User login
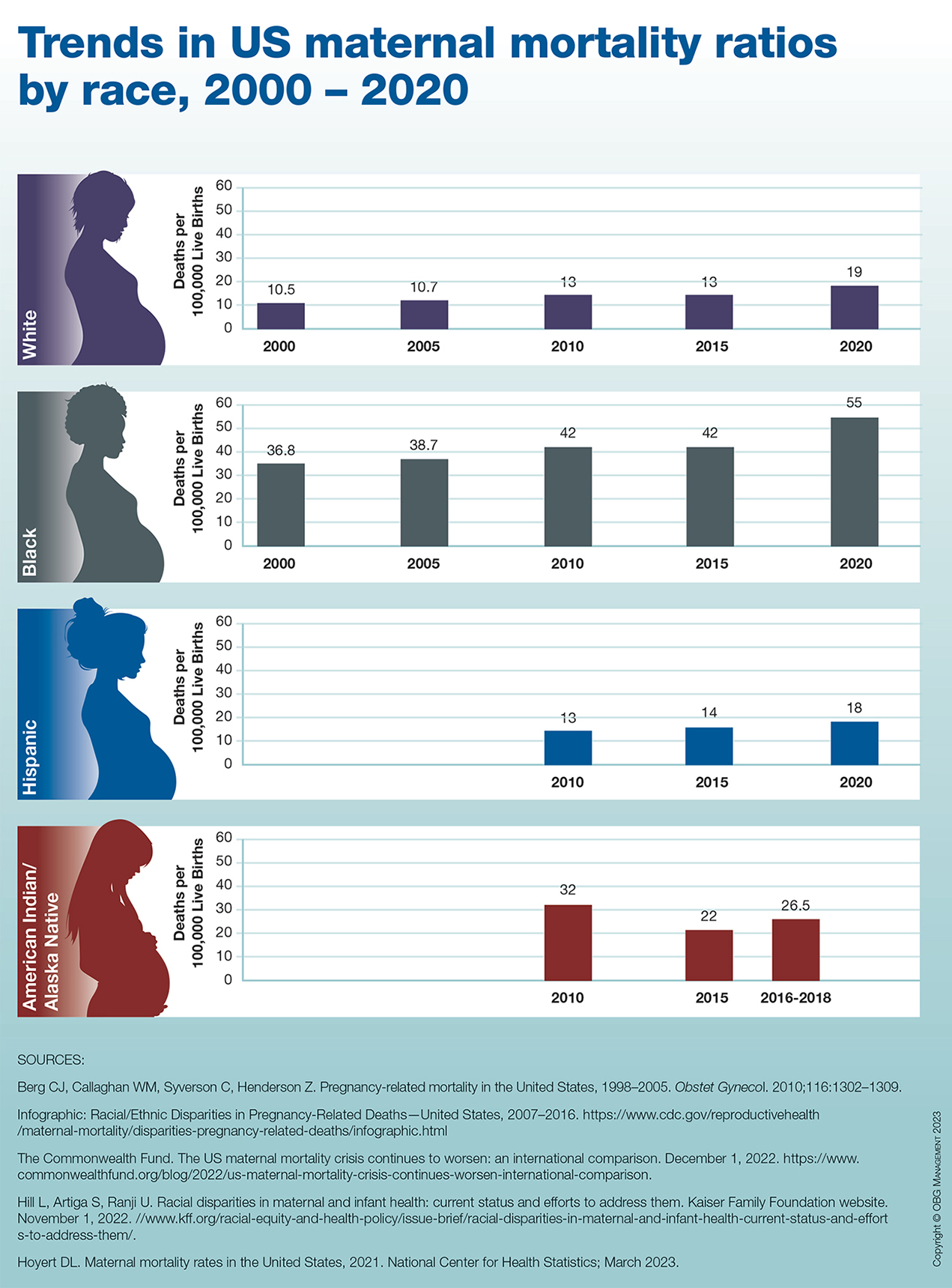
Trends in US maternal mortality ratios by race, 2000 – 2020
More support for thrombectomy in large-core strokes: TESLA, MAGNA
Although not quite meeting its primary endpoint,
And a new meta-analysis (MAGNA) of previous studies in a similar population has provided more detailed estimates of the treatment benefit of thrombectomy in these patients.
The TESLA trial, which included patients with large-core infarcts (ASPECTS score 2-5) within 24 hours of symptom onset, showed encouraging trends towards a benefit with thrombectomy for the primary outcome of 90-day utility-weighted scores on the modified Rankin scale (mRS), but this did not reach the prespecified Bayesian superiority threshold.
Several secondary efficacy endpoints also showed suggestions of benefits with thrombectomy.
“The interventional group had higher mean or average utility-weighted mRS scores than the control group which means that their functional recovery at 90 days was trending for better outcome and less disability,” lead TESLA investigator, Osama Zaidat, MD, neuroscience & stroke director at Mercy St. Vincent Medical Center, Toledo, Ohio, said in an interview. “They also showed better neurological improvement and a higher chance of achieving a good outcome (mRS 0-3).”
These patients with large-core infarct strokes were not included in the initial trials of endovascular therapy in patients presenting in the late time window, up to 24 hours, as it was thought they would not benefit. However, three recent trials (RESCUE-Japan LIMIT; ANGEL ASPECT; and SELECT 2) have shown that patients with large core infarcts can still benefit from endovascular thrombectomy.
While these three previous trials used sophisticated imaging techniques (MRI or CT perfusion) to select patients, and restricted patients included to those with an ASPECTS score of 3-5, the TESLA study had a more pragmatic design, using just noncontrast CT scan evaluation without advanced imaging to select patients, and extending the inclusion criteria to patients with an ASPECTS score of 2.
“Noncontrast CT scans are available at all stroke centers so this study is more practical, highly generalizable, and more applicable globally,” Dr. Zaidat commented.
“However, our results suggest that when using noncontrast CT only to select patients, the gain or treatment effect of thrombectomy seems to be smaller than when using sophisticated advanced imaging to make the decision to go for thrombectomy or not as in the other trials,” he added.
The TESLA trial results were presented at the recent European Stroke Organisation Conference, held in Munich.
The study included 300 stroke patients with anterior circulation large‐vessel occlusion (NIHSS of 6 or more) with a large‐core infarction (investigator read ASPECTS Score 2-5), selected on the basis of noncontrast CT scan, who were randomized to undergo intra-arterial thrombectomy or best medical management (control) up to 24 hours from last known well.
The trial had a Bayesian probabilities design, with a primary endpoint of the 90-day utility-weighted mRS (uw-mRS), a relatively new patient-centered outcome used in stroke trials, which includes a quality-of-life measurement. Utilities represent preferences for mRS health states and range from 0 (death) to 1 (perfect health), so in contrast to the traditional mRS scores, a higher uw-mRS score is better.
The 90-day uw-MRS scores were 2.93 in the thrombectomy group vs. 2.27 in the control group.
The Bayesian probability of thrombectomy superiority was 0.957, which Dr. Zaidat said was “similar” to a P value of .043, but this was less than the prespecified superiority probability of > .975 to declare efficacy.
A separate analysis in a population of patients selected by core-lab read noncontrast CT scan, showed a Bayesian probability of benefit with thrombectomy of 0.98, “similar” to one-sided P value of .02.
In terms of secondary endpoints, there were also some encouraging trends, including a suggestion of benefit in the 90-day mRS ordinal shift (odds ratio 1.40; P = .06).
The number of patients achieving functional independence (mRS 0-2) was 14% in the thrombectomy groups vs. 9% in the control group (P = .09); and a good functional outcome (mRS 0-3) was achieved in 30% of thrombectomy patients vs. 20% of those in the control group (P = .03).
Major neurological improvement (NIHSS scale of 0-2 or improvement of 8 points or more) occurred in 26% of thrombectomy patients vs. 13% of controls (P = .0008).
Quality of life, measured by the EuroQol 5-Dimension 5-Level survey, also showed a trend towards improvement in the thrombectomy group with mean scores of 53 vs. 46 (P = .058).
In terms of safety, all-cause mortality was similar in the two groups (35% thrombectomy and 33% control) and symptomatic intracerebral hemmorhage (ICH) occurred in 3.97% of thrombectomy vs. 1.34% of control patients (relative risk, 2.96).
“Cost-effective analysis and additional subgroup studies will provide more insight about the training needs to read the CT scan and if there is any value to treat patients with an ASPECTS score of 2,” Dr. Zaidat concluded.
“Larger pooled analysis will also be very useful in understanding the threshold of brain volume with irreversible damage beyond which thrombectomy wouldn’t be helpful,” he added.
Meta-analysis of previous studies: MAGNA
Another presentation at the ESOC meeting reported an individual patient data meta-analysis (MAGNA) of the three previous trials suggesting benefit of thrombectomy in patients with large-core ischemic strokes of the anterior circulation up to 24 hours of last known well.
The RESCUE Japan Limit trial was conducted in Japan; the SELECT-2 trial in North America, Europe, Australia, and New Zealand; and the ANGEL ASPECT trial in China.
In total, the meta-analysis included 1,009 patients, half of whom received thrombectomy and half received medical management only.
Results showed that in the whole population in the three trials, the use of thrombectomy improved functional outcomes, with an adjusted odds ratio of 1.78 (P < .001).
Functional independence (mRS 0-2) was also increased (23% vs. 9%; adjusted risk ratio, 2.62; P < .001); as was independent ambulation (mRS, 0-3; 41% vs. 24%; aRR, 1.76; P < .001).
But early neurological worsening was more frequent with thrombectomy (aRR 1.42, 1.09-1.84, P = .010).
No difference in mortality was identified between thrombectomy (27%) and medical management (28%) or in rates of symptomatic ICH (1.8% thrombectomy vs. 1.6% medical management).
“The results from the previously published large-core trials and from this pooled dataset provide unequivocal evidence on the efficacy and safety of endovascular thrombectomy in patients with large-core infarcts,” lead author of the MAGNA meta-analysis, Amrou Sarraj, MD, professor of neurology at University Hospitals Cleveland Medical Center, affiliate of Case Western Reserve University in Cleveland, concluded.
“The benefit persists across the spectrum of age, clinical severity, and time, with clear benefit up to an estimated ischemic core volume of 150 mL,” he added. “We have great hopes that these results will lead to more patients being treated and achieving improved functional outcomes.”
On how the TESLA results fit in with the previous three trials, Dr. Sarraj pointed out to this news organization that the TESLA trial was conducted in the United States and enrolled patients based on ASPECTS 2-5 on noncontrast CT.
“The primary outcome for intention-to-treat analysis did not reach the prespecified threshold for efficacy, but the results were largely in the same direction as shown in SELECT2, ANGEL ASPECT, and RESCUE Japan Limit,” he said. “These findings further emphasize the efficacy and safety of thrombectomy in patients with large ischemic core, at the same time reinforcing the need to provide results from pooled data from all large-core trials.”
He noted that results from two further trials of thrombectomy in large core strokes, TENSION and LASTE – both of which have now been stopped early because of the positive findings from the previous studies – are expected soon, and the MAGNA meta-analysis will be updated to include data from all six trials.
“This will increase the accuracy of the estimation of the treatment effect and will give even more power to look further into the details related to subgroups and selection imaging modalities,” Dr. Sarraj added.
The research team hopes that this joint effort will eventually set the pathway for selection algorithms and treatment boundaries in patients with large-vessel occlusion.
TESLA was an investigator-initiated study funded by unrestricted grants from Cerenovus, Penumbra, Medtronic, Stryker, and Genentech. Dr. Zaidat is a consultant for Stryker, Cerenovus, Penumbra, and Medtronic.
A version of this article first appeared on Medscape.com.
Although not quite meeting its primary endpoint,
And a new meta-analysis (MAGNA) of previous studies in a similar population has provided more detailed estimates of the treatment benefit of thrombectomy in these patients.
The TESLA trial, which included patients with large-core infarcts (ASPECTS score 2-5) within 24 hours of symptom onset, showed encouraging trends towards a benefit with thrombectomy for the primary outcome of 90-day utility-weighted scores on the modified Rankin scale (mRS), but this did not reach the prespecified Bayesian superiority threshold.
Several secondary efficacy endpoints also showed suggestions of benefits with thrombectomy.
“The interventional group had higher mean or average utility-weighted mRS scores than the control group which means that their functional recovery at 90 days was trending for better outcome and less disability,” lead TESLA investigator, Osama Zaidat, MD, neuroscience & stroke director at Mercy St. Vincent Medical Center, Toledo, Ohio, said in an interview. “They also showed better neurological improvement and a higher chance of achieving a good outcome (mRS 0-3).”
These patients with large-core infarct strokes were not included in the initial trials of endovascular therapy in patients presenting in the late time window, up to 24 hours, as it was thought they would not benefit. However, three recent trials (RESCUE-Japan LIMIT; ANGEL ASPECT; and SELECT 2) have shown that patients with large core infarcts can still benefit from endovascular thrombectomy.
