MS patients,” Dr. Slater said.
Of the 858 patients in the COViMS registry, 65.7% were White and 26.1% were Black. Black individuals were more likely to be younger, never smokers, have shorter MS duration, a relapsing MS course, and have comorbidities, compared with White patients. A higher proportion of Black patients had hypertension (40.2% vs 19.5%) and morbid obesity (17% vs. 9.5%).
Results showed that mortality rates were not statistically different between White and Black patients, but Black race was associated with increased risk of mortality and/or ICU admission, compared with White patients (16.9% vs. 12.8%), and multivariate logistic regression analysis showed Black race was independently associated with mortality/ICU admission after adjustments for covariates (OR, 3.7; P = .002).
Black race was also associated with increased risk of mortality/ICU admission/hospital admission (35.8% vs. 30.2%), and after adjustment for covariates this was found to be an independent predictor (OR, 1.7; P = .04).
“This higher COVID-19 risk in Black individuals is also seen in the general population, so these results are not that surprising and it doesn’t appear to be an effect specific to MS patients,” Dr. Salter commented.
U.K. data on risk of contracting COVID-19
A U.K. study also suggested race to be an independent predictor in the risk of contracting COVID-19 in patients with MS.
The study of more than 5,000 patients with MS showed that those from a Black, Asian, and Minority Ethnic group were twice as likely to report having COVID-19 than those who were White.
The study, which was conducted during the U.K. lockdown, also found that the trend of COVID-19 infection in patients with MS is comparable with that of the U.K. general population.
Presenting the data, Afagh Garjani, MD, concluded: “During a period with strict physical distancing measures, patients with MS are not at an increased risk of contracting COVID-19.”
Dr. Garjani, a neurology clinical research fellow at the University of Nottingham, (England), explained that the COVID-19 pandemic has introduced uncertainties into the MS community, and the focus so far has been the severity of infection among people with MS who have COVID-19.
“This approach has left questions about the risk of contracting disease in people with MS unanswered, which has implications as society gradually returns to normal,” she said.
Dr. Garjani presented data from the United Kingdom MS Register (UKMSR), which has been collecting demographic and MS-related data since 2011 from patients with MS throughout the United Kingdom.
On March 17 – just before the lockdown in United Kingdom – existing participants of the UKMSR were asked to join the COVID-19 study. The study was also advertised through social media. In this ongoing study, people with MS answered a COVID-19–related survey at participation and a different follow-up survey every 2 weeks depending on whether they contracted COVID-19.
The COVID-19 study included 5,309 patients with MS. The mean age of the study population was 52.4 years, 76.1% were female, and 95.7% were White. Of the 5,309 patients, 535 (10%) reported a self-diagnosis of COVID-19. Because of limited availability of tests in the United Kingdom at the time, only 75 patents had a positive polymerase chain reaction result.
“To our knowledge, this is the largest community-based study of COVID-19 in patients with MS worldwide,” Dr. Garjani said. She presented results from the period March 23 to June 24, when the United Kingdom was in a period of lockdown with vulnerable groups encouraged to self-isolate completely.
In this MS cohort, 47% reported self-isolating at some point. Those at older age and higher Expanded Disability Status Scale (EDSS) score were more likely to have self-isolated.
The researchers did not find that patients with progressive MS or those on disease-modifying therapies in general isolated more, but patients on monoclonal antibody drugs and fingolimod were more likely to self-isolate versus those on other therapies. “This may be because there are concerns about infection with these drugs and patients on these therapies may be more concerned about contracting COVID-19,” Dr. Garjani suggested.
In terms of contracting COVID, the researchers found a reduced risk of COVID-19 (self-diagnosed) in patients with older age and higher EDSS. “This is not really surprising that these patients were more likely to self-isolate,” Dr. Garjani commented.
No association was seen between type of MS, disease duration, disease-modifying therapy in general, and risk of COVID-19. No individual drug treatment increased risk versus no therapy or versus self-injectables. But there was an increased risk of contracting the virus in patients whose race was Black, Asian, or Minority Ethnic (OR, 2.2), which is in line with findings from the general population.
“This study is unique – the denominator is all people with MS. We are looking primarily at the risk of contracting COVID-19. Other studies are focusing more on people with MS who have COVID and assessing risk of a severe COVID outcome. Our results are not contradicting the findings from those studies,” Dr. Garjani said.
The results were similar only when patients with a confirmed COVID-19 test were considered.
In terms of outcomes in those who reported COVID-19 infection, preliminary results have not shown any MS factors – such as EDSS, age, type of MS, drug therapy in general – to be associated with outcome.