While these three previous trials used sophisticated imaging techniques (MRI or CT perfusion) to select patients, and restricted patients included to those with an ASPECTS score of 3-5, the TESLA study had a more pragmatic design, using just noncontrast CT scan evaluation without advanced imaging to select patients, and extending the inclusion criteria to patients with an ASPECTS score of 2.
“Noncontrast CT scans are available at all stroke centers so this study is more practical, highly generalizable, and more applicable globally,” Dr. Zaidat commented.
“However, our results suggest that when using noncontrast CT only to select patients, the gain or treatment effect of thrombectomy seems to be smaller than when using sophisticated advanced imaging to make the decision to go for thrombectomy or not as in the other trials,” he added.
The TESLA trial results were presented at the recent European Stroke Organisation Conference, held in Munich.
The study included 300 stroke patients with anterior circulation large‐vessel occlusion (NIHSS of 6 or more) with a large‐core infarction (investigator read ASPECTS Score 2-5), selected on the basis of noncontrast CT scan, who were randomized to undergo intra-arterial thrombectomy or best medical management (control) up to 24 hours from last known well.
The trial had a Bayesian probabilities design, with a primary endpoint of the 90-day utility-weighted mRS (uw-mRS), a relatively new patient-centered outcome used in stroke trials, which includes a quality-of-life measurement. Utilities represent preferences for mRS health states and range from 0 (death) to 1 (perfect health), so in contrast to the traditional mRS scores, a higher uw-mRS score is better.
The 90-day uw-MRS scores were 2.93 in the thrombectomy group vs. 2.27 in the control group.
The Bayesian probability of thrombectomy superiority was 0.957, which Dr. Zaidat said was “similar” to a P value of .043, but this was less than the prespecified superiority probability of > .975 to declare efficacy.
A separate analysis in a population of patients selected by core-lab read noncontrast CT scan, showed a Bayesian probability of benefit with thrombectomy of 0.98, “similar” to one-sided P value of .02.
In terms of secondary endpoints, there were also some encouraging trends, including a suggestion of benefit in the 90-day mRS ordinal shift (odds ratio 1.40; P = .06).
The number of patients achieving functional independence (mRS 0-2) was 14% in the thrombectomy groups vs. 9% in the control group (P = .09); and a good functional outcome (mRS 0-3) was achieved in 30% of thrombectomy patients vs. 20% of those in the control group (P = .03).
Major neurological improvement (NIHSS scale of 0-2 or improvement of 8 points or more) occurred in 26% of thrombectomy patients vs. 13% of controls (P = .0008).
Quality of life, measured by the EuroQol 5-Dimension 5-Level survey, also showed a trend towards improvement in the thrombectomy group with mean scores of 53 vs. 46 (P = .058).
In terms of safety, all-cause mortality was similar in the two groups (35% thrombectomy and 33% control) and symptomatic intracerebral hemmorhage (ICH) occurred in 3.97% of thrombectomy vs. 1.34% of control patients (relative risk, 2.96).
“Cost-effective analysis and additional subgroup studies will provide more insight about the training needs to read the CT scan and if there is any value to treat patients with an ASPECTS score of 2,” Dr. Zaidat concluded.
“Larger pooled analysis will also be very useful in understanding the threshold of brain volume with irreversible damage beyond which thrombectomy wouldn’t be helpful,” he added.
Meta-analysis of previous studies: MAGNA
Another presentation at the ESOC meeting reported an individual patient data meta-analysis (MAGNA) of the three previous trials suggesting benefit of thrombectomy in patients with large-core ischemic strokes of the anterior circulation up to 24 hours of last known well.
The RESCUE Japan Limit trial was conducted in Japan; the SELECT-2 trial in North America, Europe, Australia, and New Zealand; and the ANGEL ASPECT trial in China.
In total, the meta-analysis included 1,009 patients, half of whom received thrombectomy and half received medical management only.
Results showed that in the whole population in the three trials, the use of thrombectomy improved functional outcomes, with an adjusted odds ratio of 1.78 (P < .001).
Functional independence (mRS 0-2) was also increased (23% vs. 9%; adjusted risk ratio, 2.62; P < .001); as was independent ambulation (mRS, 0-3; 41% vs. 24%; aRR, 1.76; P < .001).
But early neurological worsening was more frequent with thrombectomy (aRR 1.42, 1.09-1.84, P = .010).
No difference in mortality was identified between thrombectomy (27%) and medical management (28%) or in rates of symptomatic ICH (1.8% thrombectomy vs. 1.6% medical management).
“The results from the previously published large-core trials and from this pooled dataset provide unequivocal evidence on the efficacy and safety of endovascular thrombectomy in patients with large-core infarcts,” lead author of the MAGNA meta-analysis, Amrou Sarraj, MD, professor of neurology at University Hospitals Cleveland Medical Center, affiliate of Case Western Reserve University in Cleveland, concluded.
“The benefit persists across the spectrum of age, clinical severity, and time, with clear benefit up to an estimated ischemic core volume of 150 mL,” he added. “We have great hopes that these results will lead to more patients being treated and achieving improved functional outcomes.”
On how the TESLA results fit in with the previous three trials, Dr. Sarraj pointed out to this news organization that the TESLA trial was conducted in the United States and enrolled patients based on ASPECTS 2-5 on noncontrast CT.
“The primary outcome for intention-to-treat analysis did not reach the prespecified threshold for efficacy, but the results were largely in the same direction as shown in SELECT2, ANGEL ASPECT, and RESCUE Japan Limit,” he said. “These findings further emphasize the efficacy and safety of thrombectomy in patients with large ischemic core, at the same time reinforcing the need to provide results from pooled data from all large-core trials.”
He noted that results from two further trials of thrombectomy in large core strokes, TENSION and LASTE – both of which have now been stopped early because of the positive findings from the previous studies – are expected soon, and the MAGNA meta-analysis will be updated to include data from all six trials.
“This will increase the accuracy of the estimation of the treatment effect and will give even more power to look further into the details related to subgroups and selection imaging modalities,” Dr. Sarraj added.
The research team hopes that this joint effort will eventually set the pathway for selection algorithms and treatment boundaries in patients with large-vessel occlusion.
TESLA was an investigator-initiated study funded by unrestricted grants from Cerenovus, Penumbra, Medtronic, Stryker, and Genentech. Dr. Zaidat is a consultant for Stryker, Cerenovus, Penumbra, and Medtronic.
A version of this article first appeared on Medscape.com.
Although not quite meeting its primary endpoint,
And a new meta-analysis (MAGNA) of previous studies in a similar population has provided more detailed estimates of the treatment benefit of thrombectomy in these patients.
The TESLA trial, which included patients with large-core infarcts (ASPECTS score 2-5) within 24 hours of symptom onset, showed encouraging trends towards a benefit with thrombectomy for the primary outcome of 90-day utility-weighted scores on the modified Rankin scale (mRS), but this did not reach the prespecified Bayesian superiority threshold.
Several secondary efficacy endpoints also showed suggestions of benefits with thrombectomy.
“The interventional group had higher mean or average utility-weighted mRS scores than the control group which means that their functional recovery at 90 days was trending for better outcome and less disability,” lead TESLA investigator, Osama Zaidat, MD, neuroscience & stroke director at Mercy St. Vincent Medical Center, Toledo, Ohio, said in an interview. “They also showed better neurological improvement and a higher chance of achieving a good outcome (mRS 0-3).”
These patients with large-core infarct strokes were not included in the initial trials of endovascular therapy in patients presenting in the late time window, up to 24 hours, as it was thought they would not benefit. However, three recent trials (RESCUE-Japan LIMIT; ANGEL ASPECT; and SELECT 2) have shown that patients with large core infarcts can still benefit from endovascular thrombectomy.
While these three previous trials used sophisticated imaging techniques (MRI or CT perfusion) to select patients, and restricted patients included to those with an ASPECTS score of 3-5, the TESLA study had a more pragmatic design, using just noncontrast CT scan evaluation without advanced imaging to select patients, and extending the inclusion criteria to patients with an ASPECTS score of 2.
“Noncontrast CT scans are available at all stroke centers so this study is more practical, highly generalizable, and more applicable globally,” Dr. Zaidat commented.
“However, our results suggest that when using noncontrast CT only to select patients, the gain or treatment effect of thrombectomy seems to be smaller than when using sophisticated advanced imaging to make the decision to go for thrombectomy or not as in the other trials,” he added.
The TESLA trial results were presented at the recent European Stroke Organisation Conference, held in Munich.
The study included 300 stroke patients with anterior circulation large‐vessel occlusion (NIHSS of 6 or more) with a large‐core infarction (investigator read ASPECTS Score 2-5), selected on the basis of noncontrast CT scan, who were randomized to undergo intra-arterial thrombectomy or best medical management (control) up to 24 hours from last known well.
The trial had a Bayesian probabilities design, with a primary endpoint of the 90-day utility-weighted mRS (uw-mRS), a relatively new patient-centered outcome used in stroke trials, which includes a quality-of-life measurement. Utilities represent preferences for mRS health states and range from 0 (death) to 1 (perfect health), so in contrast to the traditional mRS scores, a higher uw-mRS score is better.
The 90-day uw-MRS scores were 2.93 in the thrombectomy group vs. 2.27 in the control group.
The Bayesian probability of thrombectomy superiority was 0.957, which Dr. Zaidat said was “similar” to a P value of .043, but this was less than the prespecified superiority probability of > .975 to declare efficacy.
A separate analysis in a population of patients selected by core-lab read noncontrast CT scan, showed a Bayesian probability of benefit with thrombectomy of 0.98, “similar” to one-sided P value of .02.
In terms of secondary endpoints, there were also some encouraging trends, including a suggestion of benefit in the 90-day mRS ordinal shift (odds ratio 1.40; P = .06).
The number of patients achieving functional independence (mRS 0-2) was 14% in the thrombectomy groups vs. 9% in the control group (P = .09); and a good functional outcome (mRS 0-3) was achieved in 30% of thrombectomy patients vs. 20% of those in the control group (P = .03).
Major neurological improvement (NIHSS scale of 0-2 or improvement of 8 points or more) occurred in 26% of thrombectomy patients vs. 13% of controls (P = .0008).
Quality of life, measured by the EuroQol 5-Dimension 5-Level survey, also showed a trend towards improvement in the thrombectomy group with mean scores of 53 vs. 46 (P = .058).
In terms of safety, all-cause mortality was similar in the two groups (35% thrombectomy and 33% control) and symptomatic intracerebral hemmorhage (ICH) occurred in 3.97% of thrombectomy vs. 1.34% of control patients (relative risk, 2.96).
“Cost-effective analysis and additional subgroup studies will provide more insight about the training needs to read the CT scan and if there is any value to treat patients with an ASPECTS score of 2,” Dr. Zaidat concluded.
“Larger pooled analysis will also be very useful in understanding the threshold of brain volume with irreversible damage beyond which thrombectomy wouldn’t be helpful,” he added.
Meta-analysis of previous studies: MAGNA
Another presentation at the ESOC meeting reported an individual patient data meta-analysis (MAGNA) of the three previous trials suggesting benefit of thrombectomy in patients with large-core ischemic strokes of the anterior circulation up to 24 hours of last known well.
The RESCUE Japan Limit trial was conducted in Japan; the SELECT-2 trial in North America, Europe, Australia, and New Zealand; and the ANGEL ASPECT trial in China.
In total, the meta-analysis included 1,009 patients, half of whom received thrombectomy and half received medical management only.
Results showed that in the whole population in the three trials, the use of thrombectomy improved functional outcomes, with an adjusted odds ratio of 1.78 (P < .001).
Functional independence (mRS 0-2) was also increased (23% vs. 9%; adjusted risk ratio, 2.62; P < .001); as was independent ambulation (mRS, 0-3; 41% vs. 24%; aRR, 1.76; P < .001).
But early neurological worsening was more frequent with thrombectomy (aRR 1.42, 1.09-1.84, P = .010).
No difference in mortality was identified between thrombectomy (27%) and medical management (28%) or in rates of symptomatic ICH (1.8% thrombectomy vs. 1.6% medical management).
“The results from the previously published large-core trials and from this pooled dataset provide unequivocal evidence on the efficacy and safety of endovascular thrombectomy in patients with large-core infarcts,” lead author of the MAGNA meta-analysis, Amrou Sarraj, MD, professor of neurology at University Hospitals Cleveland Medical Center, affiliate of Case Western Reserve University in Cleveland, concluded.
“The benefit persists across the spectrum of age, clinical severity, and time, with clear benefit up to an estimated ischemic core volume of 150 mL,” he added. “We have great hopes that these results will lead to more patients being treated and achieving improved functional outcomes.”
On how the TESLA results fit in with the previous three trials, Dr. Sarraj pointed out to this news organization that the TESLA trial was conducted in the United States and enrolled patients based on ASPECTS 2-5 on noncontrast CT.
“The primary outcome for intention-to-treat analysis did not reach the prespecified threshold for efficacy, but the results were largely in the same direction as shown in SELECT2, ANGEL ASPECT, and RESCUE Japan Limit,” he said. “These findings further emphasize the efficacy and safety of thrombectomy in patients with large ischemic core, at the same time reinforcing the need to provide results from pooled data from all large-core trials.”
He noted that results from two further trials of thrombectomy in large core strokes, TENSION and LASTE – both of which have now been stopped early because of the positive findings from the previous studies – are expected soon, and the MAGNA meta-analysis will be updated to include data from all six trials.
“This will increase the accuracy of the estimation of the treatment effect and will give even more power to look further into the details related to subgroups and selection imaging modalities,” Dr. Sarraj added.
The research team hopes that this joint effort will eventually set the pathway for selection algorithms and treatment boundaries in patients with large-vessel occlusion.
TESLA was an investigator-initiated study funded by unrestricted grants from Cerenovus, Penumbra, Medtronic, Stryker, and Genentech. Dr. Zaidat is a consultant for Stryker, Cerenovus, Penumbra, and Medtronic.
A version of this article first appeared on Medscape.com.
FROM ESOC 2023
Guide explains nonsurgical management of major hemorrhage
A new guide offers recommendations for the nonsurgical management of major hemorrhage, which is a challenging clinical problem.
Major hemorrhage is a significant cause of death and can occur in a myriad of clinical settings.
“In Ontario, we’ve been collecting quality metrics on major hemorrhages to try and make sure that a higher percentage of patients gets the best possible care when they are experiencing significant bleeding,” author Jeannie Callum, MD, professor and director of transfusion medicine at Kingston (Ont.) Health Sciences Centre and Queen’s University, also in Kingston, said in an interview. “There were some gaps, so this is our effort to get open, clear information out to the emergency doctors, intensive care unit doctors, the surgeons, and everyone else involved in managing major hemorrhage, to help close these gaps.”
The guide was published in the Canadian Medical Association Journal.
Fast care essential
The guide aims to provide answers, based on the latest research, to questions such as when to activate a massive hemorrhage protocol (MHP), which patients should receive tranexamic acid (TXA), which blood products should be transfused before laboratory results are available, how to monitor the effects of blood transfusion, and when fibrinogen concentrate or prothrombin complex concentrate should be given.
Not all recommendations will be followed, Dr. Callum said, especially in rural hospitals with limited resources. But the guide is adaptable, and rural hospitals can create protocols that are customized to their unique circumstances.
Care must be “perfect and fast” in the first hour of major injury, said Dr. Callum. “You need to get a proclotting drug in that first hour if you have a traumatic or postpartum bleed. You have to make sure your clotting factors never fail you throughout your resuscitation. You have to be fast with the transfusion. You have to monitor for the complications of the transfusion, electrolyte disturbances, and the patient’s temperature dropping. It’s a complicated situation that needs a multidisciplinary team.”
Bleeding affects everybody in medicine, from family doctors in smaller institutions who work in emergency departments to obstetricians and surgeons, she added.
“For people under the age of 45, trauma is the most common cause of death. When people die of trauma, they die of bleeding. So many people experience these extreme bleeds. We believe that some of them might be preventable with faster, more standardized, more aggressive care. That’s why we wrote this review,” said Dr. Callum.
Administer TXA quickly
The first recommendation is to ensure that every hospital has a massive hemorrhage protocol. Such a protocol is vital for the emergency department, operating room, and obstetric unit. “Making sure you’ve got a protocol that is updated every 3 years and adjusted to the local hospital context is essential,” said Dr. Callum.
Smaller hospitals will have to adjust their protocols according to the capabilities of their sites. “Some smaller hospitals do not have platelets in stock and get their platelets from another hospital, so you need to adjust your protocol to what you are able to do. Not every hospital can control bleeding in a trauma patient, so your protocol would be to stabilize and call a helicopter. Make sure all of this is detailed so that implementing it becomes automatic,” said Dr. Callum.
An MHP should be activated for patients with uncontrolled hemorrhage who meet the clinical criteria of the local hospital and are expected to need blood product support and red blood cells.
“Lots of people bleed, but not everybody is bleeding enough that they need a code transfusion,” said Dr. Callum. Most patients with gastrointestinal bleeds caused by NSAID use can be managed with uncrossed matched blood from the local blood bank. “But in patients who need the full code transfusion because they are going to need plasma, clotting factor replacement, and many other drugs, that is when the MHP should be activated. Don’t activate it when you don’t need it, because doing so activates the whole hospital and diverts care away from other patients.”
TXA should be administered as soon as possible after onset of hemorrhage in most patients, with the exception of gastrointestinal hemorrhage, where a benefit has not been shown.
TXA has been a major advance in treating massive bleeding, Dr. Callum said. “TXA was invented by a Japanese husband-and-wife research team. We know that it reduces the death rate in trauma and in postpartum hemorrhage, and it reduces the chance of major bleeding with major surgical procedures. We give it routinely in surgical procedures. If a patient gets TXA within 60 minutes of injury, it dramatically reduces the death rate. And it costs $10 per patient. It’s cheap, it’s easy, it has no side effects. It’s just amazing.”
Future research must address several unanswered questions, said Dr. Callum. These questions include whether prehospital transfusion improves patient outcomes, whether whole blood has a role in the early management of major hemorrhage, and what role factor concentrates play in patients with major bleeding.
‘Optimal recommendations’
Commenting on the document, Bourke Tillmann, MD, PhD, trauma team leader at Sunnybrook Health Sciences Centre and the Ross Tilley Burn Center in Toronto, said: “Overall, I think it is a good overview of MHPs as an approach to major hemorrhage.”
The review also is timely, since Ontario released its MHP guidelines in 2021, he added. “I would have liked to see more about the treatment aspects than just an overview of an MHP. But if you are the person overseeing the emergency department or running the blood bank, these protocols are incredibly useful and incredibly important.”
“This report is a nice and thoughtful overview of best practices in many areas, especially trauma, and makes recommendations that are optimal, although they are not necessarily practical in all centers,” Eric L. Legome, MD, professor and chair of emergency medicine at Mount Sinai West and Mount Sinai Morningside, New York, said in an interview.
“If you’re in a small rural hospital with one lab technician, trying to do all of these things, it will not be possible. These are optimal recommendations that people can use to the best of their ability, but they are not standard of care, because some places will not be able to provide this level of care,” he added. “This paper provides practical, reasonable advice that should be looked at as you are trying to implement transfusion policies and processes, with the understanding that it is not necessarily applicable or practical for very small hospitals in very rural centers that might not have access to these types of products and tools, but it’s a reasonable and nicely written paper.”
No outside funding for the guideline was reported. Dr. Callum has received research funding from Canadian Blood Services and Octapharma. She sits on the nominating committee with the Association for the Advancement of Blood & Biotherapies and on the data safety monitoring boards for the Tranexamic Acid for Subdural Hematoma trial and the Fibrinogen Replacement in Trauma trial. Dr. Tillmann and Dr. Legome reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A new guide offers recommendations for the nonsurgical management of major hemorrhage, which is a challenging clinical problem.
Major hemorrhage is a significant cause of death and can occur in a myriad of clinical settings.
“In Ontario, we’ve been collecting quality metrics on major hemorrhages to try and make sure that a higher percentage of patients gets the best possible care when they are experiencing significant bleeding,” author Jeannie Callum, MD, professor and director of transfusion medicine at Kingston (Ont.) Health Sciences Centre and Queen’s University, also in Kingston, said in an interview. “There were some gaps, so this is our effort to get open, clear information out to the emergency doctors, intensive care unit doctors, the surgeons, and everyone else involved in managing major hemorrhage, to help close these gaps.”
The guide was published in the Canadian Medical Association Journal.
Fast care essential
The guide aims to provide answers, based on the latest research, to questions such as when to activate a massive hemorrhage protocol (MHP), which patients should receive tranexamic acid (TXA), which blood products should be transfused before laboratory results are available, how to monitor the effects of blood transfusion, and when fibrinogen concentrate or prothrombin complex concentrate should be given.
Not all recommendations will be followed, Dr. Callum said, especially in rural hospitals with limited resources. But the guide is adaptable, and rural hospitals can create protocols that are customized to their unique circumstances.
Care must be “perfect and fast” in the first hour of major injury, said Dr. Callum. “You need to get a proclotting drug in that first hour if you have a traumatic or postpartum bleed. You have to make sure your clotting factors never fail you throughout your resuscitation. You have to be fast with the transfusion. You have to monitor for the complications of the transfusion, electrolyte disturbances, and the patient’s temperature dropping. It’s a complicated situation that needs a multidisciplinary team.”
Bleeding affects everybody in medicine, from family doctors in smaller institutions who work in emergency departments to obstetricians and surgeons, she added.
“For people under the age of 45, trauma is the most common cause of death. When people die of trauma, they die of bleeding. So many people experience these extreme bleeds. We believe that some of them might be preventable with faster, more standardized, more aggressive care. That’s why we wrote this review,” said Dr. Callum.
Administer TXA quickly
The first recommendation is to ensure that every hospital has a massive hemorrhage protocol. Such a protocol is vital for the emergency department, operating room, and obstetric unit. “Making sure you’ve got a protocol that is updated every 3 years and adjusted to the local hospital context is essential,” said Dr. Callum.
Smaller hospitals will have to adjust their protocols according to the capabilities of their sites. “Some smaller hospitals do not have platelets in stock and get their platelets from another hospital, so you need to adjust your protocol to what you are able to do. Not every hospital can control bleeding in a trauma patient, so your protocol would be to stabilize and call a helicopter. Make sure all of this is detailed so that implementing it becomes automatic,” said Dr. Callum.
An MHP should be activated for patients with uncontrolled hemorrhage who meet the clinical criteria of the local hospital and are expected to need blood product support and red blood cells.
“Lots of people bleed, but not everybody is bleeding enough that they need a code transfusion,” said Dr. Callum. Most patients with gastrointestinal bleeds caused by NSAID use can be managed with uncrossed matched blood from the local blood bank. “But in patients who need the full code transfusion because they are going to need plasma, clotting factor replacement, and many other drugs, that is when the MHP should be activated. Don’t activate it when you don’t need it, because doing so activates the whole hospital and diverts care away from other patients.”
TXA should be administered as soon as possible after onset of hemorrhage in most patients, with the exception of gastrointestinal hemorrhage, where a benefit has not been shown.
TXA has been a major advance in treating massive bleeding, Dr. Callum said. “TXA was invented by a Japanese husband-and-wife research team. We know that it reduces the death rate in trauma and in postpartum hemorrhage, and it reduces the chance of major bleeding with major surgical procedures. We give it routinely in surgical procedures. If a patient gets TXA within 60 minutes of injury, it dramatically reduces the death rate. And it costs $10 per patient. It’s cheap, it’s easy, it has no side effects. It’s just amazing.”
Future research must address several unanswered questions, said Dr. Callum. These questions include whether prehospital transfusion improves patient outcomes, whether whole blood has a role in the early management of major hemorrhage, and what role factor concentrates play in patients with major bleeding.
‘Optimal recommendations’
Commenting on the document, Bourke Tillmann, MD, PhD, trauma team leader at Sunnybrook Health Sciences Centre and the Ross Tilley Burn Center in Toronto, said: “Overall, I think it is a good overview of MHPs as an approach to major hemorrhage.”
The review also is timely, since Ontario released its MHP guidelines in 2021, he added. “I would have liked to see more about the treatment aspects than just an overview of an MHP. But if you are the person overseeing the emergency department or running the blood bank, these protocols are incredibly useful and incredibly important.”
“This report is a nice and thoughtful overview of best practices in many areas, especially trauma, and makes recommendations that are optimal, although they are not necessarily practical in all centers,” Eric L. Legome, MD, professor and chair of emergency medicine at Mount Sinai West and Mount Sinai Morningside, New York, said in an interview.
“If you’re in a small rural hospital with one lab technician, trying to do all of these things, it will not be possible. These are optimal recommendations that people can use to the best of their ability, but they are not standard of care, because some places will not be able to provide this level of care,” he added. “This paper provides practical, reasonable advice that should be looked at as you are trying to implement transfusion policies and processes, with the understanding that it is not necessarily applicable or practical for very small hospitals in very rural centers that might not have access to these types of products and tools, but it’s a reasonable and nicely written paper.”
No outside funding for the guideline was reported. Dr. Callum has received research funding from Canadian Blood Services and Octapharma. She sits on the nominating committee with the Association for the Advancement of Blood & Biotherapies and on the data safety monitoring boards for the Tranexamic Acid for Subdural Hematoma trial and the Fibrinogen Replacement in Trauma trial. Dr. Tillmann and Dr. Legome reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A new guide offers recommendations for the nonsurgical management of major hemorrhage, which is a challenging clinical problem.
Major hemorrhage is a significant cause of death and can occur in a myriad of clinical settings.
“In Ontario, we’ve been collecting quality metrics on major hemorrhages to try and make sure that a higher percentage of patients gets the best possible care when they are experiencing significant bleeding,” author Jeannie Callum, MD, professor and director of transfusion medicine at Kingston (Ont.) Health Sciences Centre and Queen’s University, also in Kingston, said in an interview. “There were some gaps, so this is our effort to get open, clear information out to the emergency doctors, intensive care unit doctors, the surgeons, and everyone else involved in managing major hemorrhage, to help close these gaps.”