“Since the COVID-19 outbreak started there has been concern among MS patients, especially among those on disease-modifying therapies, about whether they are at increased risk of infection and severe disease,” Dr. Garjani said.
“We found similar trends of rates of infection in MS patients and the general population, and no signal of increased risks in those with higher EDSS or progressive MS. The caveat is that this study was conducted in a period of lockdown, but we adjusted for self-isolating behavior in the multivariable regression analysis,” she noted.
Dr. Salter is a statistical editor for the American Heart Association journal Circulation: Cardiovascular Imaging. Dr. Garjani has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new U.S. data suggest. A separate study from the United Kingdom also found similar trends of rates of COVID-19 infection in patients with MS and the general population.
Both studies were presented Sept. 26 at a special session on multiple sclerosis and COVID-19 at a final “Encore” event as part of the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The U.S. data appear consistent with studies from several other countries, in that worse COVID-19 outcomes increase with age and higher disability levels, both of which would be expected from findings in the general population.
The U.S. data also show a clear effect of race in MS, with higher rates of adverse COVID-19 outcomes in Black patients, again in line with what is seen in the general population.
“I would say the results from our study and in general do not suggest that MS itself is associated with higher risks of severe COVID-19 outcomes, compared with the general population,” said Amber Salter, PhD.
Dr. Salter, who is assistant professor of biostatistics at Washington University, St. Louis, presented data from the COViMS North American registry, set up for health care providers to report persons with MS who are infected with COVID-19.
The COViMS registry so far has information on 858 patients with MS who have COVID-19 (80% verified by a positive test), as reported from 150 different health care providers in the United States and Canada. The average age was 48 years, with average disease duration of 13.6 years. MS clinical course was reported as relapsing remitting in 78%, secondary progressive in 15%, and primary progressive in 5%. Most patients (72%) were fully ambulatory, 16% could walk with assistance, and 12% were nonambulatory.
Severe COVID-19 outcomes were classified as mortality (which occurred in 5.7% of the cohort), mortality/ICU admission (13.6%) and mortality/ICU admission/hospitalization (30.2%).
Results were adjusted for many different covariates, including sex, age, smoking, MS clinical course (relapsing, progressive), disease duration, ambulation, individual comorbidities (cardiovascular disease, cerebrovascular disease, chronic kidney disease, chronic lung disease, diabetes, hypertension, morbid obesity), and disease-modifying therapy use.
In multivariable logistic regression analyses, older age, having chronic renal disease, and being nonambulatory were consistently associated with increased odds of poorer outcomes. Chronic kidney disease had the strongest association with mortality (odds ratio, 28.6; P < .001). Other factors associated with mortality included cardiovascular disease (OR, 4.35; P = .009); age (OR per 10 years, 1.91; P = .012), and male sex (OR, 2.60; P = .041).
Patients who were nonambulatory had a higher risk of mortality/ICU admission/hospitalization (OR, 3.32; P = .003). This endpoint was also increased in patients on anti-CD20 drugs, compared with other disease-modifying treatment (OR, 2.31; P = .002), consistent with results from at least two other studies.
Disease-modifying therapy in general was not associated with an increased risk of worse outcomes. “There was some concern at the outset about the effect of disease-modifying therapies on COVID-19 outcomes, but most studies have not found an increased risk of worse outcomes in patients on such drug treatments, with the possible exception of anti-CD20 drugs,” Dr. Salter said.
“Some disease-modifying therapies may actually be protective (particularly interferon) and studies are investigating whether they may have a role in the treatment of COVID-19,” she added.
“The factors in MS patients that we and others have found to be associated with worse COVID-19 outcomes may not be specific to MS. Older age is known to be a primary risk factor for worse COVID-19 outcomes in the general population, and increasing disability presumably tracks with worse general heath,” Dr. Salter commented.
“I would say the overall data are fairly reassuring for MS patents,” she concluded.
Black patients have higher risk
One worrying finding in the North American data, however, was the effect of race. “We found an independent effect of race for worse COVID-19 outcomes in MS patients,” Dr. Slater said.
Of the 858 patients in the COViMS registry, 65.7% were White and 26.1% were Black. Black individuals were more likely to be younger, never smokers, have shorter MS duration, a relapsing MS course, and have comorbidities, compared with White patients. A higher proportion of Black patients had hypertension (40.2% vs 19.5%) and morbid obesity (17% vs. 9.5%).
Results showed that mortality rates were not statistically different between White and Black patients, but Black race was associated with increased risk of mortality and/or ICU admission, compared with White patients (16.9% vs. 12.8%), and multivariate logistic regression analysis showed Black race was independently associated with mortality/ICU admission after adjustments for covariates (OR, 3.7; P = .002).