The guide was published in the Canadian Medical Association Journal.
Fast care essential
The guide aims to provide answers, based on the latest research, to questions such as when to activate a massive hemorrhage protocol (MHP), which patients should receive tranexamic acid (TXA), which blood products should be transfused before laboratory results are available, how to monitor the effects of blood transfusion, and when fibrinogen concentrate or prothrombin complex concentrate should be given.
Not all recommendations will be followed, Dr. Callum said, especially in rural hospitals with limited resources. But the guide is adaptable, and rural hospitals can create protocols that are customized to their unique circumstances.
Care must be “perfect and fast” in the first hour of major injury, said Dr. Callum. “You need to get a proclotting drug in that first hour if you have a traumatic or postpartum bleed. You have to make sure your clotting factors never fail you throughout your resuscitation. You have to be fast with the transfusion. You have to monitor for the complications of the transfusion, electrolyte disturbances, and the patient’s temperature dropping. It’s a complicated situation that needs a multidisciplinary team.”
Bleeding affects everybody in medicine, from family doctors in smaller institutions who work in emergency departments to obstetricians and surgeons, she added.
“For people under the age of 45, trauma is the most common cause of death. When people die of trauma, they die of bleeding. So many people experience these extreme bleeds. We believe that some of them might be preventable with faster, more standardized, more aggressive care. That’s why we wrote this review,” said Dr. Callum.
Administer TXA quickly
The first recommendation is to ensure that every hospital has a massive hemorrhage protocol. Such a protocol is vital for the emergency department, operating room, and obstetric unit. “Making sure you’ve got a protocol that is updated every 3 years and adjusted to the local hospital context is essential,” said Dr. Callum.
Smaller hospitals will have to adjust their protocols according to the capabilities of their sites. “Some smaller hospitals do not have platelets in stock and get their platelets from another hospital, so you need to adjust your protocol to what you are able to do. Not every hospital can control bleeding in a trauma patient, so your protocol would be to stabilize and call a helicopter. Make sure all of this is detailed so that implementing it becomes automatic,” said Dr. Callum.
An MHP should be activated for patients with uncontrolled hemorrhage who meet the clinical criteria of the local hospital and are expected to need blood product support and red blood cells.
“Lots of people bleed, but not everybody is bleeding enough that they need a code transfusion,” said Dr. Callum. Most patients with gastrointestinal bleeds caused by NSAID use can be managed with uncrossed matched blood from the local blood bank. “But in patients who need the full code transfusion because they are going to need plasma, clotting factor replacement, and many other drugs, that is when the MHP should be activated. Don’t activate it when you don’t need it, because doing so activates the whole hospital and diverts care away from other patients.”
TXA should be administered as soon as possible after onset of hemorrhage in most patients, with the exception of gastrointestinal hemorrhage, where a benefit has not been shown.
TXA has been a major advance in treating massive bleeding, Dr. Callum said. “TXA was invented by a Japanese husband-and-wife research team. We know that it reduces the death rate in trauma and in postpartum hemorrhage, and it reduces the chance of major bleeding with major surgical procedures. We give it routinely in surgical procedures. If a patient gets TXA within 60 minutes of injury, it dramatically reduces the death rate. And it costs $10 per patient. It’s cheap, it’s easy, it has no side effects. It’s just amazing.”
Future research must address several unanswered questions, said Dr. Callum. These questions include whether prehospital transfusion improves patient outcomes, whether whole blood has a role in the early management of major hemorrhage, and what role factor concentrates play in patients with major bleeding.
‘Optimal recommendations’
Commenting on the document, Bourke Tillmann, MD, PhD, trauma team leader at Sunnybrook Health Sciences Centre and the Ross Tilley Burn Center in Toronto, said: “Overall, I think it is a good overview of MHPs as an approach to major hemorrhage.”
The review also is timely, since Ontario released its MHP guidelines in 2021, he added. “I would have liked to see more about the treatment aspects than just an overview of an MHP. But if you are the person overseeing the emergency department or running the blood bank, these protocols are incredibly useful and incredibly important.”
“This report is a nice and thoughtful overview of best practices in many areas, especially trauma, and makes recommendations that are optimal, although they are not necessarily practical in all centers,” Eric L. Legome, MD, professor and chair of emergency medicine at Mount Sinai West and Mount Sinai Morningside, New York, said in an interview.
“If you’re in a small rural hospital with one lab technician, trying to do all of these things, it will not be possible. These are optimal recommendations that people can use to the best of their ability, but they are not standard of care, because some places will not be able to provide this level of care,” he added. “This paper provides practical, reasonable advice that should be looked at as you are trying to implement transfusion policies and processes, with the understanding that it is not necessarily applicable or practical for very small hospitals in very rural centers that might not have access to these types of products and tools, but it’s a reasonable and nicely written paper.”
No outside funding for the guideline was reported. Dr. Callum has received research funding from Canadian Blood Services and Octapharma. She sits on the nominating committee with the Association for the Advancement of Blood & Biotherapies and on the data safety monitoring boards for the Tranexamic Acid for Subdural Hematoma trial and the Fibrinogen Replacement in Trauma trial. Dr. Tillmann and Dr. Legome reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
B vitamin may help boost antidepressant efficacy
The investigators analyzed six studies and found support for adjunctive use of LMF with patients with MDD not responding to antidepressant monotherapy. Treatment response was highest in those with obesity and inflammatory biomarkers.

“If clinicians try LMF on their patients with treatment-resistant depression, the treatment is very robust in patients who have high BMI [body mass index] or inflammatory biomarkers, and it’s worth a try even in patients who don’t have these indicators, since it’s safe and well tolerated, with no downside,” study investigator Vladimir Maletic, MD, MS, clinical professor of psychiatry and behavioral science, University of South Carolina, Greenville, said in an interview.
The study was published online in the Journal of Clinical Psychiatry.
‘Shortcut’ to the brain
A considerable percentage of patients with MDD fail to achieve an adequate response to treatment, the authors wrote.
Previous research shows benefits of folate (vitamin B9) and other B vitamins in the pathophysiology and treatment of depression.
Folate is available in several forms, including LMF, which differs from dietary folate and synthetic folic acid supplements because it’s a reduced metabolite that readily crosses the blood-brain barrier.
“This is a ‘shortcut’ that gets directly to the brain, especially in those with higher BMI or inflammatory indicators, allowing their antidepressant to work better,” Dr. Maletic said.
LMF is available as a prescription medical food and approved for the clinical dietary management of patients with MDD.
The authors wanted to understand the potential role of LMF in treating patients with MDD with insufficient response to current antidepressant therapy.
They analyzed six studies:
- Two multicenter, randomized, double-blind, placebo-controlled sequential parallel trials for patients with SSRI-resistant MDD (n = 148 and n = 75).
- A 12-month open-label extension trial of the two randomized, controlled trials (n = 68).
- A retrospective cohort study evaluating patients previously prescribed LMF (n = 554).
- Two post hoc exploratory analyses of the second randomized, controlled trial, stratifying patients by specific biological and genetic markers (n = 74) and evaluating the effect of biomarkers on treatment effect (n = 74).
The primary endpoints were improvement on the 17-item Hamilton Depression Rating Scale (HDRS-17) or the Patient Health Questionnaire (PHQ-9).
Patients in all trials were treated with either 7.5 mg or 15 mg of LMF.
Both RCTs were divided into two 30-day phases, with patients assessed every 10 days. Response was defined as at least a 50% reduction in HDRS-17 score during treatment or a final score of 7 or less.
‘Salvage pathway’
In the RCTs, patients who received 7.5 mg of LMF did not achieve efficacy superior to placebo, while those receiving 15 mg/day of LMF for 30 days showed significantly greater reduction in HDRS-17 scores (–5.6 vs. –3.0; P = .05, respectively) and higher response rates (32.3% vs. 14.6%; P = .05, respectively).
The 12-month open extension trial showed that among patients who received the 15-mg dose, 61% achieved remission at any point, and 38% achieved recovery. Among initial nonresponders, 60% eventually achieved remission, with no serious adverse events.
“These results indicate that patients who respond well to shorter-term treatment are likely to maintain that response over the subsequent year and shows that those not adequately responding within the first 8 weeks of therapy may benefit from longer-term LMF treatments,” the investigators noted.
In the prospective observational study, the pooled mean change in PHQ-9 was –8.5, with response and remission rates of 67.9% and 45.7%, respectively.
“These outcomes suggest that the results seen in the controlled trial are likely to extend to patients in real-world practice,” the researchers wrote.
The post hoc analyses focusing on the findings of the two RCTs explored the differences in response to LMF, based on biomarker, BMI, and genotype.
Individuals with BMI less than 30 did not have a significant change from baseline with LMF treatment, in contrast to those with BMI of 30 or higher (pooled treatment effect, –4.66;95% CI, –7.22 to –1.98) – a difference the authors call “striking.”
Levels of inflammatory markers (tumor necrosis factor–alpha, interleukin-8, heart-specific C-reactive protein, and leptin) above the median value were associated with significantly greater treatment effect – a finding that remained significant even after adjustment for BMI.
Although BMI and cytokines all showed significant main effects, the “synergy” between them “suggests that these risk factors may interact with each other to influence response to LMF,” the authors wrote.
The mechanism by which LMF augments antidepressant treatment is tied to monoamine synthesis, since LMF promotes the synthesis of key monoamine neurotransmitters associated with MDD (serotonin, norepinephrine, and dopamine), Dr. Maletic explained.
High levels of inflammation (often tied to obesity) cause oxidative stress, which inhibits the synthesis of these neurotransmitters and depletes them more rapidly. LMF provides a “salvage pathway” that may prevent this from happening, thus increasing the antidepressant response of the monoamines, he said.
A ‘good addition’
In a comment, David Mischoulon, MD, PhD, Joyce R. Tedlow Professor of Psychiatry at Harvard Medical School and director of the depression clinical and research program at Massachusetts General Hospital, both in Boston, said the paper “does a good job of synthesizing what we know about LMF as an adjunctive treatment in major depression.”

However, he recommended “caution” when interpreting the findings, since “relatively few” studies were reviewed.
Dr. Mischoulon, who was not involved with the study, said that a “particularly interesting finding from these studies is individuals who are overweight and/or have elevation in inflammatory activity ... seemed to respond better to the addition of LMF.” This finding is similar to what his research team observed when investigating the potential role of fish oils in treating depression.
“These findings overall are not surprising, in view of the well-established multidirectional relationship between depression, inflammation, and overweight status,” he said.
LMF “seems like a good addition to the pharmacological armamentarium for depression; and because it is safe and has minimal side effects, it can be added to the treatment regimen of patients who are depressed and not responding adequately to standard antidepressants,” he said.
This work was funded by Alfasigma USA. The authors did not receive payment for their participation. Dr. Maletic has received writing support from Alfasigma USA; consulting/advisory fees from AbbVie/Allergan, Acadia, Alfasigma USA, Alkermes, Eisai-Purdue, Intra-Cellular Therapies, Janssen, Lundbeck, Jazz, Noven, Otsuka America, Sage, Sunovion, Supernus, and Takeda; and honoraria for lectures from AbbVie, Acadia, Alkermes, Allergan, Eisai, Ironshore, Intra-Cellular, Janssen, Lundbeck, Otsuka America, Sunovion, Supernus, and Takeda. Dr. Mischoulon has received research support from Nordic Naturals and Heckel Medizintechnik. He has received honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy, PeerPoint Medical Education Institute, and Harvard blog.
A version of this article first appeared on Medscape.com.
The investigators analyzed six studies and found support for adjunctive use of LMF with patients with MDD not responding to antidepressant monotherapy. Treatment response was highest in those with obesity and inflammatory biomarkers.
“If clinicians try LMF on their patients with treatment-resistant depression, the treatment is very robust in patients who have high BMI [body mass index] or inflammatory biomarkers, and it’s worth a try even in patients who don’t have these indicators, since it’s safe and well tolerated, with no downside,” study investigator Vladimir Maletic, MD, MS, clinical professor of psychiatry and behavioral science, University of South Carolina, Greenville, said in an interview.
The study was published online in the Journal of Clinical Psychiatry.
‘Shortcut’ to the brain
A considerable percentage of patients with MDD fail to achieve an adequate response to treatment, the authors wrote.
Previous research shows benefits of folate (vitamin B9) and other B vitamins in the pathophysiology and treatment of depression.
Folate is available in several forms, including LMF, which differs from dietary folate and synthetic folic acid supplements because it’s a reduced metabolite that readily crosses the blood-brain barrier.
“This is a ‘shortcut’ that gets directly to the brain, especially in those with higher BMI or inflammatory indicators, allowing their antidepressant to work better,” Dr. Maletic said.
LMF is available as a prescription medical food and approved for the clinical dietary management of patients with MDD.
The authors wanted to understand the potential role of LMF in treating patients with MDD with insufficient response to current antidepressant therapy.
They analyzed six studies:
- Two multicenter, randomized, double-blind, placebo-controlled sequential parallel trials for patients with SSRI-resistant MDD (n = 148 and n = 75).
- A 12-month open-label extension trial of the two randomized, controlled trials (n = 68).
- A retrospective cohort study evaluating patients previously prescribed LMF (n = 554).
- Two post hoc exploratory analyses of the second randomized, controlled trial, stratifying patients by specific biological and genetic markers (n = 74) and evaluating the effect of biomarkers on treatment effect (n = 74).
The primary endpoints were improvement on the 17-item Hamilton Depression Rating Scale (HDRS-17) or the Patient Health Questionnaire (PHQ-9).
Patients in all trials were treated with either 7.5 mg or 15 mg of LMF.
Both RCTs were divided into two 30-day phases, with patients assessed every 10 days. Response was defined as at least a 50% reduction in HDRS-17 score during treatment or a final score of 7 or less.
‘Salvage pathway’
In the RCTs, patients who received 7.5 mg of LMF did not achieve efficacy superior to placebo, while those receiving 15 mg/day of LMF for 30 days showed significantly greater reduction in HDRS-17 scores (–5.6 vs. –3.0; P = .05, respectively) and higher response rates (32.3% vs. 14.6%; P = .05, respectively).
The 12-month open extension trial showed that among patients who received the 15-mg dose, 61% achieved remission at any point, and 38% achieved recovery. Among initial nonresponders, 60% eventually achieved remission, with no serious adverse events.
“These results indicate that patients who respond well to shorter-term treatment are likely to maintain that response over the subsequent year and shows that those not adequately responding within the first 8 weeks of therapy may benefit from longer-term LMF treatments,” the investigators noted.
In the prospective observational study, the pooled mean change in PHQ-9 was –8.5, with response and remission rates of 67.9% and 45.7%, respectively.
“These outcomes suggest that the results seen in the controlled trial are likely to extend to patients in real-world practice,” the researchers wrote.
The post hoc analyses focusing on the findings of the two RCTs explored the differences in response to LMF, based on biomarker, BMI, and genotype.
Individuals with BMI less than 30 did not have a significant change from baseline with LMF treatment, in contrast to those with BMI of 30 or higher (pooled treatment effect, –4.66;95% CI, –7.22 to –1.98) – a difference the authors call “striking.”
Levels of inflammatory markers (tumor necrosis factor–alpha, interleukin-8, heart-specific C-reactive protein, and leptin) above the median value were associated with significantly greater treatment effect – a finding that remained significant even after adjustment for BMI.
Although BMI and cytokines all showed significant main effects, the “synergy” between them “suggests that these risk factors may interact with each other to influence response to LMF,” the authors wrote.
The mechanism by which LMF augments antidepressant treatment is tied to monoamine synthesis, since LMF promotes the synthesis of key monoamine neurotransmitters associated with MDD (serotonin, norepinephrine, and dopamine), Dr. Maletic explained.
High levels of inflammation (often tied to obesity) cause oxidative stress, which inhibits the synthesis of these neurotransmitters and depletes them more rapidly. LMF provides a “salvage pathway” that may prevent this from happening, thus increasing the antidepressant response of the monoamines, he said.
A ‘good addition’
In a comment, David Mischoulon, MD, PhD, Joyce R. Tedlow Professor of Psychiatry at Harvard Medical School and director of the depression clinical and research program at Massachusetts General Hospital, both in Boston, said the paper “does a good job of synthesizing what we know about LMF as an adjunctive treatment in major depression.”
However, he recommended “caution” when interpreting the findings, since “relatively few” studies were reviewed.
Dr. Mischoulon, who was not involved with the study, said that a “particularly interesting finding from these studies is individuals who are overweight and/or have elevation in inflammatory activity ... seemed to respond better to the addition of LMF.” This finding is similar to what his research team observed when investigating the potential role of fish oils in treating depression.
“These findings overall are not surprising, in view of the well-established multidirectional relationship between depression, inflammation, and overweight status,” he said.
LMF “seems like a good addition to the pharmacological armamentarium for depression; and because it is safe and has minimal side effects, it can be added to the treatment regimen of patients who are depressed and not responding adequately to standard antidepressants,” he said.
This work was funded by Alfasigma USA. The authors did not receive payment for their participation. Dr. Maletic has received writing support from Alfasigma USA; consulting/advisory fees from AbbVie/Allergan, Acadia, Alfasigma USA, Alkermes, Eisai-Purdue, Intra-Cellular Therapies, Janssen, Lundbeck, Jazz, Noven, Otsuka America, Sage, Sunovion, Supernus, and Takeda; and honoraria for lectures from AbbVie, Acadia, Alkermes, Allergan, Eisai, Ironshore, Intra-Cellular, Janssen, Lundbeck, Otsuka America, Sunovion, Supernus, and Takeda. Dr. Mischoulon has received research support from Nordic Naturals and Heckel Medizintechnik. He has received honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy, PeerPoint Medical Education Institute, and Harvard blog.
A version of this article first appeared on Medscape.com.
The investigators analyzed six studies and found support for adjunctive use of LMF with patients with MDD not responding to antidepressant monotherapy. Treatment response was highest in those with obesity and inflammatory biomarkers.
“If clinicians try LMF on their patients with treatment-resistant depression, the treatment is very robust in patients who have high BMI [body mass index] or inflammatory biomarkers, and it’s worth a try even in patients who don’t have these indicators, since it’s safe and well tolerated, with no downside,” study investigator Vladimir Maletic, MD, MS, clinical professor of psychiatry and behavioral science, University of South Carolina, Greenville, said in an interview.
The study was published online in the Journal of Clinical Psychiatry.
‘Shortcut’ to the brain
A considerable percentage of patients with MDD fail to achieve an adequate response to treatment, the authors wrote.
Previous research shows benefits of folate (vitamin B9) and other B vitamins in the pathophysiology and treatment of depression.
Folate is available in several forms, including LMF, which differs from dietary folate and synthetic folic acid supplements because it’s a reduced metabolite that readily crosses the blood-brain barrier.
“This is a ‘shortcut’ that gets directly to the brain, especially in those with higher BMI or inflammatory indicators, allowing their antidepressant to work better,” Dr. Maletic said.
LMF is available as a prescription medical food and approved for the clinical dietary management of patients with MDD.
The authors wanted to understand the potential role of LMF in treating patients with MDD with insufficient response to current antidepressant therapy.
They analyzed six studies:
- Two multicenter, randomized, double-blind, placebo-controlled sequential parallel trials for patients with SSRI-resistant MDD (n = 148 and n = 75).
- A 12-month open-label extension trial of the two randomized, controlled trials (n = 68).
- A retrospective cohort study evaluating patients previously prescribed LMF (n = 554).
- Two post hoc exploratory analyses of the second randomized, controlled trial, stratifying patients by specific biological and genetic markers (n = 74) and evaluating the effect of biomarkers on treatment effect (n = 74).
The primary endpoints were improvement on the 17-item Hamilton Depression Rating Scale (HDRS-17) or the Patient Health Questionnaire (PHQ-9).
Patients in all trials were treated with either 7.5 mg or 15 mg of LMF.
Both RCTs were divided into two 30-day phases, with patients assessed every 10 days. Response was defined as at least a 50% reduction in HDRS-17 score during treatment or a final score of 7 or less.
‘Salvage pathway’
In the RCTs, patients who received 7.5 mg of LMF did not achieve efficacy superior to placebo, while those receiving 15 mg/day of LMF for 30 days showed significantly greater reduction in HDRS-17 scores (–5.6 vs. –3.0; P = .05, respectively) and higher response rates (32.3% vs. 14.6%; P = .05, respectively).
The 12-month open extension trial showed that among patients who received the 15-mg dose, 61% achieved remission at any point, and 38% achieved recovery. Among initial nonresponders, 60% eventually achieved remission, with no serious adverse events.
“These results indicate that patients who respond well to shorter-term treatment are likely to maintain that response over the subsequent year and shows that those not adequately responding within the first 8 weeks of therapy may benefit from longer-term LMF treatments,” the investigators noted.
In the prospective observational study, the pooled mean change in PHQ-9 was –8.5, with response and remission rates of 67.9% and 45.7%, respectively.
“These outcomes suggest that the results seen in the controlled trial are likely to extend to patients in real-world practice,” the researchers wrote.
The post hoc analyses focusing on the findings of the two RCTs explored the differences in response to LMF, based on biomarker, BMI, and genotype.
Individuals with BMI less than 30 did not have a significant change from baseline with LMF treatment, in contrast to those with BMI of 30 or higher (pooled treatment effect, –4.66;95% CI, –7.22 to –1.98) – a difference the authors call “striking.”
Levels of inflammatory markers (tumor necrosis factor–alpha, interleukin-8, heart-specific C-reactive protein, and leptin) above the median value were associated with significantly greater treatment effect – a finding that remained significant even after adjustment for BMI.
Although BMI and cytokines all showed significant main effects, the “synergy” between them “suggests that these risk factors may interact with each other to influence response to LMF,” the authors wrote.
The mechanism by which LMF augments antidepressant treatment is tied to monoamine synthesis, since LMF promotes the synthesis of key monoamine neurotransmitters associated with MDD (serotonin, norepinephrine, and dopamine), Dr. Maletic explained.
High levels of inflammation (often tied to obesity) cause oxidative stress, which inhibits the synthesis of these neurotransmitters and depletes them more rapidly. LMF provides a “salvage pathway” that may prevent this from happening, thus increasing the antidepressant response of the monoamines, he said.
A ‘good addition’
In a comment, David Mischoulon, MD, PhD, Joyce R. Tedlow Professor of Psychiatry at Harvard Medical School and director of the depression clinical and research program at Massachusetts General Hospital, both in Boston, said the paper “does a good job of synthesizing what we know about LMF as an adjunctive treatment in major depression.”
However, he recommended “caution” when interpreting the findings, since “relatively few” studies were reviewed.
Dr. Mischoulon, who was not involved with the study, said that a “particularly interesting finding from these studies is individuals who are overweight and/or have elevation in inflammatory activity ... seemed to respond better to the addition of LMF.” This finding is similar to what his research team observed when investigating the potential role of fish oils in treating depression.
“These findings overall are not surprising, in view of the well-established multidirectional relationship between depression, inflammation, and overweight status,” he said.
LMF “seems like a good addition to the pharmacological armamentarium for depression; and because it is safe and has minimal side effects, it can be added to the treatment regimen of patients who are depressed and not responding adequately to standard antidepressants,” he said.
This work was funded by Alfasigma USA. The authors did not receive payment for their participation. Dr. Maletic has received writing support from Alfasigma USA; consulting/advisory fees from AbbVie/Allergan, Acadia, Alfasigma USA, Alkermes, Eisai-Purdue, Intra-Cellular Therapies, Janssen, Lundbeck, Jazz, Noven, Otsuka America, Sage, Sunovion, Supernus, and Takeda; and honoraria for lectures from AbbVie, Acadia, Alkermes, Allergan, Eisai, Ironshore, Intra-Cellular, Janssen, Lundbeck, Otsuka America, Sunovion, Supernus, and Takeda. Dr. Mischoulon has received research support from Nordic Naturals and Heckel Medizintechnik. He has received honoraria for speaking from the Massachusetts General Hospital Psychiatry Academy, PeerPoint Medical Education Institute, and Harvard blog.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Tips, contraindications for superficial chemical peels reviewed
CHICAGO – Heather Woolery-Lloyd, MD, says she’s generally “risk averse,” but when it comes to superficial chemical peels, she’s in her comfort zone.
Superficial peeling is “one of the most common cosmetic procedures that I do,” Dr. Woolery-Lloyd, director of the skin of color division in the dermatology department at the University of Miami, said at the Pigmentary Disorders Exchange Symposium.
In her practice, .

Contraindications are an active bacterial infection, open wounds, and active herpes simplex virus. “If someone looks like they even have a remnant of a cold sore, I tell them to come back,” she said.
Setting expectations for patients is critical, Dr. Woolery-Lloyd said, as a series of superficial peels is needed before the desired results are evident.
The peel she uses most is salicylic acid, a beta-hydroxy acid, at a strength of 20%-30%. “It’s very effective on our acne patients,” she said at the meeting, provided by MedscapeLIVE! “If you’re just starting with peels, I think this is a very safe one. You don’t have to time it, and you don’t have to neutralize it,” and at lower concentrations, is “very safe.”
Dr. Woolery-Lloyd provided these other tips during her presentation:
- Even superficial peels can be uncomfortable, she noted, so she keeps a fan nearby to use when needed to help with discomfort.
- Find the peel you’re comfortable with, master that peel, and don’t jump from peel to peel. Get familiar with the side effects and how to predict results.
- Stop retinoids up to 7 days before a peel. Consider placing the patient on hydroquinone before the chemical peel to decrease the risk of hyperpigmentation.
- Before the procedure, prep the skin with acetone or alcohol. Applying petrolatum helps protect around the eyes, alar crease, and other sensitive areas, “or anywhere you’re concerned about the depth of the peel.”