Black race was also associated with increased risk of mortality/ICU admission/hospital admission (35.8% vs. 30.2%), and after adjustment for covariates this was found to be an independent predictor (OR, 1.7; P = .04).
“This higher COVID-19 risk in Black individuals is also seen in the general population, so these results are not that surprising and it doesn’t appear to be an effect specific to MS patients,” Dr. Salter commented.
U.K. data on risk of contracting COVID-19
A U.K. study also suggested race to be an independent predictor in the risk of contracting COVID-19 in patients with MS.
The study of more than 5,000 patients with MS showed that those from a Black, Asian, and Minority Ethnic group were twice as likely to report having COVID-19 than those who were White.
The study, which was conducted during the U.K. lockdown, also found that the trend of COVID-19 infection in patients with MS is comparable with that of the U.K. general population.
Presenting the data, Afagh Garjani, MD, concluded: “During a period with strict physical distancing measures, patients with MS are not at an increased risk of contracting COVID-19.”
Dr. Garjani, a neurology clinical research fellow at the University of Nottingham, (England), explained that the COVID-19 pandemic has introduced uncertainties into the MS community, and the focus so far has been the severity of infection among people with MS who have COVID-19.
“This approach has left questions about the risk of contracting disease in people with MS unanswered, which has implications as society gradually returns to normal,” she said.
Dr. Garjani presented data from the United Kingdom MS Register (UKMSR), which has been collecting demographic and MS-related data since 2011 from patients with MS throughout the United Kingdom.
On March 17 – just before the lockdown in United Kingdom – existing participants of the UKMSR were asked to join the COVID-19 study. The study was also advertised through social media. In this ongoing study, people with MS answered a COVID-19–related survey at participation and a different follow-up survey every 2 weeks depending on whether they contracted COVID-19.
The COVID-19 study included 5,309 patients with MS. The mean age of the study population was 52.4 years, 76.1% were female, and 95.7% were White. Of the 5,309 patients, 535 (10%) reported a self-diagnosis of COVID-19. Because of limited availability of tests in the United Kingdom at the time, only 75 patents had a positive polymerase chain reaction result.
“To our knowledge, this is the largest community-based study of COVID-19 in patients with MS worldwide,” Dr. Garjani said. She presented results from the period March 23 to June 24, when the United Kingdom was in a period of lockdown with vulnerable groups encouraged to self-isolate completely.
In this MS cohort, 47% reported self-isolating at some point. Those at older age and higher Expanded Disability Status Scale (EDSS) score were more likely to have self-isolated.
The researchers did not find that patients with progressive MS or those on disease-modifying therapies in general isolated more, but patients on monoclonal antibody drugs and fingolimod were more likely to self-isolate versus those on other therapies. “This may be because there are concerns about infection with these drugs and patients on these therapies may be more concerned about contracting COVID-19,” Dr. Garjani suggested.
In terms of contracting COVID, the researchers found a reduced risk of COVID-19 (self-diagnosed) in patients with older age and higher EDSS. “This is not really surprising that these patients were more likely to self-isolate,” Dr. Garjani commented.
No association was seen between type of MS, disease duration, disease-modifying therapy in general, and risk of COVID-19. No individual drug treatment increased risk versus no therapy or versus self-injectables. But there was an increased risk of contracting the virus in patients whose race was Black, Asian, or Minority Ethnic (OR, 2.2), which is in line with findings from the general population.
“This study is unique – the denominator is all people with MS. We are looking primarily at the risk of contracting COVID-19. Other studies are focusing more on people with MS who have COVID and assessing risk of a severe COVID outcome. Our results are not contradicting the findings from those studies,” Dr. Garjani said.
The results were similar only when patients with a confirmed COVID-19 test were considered.
In terms of outcomes in those who reported COVID-19 infection, preliminary results have not shown any MS factors – such as EDSS, age, type of MS, drug therapy in general – to be associated with outcome.
“Since the COVID-19 outbreak started there has been concern among MS patients, especially among those on disease-modifying therapies, about whether they are at increased risk of infection and severe disease,” Dr. Garjani said.
“We found similar trends of rates of infection in MS patients and the general population, and no signal of increased risks in those with higher EDSS or progressive MS. The caveat is that this study was conducted in a period of lockdown, but we adjusted for self-isolating behavior in the multivariable regression analysis,” she noted.
Dr. Salter is a statistical editor for the American Heart Association journal Circulation: Cardiovascular Imaging. Dr. Garjani has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM MSVIRTUAL2020