- Application with rough gauze helps avoid the waste that comes with makeup sponges soaking up the product. It also helps add exfoliation.
- Have everything ready before starting the procedure, including (depending on the peel), a neutralizer or soapless cleanser. Although peels are generally safe, you want to be able to remove one quickly, if needed, without having to leave the room.
- Start with the lowest concentration (salicylic acid or glycolic acid) then titrate up. Ask patients about any reactions they experienced with the previous peel before making the decision on the next concentration.
- For a peel to treat hyperpigmentation, she recommends one peel about every 4 weeks for a series of 5-6 peels.
- After a peel, the patient should use a mineral sunscreen; chemical sunscreens will sting.
Know your comfort zone
Conference chair Pearl Grimes, MD, director of The Vitiligo & Pigmentation Institute of Southern California in Los Angeles, said superficial peels are best for dermatologists new to peeling until they gain comfort with experience.
Superficial and medium-depth peels work well for mild to moderate photoaging, she said at the meeting.
“We know that in darker skin we have more intrinsic aging rather than photoaging. We have more textural changes, hyperpigmentation,” Dr. Grimes said.
For Fitzpatrick skin types I-III, she said, “you can do superficial, medium, and deep peels.” For darker skin types, “I typically stay in the superficial, medium range.”
She said that she uses retinoids to exfoliate before a superficial peel but added, “you’ve got to stop them early because retinoids can make a superficial peel a medium-depth peel.”
Taking photos is important before any procedure, she said, as is spending time with patients clarifying their outcome expectations.
“I love peeling,” Dr. Grimes said. “And it’s cost effective. If you don’t want to spend a ton of money, it’s amazing what you can achieve with chemical peeling.”
When asked by a member of the audience whether they avoid superficial peels in women who are pregnant or breastfeeding, both Dr. Woolery-Lloyd and Dr. Grimes said they do avoid them in those patients.
Dr. Grimes said she tells her patients, especially in the first trimester, “I am the most conservative woman on the planet. I do nothing during the first trimester.”
Dr. Woolery-Lloyd has been a speaker for Ortho Dermatologics, Loreal and EPI, and has done research for Pfizer, Galderma, Allergan, Arcutis, Vyne, Merz, and Eirion. She has been on advisory boards for Loreal, Allergan, Ortho Dermatologics, Pfize,r and Merz. Dr. Grimes reports grant/research Support from Clinuvel Pharmaceuticals, Incyte, Johnson & Johnson, LASEROPTEK, L’Oréal USA, Pfizer, Procter & Gamble, skinbetter science, and Versicolor Technologies, and is on the speakers bureau/receives honoraria for non-CME for Incyte and Procter & Gamble; and is a consultant or is on the advisory board for L’Oréal USA and Procter & Gamble. She has stock options in Versicolor Technologies.
CHICAGO – Heather Woolery-Lloyd, MD, says she’s generally “risk averse,” but when it comes to superficial chemical peels, she’s in her comfort zone.
Superficial peeling is “one of the most common cosmetic procedures that I do,” Dr. Woolery-Lloyd, director of the skin of color division in the dermatology department at the University of Miami, said at the Pigmentary Disorders Exchange Symposium.
In her practice, .
Contraindications are an active bacterial infection, open wounds, and active herpes simplex virus. “If someone looks like they even have a remnant of a cold sore, I tell them to come back,” she said.
Setting expectations for patients is critical, Dr. Woolery-Lloyd said, as a series of superficial peels is needed before the desired results are evident.
The peel she uses most is salicylic acid, a beta-hydroxy acid, at a strength of 20%-30%. “It’s very effective on our acne patients,” she said at the meeting, provided by MedscapeLIVE! “If you’re just starting with peels, I think this is a very safe one. You don’t have to time it, and you don’t have to neutralize it,” and at lower concentrations, is “very safe.”
Dr. Woolery-Lloyd provided these other tips during her presentation:
- Even superficial peels can be uncomfortable, she noted, so she keeps a fan nearby to use when needed to help with discomfort.
- Find the peel you’re comfortable with, master that peel, and don’t jump from peel to peel. Get familiar with the side effects and how to predict results.
- Stop retinoids up to 7 days before a peel. Consider placing the patient on hydroquinone before the chemical peel to decrease the risk of hyperpigmentation.
- Before the procedure, prep the skin with acetone or alcohol. Applying petrolatum helps protect around the eyes, alar crease, and other sensitive areas, “or anywhere you’re concerned about the depth of the peel.”
- Application with rough gauze helps avoid the waste that comes with makeup sponges soaking up the product. It also helps add exfoliation.
- Have everything ready before starting the procedure, including (depending on the peel), a neutralizer or soapless cleanser. Although peels are generally safe, you want to be able to remove one quickly, if needed, without having to leave the room.
- Start with the lowest concentration (salicylic acid or glycolic acid) then titrate up. Ask patients about any reactions they experienced with the previous peel before making the decision on the next concentration.
- For a peel to treat hyperpigmentation, she recommends one peel about every 4 weeks for a series of 5-6 peels.
- After a peel, the patient should use a mineral sunscreen; chemical sunscreens will sting.
Know your comfort zone
Conference chair Pearl Grimes, MD, director of The Vitiligo & Pigmentation Institute of Southern California in Los Angeles, said superficial peels are best for dermatologists new to peeling until they gain comfort with experience.
Superficial and medium-depth peels work well for mild to moderate photoaging, she said at the meeting.
“We know that in darker skin we have more intrinsic aging rather than photoaging. We have more textural changes, hyperpigmentation,” Dr. Grimes said.
For Fitzpatrick skin types I-III, she said, “you can do superficial, medium, and deep peels.” For darker skin types, “I typically stay in the superficial, medium range.”
She said that she uses retinoids to exfoliate before a superficial peel but added, “you’ve got to stop them early because retinoids can make a superficial peel a medium-depth peel.”
Taking photos is important before any procedure, she said, as is spending time with patients clarifying their outcome expectations.
“I love peeling,” Dr. Grimes said. “And it’s cost effective. If you don’t want to spend a ton of money, it’s amazing what you can achieve with chemical peeling.”
When asked by a member of the audience whether they avoid superficial peels in women who are pregnant or breastfeeding, both Dr. Woolery-Lloyd and Dr. Grimes said they do avoid them in those patients.
Dr. Grimes said she tells her patients, especially in the first trimester, “I am the most conservative woman on the planet. I do nothing during the first trimester.”
Dr. Woolery-Lloyd has been a speaker for Ortho Dermatologics, Loreal and EPI, and has done research for Pfizer, Galderma, Allergan, Arcutis, Vyne, Merz, and Eirion. She has been on advisory boards for Loreal, Allergan, Ortho Dermatologics, Pfize,r and Merz. Dr. Grimes reports grant/research Support from Clinuvel Pharmaceuticals, Incyte, Johnson & Johnson, LASEROPTEK, L’Oréal USA, Pfizer, Procter & Gamble, skinbetter science, and Versicolor Technologies, and is on the speakers bureau/receives honoraria for non-CME for Incyte and Procter & Gamble; and is a consultant or is on the advisory board for L’Oréal USA and Procter & Gamble. She has stock options in Versicolor Technologies.
CHICAGO – Heather Woolery-Lloyd, MD, says she’s generally “risk averse,” but when it comes to superficial chemical peels, she’s in her comfort zone.
Superficial peeling is “one of the most common cosmetic procedures that I do,” Dr. Woolery-Lloyd, director of the skin of color division in the dermatology department at the University of Miami, said at the Pigmentary Disorders Exchange Symposium.
In her practice, .
Contraindications are an active bacterial infection, open wounds, and active herpes simplex virus. “If someone looks like they even have a remnant of a cold sore, I tell them to come back,” she said.
Setting expectations for patients is critical, Dr. Woolery-Lloyd said, as a series of superficial peels is needed before the desired results are evident.
The peel she uses most is salicylic acid, a beta-hydroxy acid, at a strength of 20%-30%. “It’s very effective on our acne patients,” she said at the meeting, provided by MedscapeLIVE! “If you’re just starting with peels, I think this is a very safe one. You don’t have to time it, and you don’t have to neutralize it,” and at lower concentrations, is “very safe.”
Dr. Woolery-Lloyd provided these other tips during her presentation:
- Even superficial peels can be uncomfortable, she noted, so she keeps a fan nearby to use when needed to help with discomfort.
- Find the peel you’re comfortable with, master that peel, and don’t jump from peel to peel. Get familiar with the side effects and how to predict results.
- Stop retinoids up to 7 days before a peel. Consider placing the patient on hydroquinone before the chemical peel to decrease the risk of hyperpigmentation.
- Before the procedure, prep the skin with acetone or alcohol. Applying petrolatum helps protect around the eyes, alar crease, and other sensitive areas, “or anywhere you’re concerned about the depth of the peel.”
- Application with rough gauze helps avoid the waste that comes with makeup sponges soaking up the product. It also helps add exfoliation.
- Have everything ready before starting the procedure, including (depending on the peel), a neutralizer or soapless cleanser. Although peels are generally safe, you want to be able to remove one quickly, if needed, without having to leave the room.
- Start with the lowest concentration (salicylic acid or glycolic acid) then titrate up. Ask patients about any reactions they experienced with the previous peel before making the decision on the next concentration.
- For a peel to treat hyperpigmentation, she recommends one peel about every 4 weeks for a series of 5-6 peels.
- After a peel, the patient should use a mineral sunscreen; chemical sunscreens will sting.
Know your comfort zone
Conference chair Pearl Grimes, MD, director of The Vitiligo & Pigmentation Institute of Southern California in Los Angeles, said superficial peels are best for dermatologists new to peeling until they gain comfort with experience.
Superficial and medium-depth peels work well for mild to moderate photoaging, she said at the meeting.
“We know that in darker skin we have more intrinsic aging rather than photoaging. We have more textural changes, hyperpigmentation,” Dr. Grimes said.
For Fitzpatrick skin types I-III, she said, “you can do superficial, medium, and deep peels.” For darker skin types, “I typically stay in the superficial, medium range.”
She said that she uses retinoids to exfoliate before a superficial peel but added, “you’ve got to stop them early because retinoids can make a superficial peel a medium-depth peel.”
Taking photos is important before any procedure, she said, as is spending time with patients clarifying their outcome expectations.
“I love peeling,” Dr. Grimes said. “And it’s cost effective. If you don’t want to spend a ton of money, it’s amazing what you can achieve with chemical peeling.”
When asked by a member of the audience whether they avoid superficial peels in women who are pregnant or breastfeeding, both Dr. Woolery-Lloyd and Dr. Grimes said they do avoid them in those patients.
Dr. Grimes said she tells her patients, especially in the first trimester, “I am the most conservative woman on the planet. I do nothing during the first trimester.”
Dr. Woolery-Lloyd has been a speaker for Ortho Dermatologics, Loreal and EPI, and has done research for Pfizer, Galderma, Allergan, Arcutis, Vyne, Merz, and Eirion. She has been on advisory boards for Loreal, Allergan, Ortho Dermatologics, Pfize,r and Merz. Dr. Grimes reports grant/research Support from Clinuvel Pharmaceuticals, Incyte, Johnson & Johnson, LASEROPTEK, L’Oréal USA, Pfizer, Procter & Gamble, skinbetter science, and Versicolor Technologies, and is on the speakers bureau/receives honoraria for non-CME for Incyte and Procter & Gamble; and is a consultant or is on the advisory board for L’Oréal USA and Procter & Gamble. She has stock options in Versicolor Technologies.
AT THE MEDSCAPE LIVE! PIGMENTARY DISORDERS SYMPOSIUM
Nitroglycerin patches do not improve menopause symptoms
Vasomotor symptoms affect as many as 75% of menopausal women in the United States. Characterized by a sudden onset of flushing, sweating, and chills, symptoms of hot flashes can be managed with hormone therapy, but prolonged use of the treatment poses health risks. In a study published in JAMA Internal Medicine,
METHODOLOGY
- The was a randomized, double-blinded trial involving 134 California women aged 40-62 years.
- Between July 2018 and December 2021, participants self-administered either a nitroglycerin patch at a dosage of 0.2 to 0.6 mg/h or a placebo patch every night.
- Participants were in the late stages of menopause or had already undergone menopause. They reported having seven or more hot flashes per day; at least four were moderate to severe over a 1-week period.
- The primary outcome was a change in the frequency of hot flashes over 5 and 12 weeks.
TAKEAWAY
- Over 5 weeks, the frequency of moderate to severe hot flashes decreased by 3.3 episodes per day in the nitroglycerine group, compared with 2.2 episodes per day in the placebo group (95% CI, −2.2 to 0; P = .05).
- The reduction in overall frequency of hot flashes – either mild, moderate, or severe – over the 5-week period was not statistically significant.
- Over the 12-week period, no statistically significant reductions in hot flashes occurred.
- More than two thirds of participants assigned to the nitroglycerin patches reported having headaches, while three reported chest pain and one had a syncopal episode.
IN PRACTICE
The findings do not support daily use of nitroglycerin patches to treat vasomotor symptoms, the researchers conclude.
“The bottom line is that our study doesn’t allow us to recommend nitroglycerin skin patches as a strategy for consumers to suppress hot flashes in the long term,” Alison Huang, MD, MAS, lead author of the study, said in a press release. “The menopause field is still lacking in effective treatment approaches that don’t involve hormones.”
STUDY DETAILS
The study was led by Alison Huang, MD, MAS, a professor of medicine at the University of California, San Francisco. Two of the authors reported grants from the National Institute on Aging.
LIMITATIONS
Almost 20% of women who used the nitroglycerin patches discontinued treatment before the end of the trial because they could not tolerate the medication, experienced an adverse event, or their symptoms did not improve, according to the researchers. In addition, the 1-week period used to screen for severity and frequency of hot flashes may have been too short to confirm that symptoms were prolonged, which could explain the better-than-expected results in the placebo group.
DISCLOSURES
One author served on the medical advisory board of SomaLogic. Another author is an unpaid consultant to Astellas Pharma. Another author reported grants from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Vasomotor symptoms affect as many as 75% of menopausal women in the United States. Characterized by a sudden onset of flushing, sweating, and chills, symptoms of hot flashes can be managed with hormone therapy, but prolonged use of the treatment poses health risks. In a study published in JAMA Internal Medicine,
METHODOLOGY
- The was a randomized, double-blinded trial involving 134 California women aged 40-62 years.
- Between July 2018 and December 2021, participants self-administered either a nitroglycerin patch at a dosage of 0.2 to 0.6 mg/h or a placebo patch every night.
- Participants were in the late stages of menopause or had already undergone menopause. They reported having seven or more hot flashes per day; at least four were moderate to severe over a 1-week period.
- The primary outcome was a change in the frequency of hot flashes over 5 and 12 weeks.
TAKEAWAY
- Over 5 weeks, the frequency of moderate to severe hot flashes decreased by 3.3 episodes per day in the nitroglycerine group, compared with 2.2 episodes per day in the placebo group (95% CI, −2.2 to 0; P = .05).
- The reduction in overall frequency of hot flashes – either mild, moderate, or severe – over the 5-week period was not statistically significant.
- Over the 12-week period, no statistically significant reductions in hot flashes occurred.
- More than two thirds of participants assigned to the nitroglycerin patches reported having headaches, while three reported chest pain and one had a syncopal episode.
IN PRACTICE
The findings do not support daily use of nitroglycerin patches to treat vasomotor symptoms, the researchers conclude.
“The bottom line is that our study doesn’t allow us to recommend nitroglycerin skin patches as a strategy for consumers to suppress hot flashes in the long term,” Alison Huang, MD, MAS, lead author of the study, said in a press release. “The menopause field is still lacking in effective treatment approaches that don’t involve hormones.”
STUDY DETAILS
The study was led by Alison Huang, MD, MAS, a professor of medicine at the University of California, San Francisco. Two of the authors reported grants from the National Institute on Aging.
LIMITATIONS
Almost 20% of women who used the nitroglycerin patches discontinued treatment before the end of the trial because they could not tolerate the medication, experienced an adverse event, or their symptoms did not improve, according to the researchers. In addition, the 1-week period used to screen for severity and frequency of hot flashes may have been too short to confirm that symptoms were prolonged, which could explain the better-than-expected results in the placebo group.
DISCLOSURES
One author served on the medical advisory board of SomaLogic. Another author is an unpaid consultant to Astellas Pharma. Another author reported grants from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Vasomotor symptoms affect as many as 75% of menopausal women in the United States. Characterized by a sudden onset of flushing, sweating, and chills, symptoms of hot flashes can be managed with hormone therapy, but prolonged use of the treatment poses health risks. In a study published in JAMA Internal Medicine,
METHODOLOGY
- The was a randomized, double-blinded trial involving 134 California women aged 40-62 years.
- Between July 2018 and December 2021, participants self-administered either a nitroglycerin patch at a dosage of 0.2 to 0.6 mg/h or a placebo patch every night.
- Participants were in the late stages of menopause or had already undergone menopause. They reported having seven or more hot flashes per day; at least four were moderate to severe over a 1-week period.
- The primary outcome was a change in the frequency of hot flashes over 5 and 12 weeks.
TAKEAWAY
- Over 5 weeks, the frequency of moderate to severe hot flashes decreased by 3.3 episodes per day in the nitroglycerine group, compared with 2.2 episodes per day in the placebo group (95% CI, −2.2 to 0; P = .05).
- The reduction in overall frequency of hot flashes – either mild, moderate, or severe – over the 5-week period was not statistically significant.
- Over the 12-week period, no statistically significant reductions in hot flashes occurred.
- More than two thirds of participants assigned to the nitroglycerin patches reported having headaches, while three reported chest pain and one had a syncopal episode.
IN PRACTICE
The findings do not support daily use of nitroglycerin patches to treat vasomotor symptoms, the researchers conclude.
“The bottom line is that our study doesn’t allow us to recommend nitroglycerin skin patches as a strategy for consumers to suppress hot flashes in the long term,” Alison Huang, MD, MAS, lead author of the study, said in a press release. “The menopause field is still lacking in effective treatment approaches that don’t involve hormones.”
STUDY DETAILS
The study was led by Alison Huang, MD, MAS, a professor of medicine at the University of California, San Francisco. Two of the authors reported grants from the National Institute on Aging.
LIMITATIONS
Almost 20% of women who used the nitroglycerin patches discontinued treatment before the end of the trial because they could not tolerate the medication, experienced an adverse event, or their symptoms did not improve, according to the researchers. In addition, the 1-week period used to screen for severity and frequency of hot flashes may have been too short to confirm that symptoms were prolonged, which could explain the better-than-expected results in the placebo group.
DISCLOSURES
One author served on the medical advisory board of SomaLogic. Another author is an unpaid consultant to Astellas Pharma. Another author reported grants from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
`Remarkable’: CAR T therapy for CLL/SLL
The phase 1/2 TRANSCEND CLL 004 trial represents “the first pivotal multicenter trial to evaluate a CAR T-cell therapy in heavily pretreated patients with relapsed or refractory chronic lymphocytic leukemia or small lymphocytic lymphoma,” first author Tanya Siddiqi, MD, associate professor in the division of lymphoma, City of Hope National Medical Center, Duarte, Calif., said in a press statement in connection with her presentation at the annual meeting of the American Society of Clinical Oncology.
“The durable complete responses observed with liso-cel in the TRANSCEND CLL 004 trial are remarkable and represent a major step in bringing a personalized, T cell–based treatment approach delivered as a one-time infusion into clinical practice for a complex and historically incurable disease,” she said.
Real-world evidence shows that patients with CLL or SLL who have relapsed or are refractory to treatment with BTKi therapy can have progressively worse outcomes. Moreover, with few other treatment options, research shows that the median time from dual discontinuation of BTKi and venetoclax to subsequent treatment failure or death is just 5.6 months.
“We are seeing a subset of patients now who are progressing on BTK inhibitors and venetoclax, and there is a high, unmet medical need for new, more effective treatments in this patient population,” Dr. Siddiqi said.
With liso-cel showing efficacy in the treatment of large B-cell lymphoma and receiving approval from the Food and Drug Administration for the indication, the multicenter TRANSCEND CLL 004 trial was launched to investigate the therapy’s effects in r/r CLL/SLL.
In a safety set of 117 patients with r/r CLL or SLL who received at least two prior lines of therapy, including a BTKi, patients received a single target dose of either 50 (n=9) or 100 × 106 (n = 87) CAR-positive T cells.
The primary efficacy analysis set included 49 patients who were treated with the target dose of 100 x 106 CAR-positive viable T cells of liso-cel.
With a median on-study follow-up of 21.1 months, the primary endpoint of a complete response (CR) and complete response was achieved among 18.4% (n = 9; P = .0006).
Among patients achieving a complete response, no disease progression or deaths were reported, with a median duration of response that was not reached.
The undetectable minimal residual disease (MRD) rate was 63.3% in blood and 59.2% in bone marrow, which was associated with progression-free survival.
The overall response rate was 42.9%, which was not statistically significant, and the median duration of an objective response was 35.3 months (95% confidence interval, 11.01 to not reached).
The median time to first response was 1.2 months, and the median time to first complete response was 3.0 months.
The results were consistent in the broader safety set of 117 patients, including those who were heavily pretreated with a median of five prior lines of therapy (range, 2-12) and high-risk disease, with a CR rate of 18.4%.
In terms of safety, no new safety signals were observed, and the treatment’s safety profile was manageable, the authors noted.
Cytokine release syndrome (CRS), common with CAR T-cell therapy, occurred in 85% of patients; however, most cases were low grade; 9% of cases were grade 3, and there were no grade 4 or 5 cases.
Neurologic events occurred among 45%, including grade 3 in 17.9% and grade 4 in 0.9%, with no cases of grade 5.
For treatment of the CRS, 69.2% of patients received tocilizumab and/or corticosteroids for the cases of CRS and neurological events.
Of 51 deaths that occurred while on the study, 43 occurred following liso-cel infusion, including 5 caused by treatment-emergent adverse events occurring within 90 days of liso-cel infusion.
One death was determined to be related to liso-cel, involving macrophage activation syndrome–hemophagocytic lymphohistiocytosis.
“The safety profile was manageable, with low rates of grade 3 or higher CRS and neurotoxicity,” Dr. Siddiqi said.
She noted that, as encouraging as the results are, work should continue regarding further improving survival for patients.
“We need to look at this population more closely to see how we can make it even better for them,” she said in her talk.
For instance, “do we need to add maintenance, or do we need to do something else with CAR T therapy? Because one shot of CAR T is buying them a lot of time – 6 or 12 months of progression-free survival, but maybe we can make it even better.”
Dr. Siddiqi noted that she has “a lot of patients” who received CAR T-cell therapy who have not progressed or relapsed after as long as 4 years.
“I also have some patients who did relapse at 3 or 3 and 1/2 years, but everybody is so thankful for having that time of several years without any treatment; without the need for continuous therapy or continuous doctors’ visits. It is actually priceless,” she said.
Largest data set to date
Commenting on the study, Jakub Svoboda, MD, agreed that the findings suggest an important role of liso-cel among the growing numbers of patients who progress despite standard therapies.
“This is an important study and the [results] are very relevant as there is a growing population of patients with CLL/SLL who stopped responding to both BTKi and venetoclax and have limited options,” Dr. Svoboda, a medical oncologist at Penn Medicine, and associate professor of medicine at the Hospital of the University of Pennsylvania, both in Philadelphia, said in an interview.
“Many of my CLL/SLL patients benefited from BTK inhibitors and venetoclax for years, but it is clear that these are not curative agents, and ultimately our patients need other effective therapeutic options,” he said. “We have seen reports of smaller single-site studies with different anti-CD19 CAR T-cell products used in CLL/SLL in the past, but this multisite study using liso-cel represents the largest data set in over 100 patients with median follow-up of 21 months.”
Liso-cel, like other CAR T-cell treatments – which are derived from patients’ own cells that are then reengineered and delivered via a one-time infusion – has a 4-1BB costimulatory domain. This has the effect of enhancing the expansion and persistence of the CAR T cells.
Significantly, the study establishes that CAR T-cell manufacturing in CLL/SLL patients is feasible on a large scale, “which is important, considering the unique T-lymphocyte biology in CLL/SLL,” Dr. Svoboda remarked.
In terms of efficacy, “I have been mostly impressed by the high degree of undetectable minimal residual disease and the duration of response in the cohort of patients who previously failed both BTKi and venetoclax,” he added. “While there are a few agents used or being developed for patients failing both BTKi and venetoclax, it appears that CAR T-cell therapy has the unique potential to achieve long-term remissions in a subset of these patients.”
Discussant Carolyn Owen, MD, an associate professor in the division of hematology and hematological malignancies, University of Calgary (Alta.), and hematologist at the Tom Baker Cancer Centre, also in Calgary, also expressed enthusiasm over the encouraging results.
“The results of this study are very exciting,” she said during her discussion in the session.
“What is really important is that, even though this may be a small proportion of all of the patients, if we start offering this therapy a little bit earlier, and don’t wait for people to become completely refractory, we could increase the proportion of patients who are [not relapsing].”
Furthermore, “what’s most groundbreaking about this study is that patients could indeed have a really durable remission,” Dr. Owen added. “Hopefully not relapsing even beyond this 20-month follow up, which we haven’t seen with any of our other therapies.”
The results were also published in The Lancet.
The study was sponsored by Juno Therapeutics. Dr. Siddiqi disclosed relationships with Acerta Pharma, Ascentage Pharma, AstraZeneca, BeiGene, Bristol-Myers Squibb/Sanofi, Celgene, Juno Therapeutics, Kite, Oncternal Therapeutics, Pharmacyclics, and TG Therapeutics. Dr. Svoboda reported ties with Bristol-Myers Squibb. Dr. Owen disclosed relationships with Janssen, AstraZeneca, Roche Canada, AbbVie, Novartis Canada Pharmaceuticals, BeiGene, Merck, Incyte, and Seagen.
The phase 1/2 TRANSCEND CLL 004 trial represents “the first pivotal multicenter trial to evaluate a CAR T-cell therapy in heavily pretreated patients with relapsed or refractory chronic lymphocytic leukemia or small lymphocytic lymphoma,” first author Tanya Siddiqi, MD, associate professor in the division of lymphoma, City of Hope National Medical Center, Duarte, Calif., said in a press statement in connection with her presentation at the annual meeting of the American Society of Clinical Oncology.
“The durable complete responses observed with liso-cel in the TRANSCEND CLL 004 trial are remarkable and represent a major step in bringing a personalized, T cell–based treatment approach delivered as a one-time infusion into clinical practice for a complex and historically incurable disease,” she said.
Real-world evidence shows that patients with CLL or SLL who have relapsed or are refractory to treatment with BTKi therapy can have progressively worse outcomes. Moreover, with few other treatment options, research shows that the median time from dual discontinuation of BTKi and venetoclax to subsequent treatment failure or death is just 5.6 months.
“We are seeing a subset of patients now who are progressing on BTK inhibitors and venetoclax, and there is a high, unmet medical need for new, more effective treatments in this patient population,” Dr. Siddiqi said.
With liso-cel showing efficacy in the treatment of large B-cell lymphoma and receiving approval from the Food and Drug Administration for the indication, the multicenter TRANSCEND CLL 004 trial was launched to investigate the therapy’s effects in r/r CLL/SLL.
In a safety set of 117 patients with r/r CLL or SLL who received at least two prior lines of therapy, including a BTKi, patients received a single target dose of either 50 (n=9) or 100 × 106 (n = 87) CAR-positive T cells.
The primary efficacy analysis set included 49 patients who were treated with the target dose of 100 x 106 CAR-positive viable T cells of liso-cel.
With a median on-study follow-up of 21.1 months, the primary endpoint of a complete response (CR) and complete response was achieved among 18.4% (n = 9; P = .0006).
Among patients achieving a complete response, no disease progression or deaths were reported, with a median duration of response that was not reached.
The undetectable minimal residual disease (MRD) rate was 63.3% in blood and 59.2% in bone marrow, which was associated with progression-free survival.
The overall response rate was 42.9%, which was not statistically significant, and the median duration of an objective response was 35.3 months (95% confidence interval, 11.01 to not reached).
The median time to first response was 1.2 months, and the median time to first complete response was 3.0 months.
The results were consistent in the broader safety set of 117 patients, including those who were heavily pretreated with a median of five prior lines of therapy (range, 2-12) and high-risk disease, with a CR rate of 18.4%.
In terms of safety, no new safety signals were observed, and the treatment’s safety profile was manageable, the authors noted.
Cytokine release syndrome (CRS), common with CAR T-cell therapy, occurred in 85% of patients; however, most cases were low grade; 9% of cases were grade 3, and there were no grade 4 or 5 cases.
Neurologic events occurred among 45%, including grade 3 in 17.9% and grade 4 in 0.9%, with no cases of grade 5.
For treatment of the CRS, 69.2% of patients received tocilizumab and/or corticosteroids for the cases of CRS and neurological events.
Of 51 deaths that occurred while on the study, 43 occurred following liso-cel infusion, including 5 caused by treatment-emergent adverse events occurring within 90 days of liso-cel infusion.
One death was determined to be related to liso-cel, involving macrophage activation syndrome–hemophagocytic lymphohistiocytosis.
“The safety profile was manageable, with low rates of grade 3 or higher CRS and neurotoxicity,” Dr. Siddiqi said.
She noted that, as encouraging as the results are, work should continue regarding further improving survival for patients.
“We need to look at this population more closely to see how we can make it even better for them,” she said in her talk.
For instance, “do we need to add maintenance, or do we need to do something else with CAR T therapy? Because one shot of CAR T is buying them a lot of time – 6 or 12 months of progression-free survival, but maybe we can make it even better.”
Dr. Siddiqi noted that she has “a lot of patients” who received CAR T-cell therapy who have not progressed or relapsed after as long as 4 years.
“I also have some patients who did relapse at 3 or 3 and 1/2 years, but everybody is so thankful for having that time of several years without any treatment; without the need for continuous therapy or continuous doctors’ visits. It is actually priceless,” she said.
Largest data set to date
Commenting on the study, Jakub Svoboda, MD, agreed that the findings suggest an important role of liso-cel among the growing numbers of patients who progress despite standard therapies.
“This is an important study and the [results] are very relevant as there is a growing population of patients with CLL/SLL who stopped responding to both BTKi and venetoclax and have limited options,” Dr. Svoboda, a medical oncologist at Penn Medicine, and associate professor of medicine at the Hospital of the University of Pennsylvania, both in Philadelphia, said in an interview.
“Many of my CLL/SLL patients benefited from BTK inhibitors and venetoclax for years, but it is clear that these are not curative agents, and ultimately our patients need other effective therapeutic options,” he said. “We have seen reports of smaller single-site studies with different anti-CD19 CAR T-cell products used in CLL/SLL in the past, but this multisite study using liso-cel represents the largest data set in over 100 patients with median follow-up of 21 months.”
Liso-cel, like other CAR T-cell treatments – which are derived from patients’ own cells that are then reengineered and delivered via a one-time infusion – has a 4-1BB costimulatory domain. This has the effect of enhancing the expansion and persistence of the CAR T cells.
Significantly, the study establishes that CAR T-cell manufacturing in CLL/SLL patients is feasible on a large scale, “which is important, considering the unique T-lymphocyte biology in CLL/SLL,” Dr. Svoboda remarked.
In terms of efficacy, “I have been mostly impressed by the high degree of undetectable minimal residual disease and the duration of response in the cohort of patients who previously failed both BTKi and venetoclax,” he added. “While there are a few agents used or being developed for patients failing both BTKi and venetoclax, it appears that CAR T-cell therapy has the unique potential to achieve long-term remissions in a subset of these patients.”
Discussant Carolyn Owen, MD, an associate professor in the division of hematology and hematological malignancies, University of Calgary (Alta.), and hematologist at the Tom Baker Cancer Centre, also in Calgary, also expressed enthusiasm over the encouraging results.
“The results of this study are very exciting,” she said during her discussion in the session.
“What is really important is that, even though this may be a small proportion of all of the patients, if we start offering this therapy a little bit earlier, and don’t wait for people to become completely refractory, we could increase the proportion of patients who are [not relapsing].”
Furthermore, “what’s most groundbreaking about this study is that patients could indeed have a really durable remission,” Dr. Owen added. “Hopefully not relapsing even beyond this 20-month follow up, which we haven’t seen with any of our other therapies.”
The results were also published in The Lancet.
The study was sponsored by Juno Therapeutics. Dr. Siddiqi disclosed relationships with Acerta Pharma, Ascentage Pharma, AstraZeneca, BeiGene, Bristol-Myers Squibb/Sanofi, Celgene, Juno Therapeutics, Kite, Oncternal Therapeutics, Pharmacyclics, and TG Therapeutics. Dr. Svoboda reported ties with Bristol-Myers Squibb. Dr. Owen disclosed relationships with Janssen, AstraZeneca, Roche Canada, AbbVie, Novartis Canada Pharmaceuticals, BeiGene, Merck, Incyte, and Seagen.
The phase 1/2 TRANSCEND CLL 004 trial represents “the first pivotal multicenter trial to evaluate a CAR T-cell therapy in heavily pretreated patients with relapsed or refractory chronic lymphocytic leukemia or small lymphocytic lymphoma,” first author Tanya Siddiqi, MD, associate professor in the division of lymphoma, City of Hope National Medical Center, Duarte, Calif., said in a press statement in connection with her presentation at the annual meeting of the American Society of Clinical Oncology.
“The durable complete responses observed with liso-cel in the TRANSCEND CLL 004 trial are remarkable and represent a major step in bringing a personalized, T cell–based treatment approach delivered as a one-time infusion into clinical practice for a complex and historically incurable disease,” she said.
Real-world evidence shows that patients with CLL or SLL who have relapsed or are refractory to treatment with BTKi therapy can have progressively worse outcomes. Moreover, with few other treatment options, research shows that the median time from dual discontinuation of BTKi and venetoclax to subsequent treatment failure or death is just 5.6 months.
“We are seeing a subset of patients now who are progressing on BTK inhibitors and venetoclax, and there is a high, unmet medical need for new, more effective treatments in this patient population,” Dr. Siddiqi said.
With liso-cel showing efficacy in the treatment of large B-cell lymphoma and receiving approval from the Food and Drug Administration for the indication, the multicenter TRANSCEND CLL 004 trial was launched to investigate the therapy’s effects in r/r CLL/SLL.
In a safety set of 117 patients with r/r CLL or SLL who received at least two prior lines of therapy, including a BTKi, patients received a single target dose of either 50 (n=9) or 100 × 106 (n = 87) CAR-positive T cells.
The primary efficacy analysis set included 49 patients who were treated with the target dose of 100 x 106 CAR-positive viable T cells of liso-cel.
With a median on-study follow-up of 21.1 months, the primary endpoint of a complete response (CR) and complete response was achieved among 18.4% (n = 9; P = .0006).
Among patients achieving a complete response, no disease progression or deaths were reported, with a median duration of response that was not reached.
The undetectable minimal residual disease (MRD) rate was 63.3% in blood and 59.2% in bone marrow, which was associated with progression-free survival.
The overall response rate was 42.9%, which was not statistically significant, and the median duration of an objective response was 35.3 months (95% confidence interval, 11.01 to not reached).
The median time to first response was 1.2 months, and the median time to first complete response was 3.0 months.
The results were consistent in the broader safety set of 117 patients, including those who were heavily pretreated with a median of five prior lines of therapy (range, 2-12) and high-risk disease, with a CR rate of 18.4%.
In terms of safety, no new safety signals were observed, and the treatment’s safety profile was manageable, the authors noted.
Cytokine release syndrome (CRS), common with CAR T-cell therapy, occurred in 85% of patients; however, most cases were low grade; 9% of cases were grade 3, and there were no grade 4 or 5 cases.
Neurologic events occurred among 45%, including grade 3 in 17.9% and grade 4 in 0.9%, with no cases of grade 5.
For treatment of the CRS, 69.2% of patients received tocilizumab and/or corticosteroids for the cases of CRS and neurological events.
Of 51 deaths that occurred while on the study, 43 occurred following liso-cel infusion, including 5 caused by treatment-emergent adverse events occurring within 90 days of liso-cel infusion.
One death was determined to be related to liso-cel, involving macrophage activation syndrome–hemophagocytic lymphohistiocytosis.
“The safety profile was manageable, with low rates of grade 3 or higher CRS and neurotoxicity,” Dr. Siddiqi said.
She noted that, as encouraging as the results are, work should continue regarding further improving survival for patients.
“We need to look at this population more closely to see how we can make it even better for them,” she said in her talk.
For instance, “do we need to add maintenance, or do we need to do something else with CAR T therapy? Because one shot of CAR T is buying them a lot of time – 6 or 12 months of progression-free survival, but maybe we can make it even better.”
Dr. Siddiqi noted that she has “a lot of patients” who received CAR T-cell therapy who have not progressed or relapsed after as long as 4 years.
“I also have some patients who did relapse at 3 or 3 and 1/2 years, but everybody is so thankful for having that time of several years without any treatment; without the need for continuous therapy or continuous doctors’ visits. It is actually priceless,” she said.
Largest data set to date
Commenting on the study, Jakub Svoboda, MD, agreed that the findings suggest an important role of liso-cel among the growing numbers of patients who progress despite standard therapies.
“This is an important study and the [results] are very relevant as there is a growing population of patients with CLL/SLL who stopped responding to both BTKi and venetoclax and have limited options,” Dr. Svoboda, a medical oncologist at Penn Medicine, and associate professor of medicine at the Hospital of the University of Pennsylvania, both in Philadelphia, said in an interview.
“Many of my CLL/SLL patients benefited from BTK inhibitors and venetoclax for years, but it is clear that these are not curative agents, and ultimately our patients need other effective therapeutic options,” he said. “We have seen reports of smaller single-site studies with different anti-CD19 CAR T-cell products used in CLL/SLL in the past, but this multisite study using liso-cel represents the largest data set in over 100 patients with median follow-up of 21 months.”
Liso-cel, like other CAR T-cell treatments – which are derived from patients’ own cells that are then reengineered and delivered via a one-time infusion – has a 4-1BB costimulatory domain. This has the effect of enhancing the expansion and persistence of the CAR T cells.
Significantly, the study establishes that CAR T-cell manufacturing in CLL/SLL patients is feasible on a large scale, “which is important, considering the unique T-lymphocyte biology in CLL/SLL,” Dr. Svoboda remarked.
In terms of efficacy, “I have been mostly impressed by the high degree of undetectable minimal residual disease and the duration of response in the cohort of patients who previously failed both BTKi and venetoclax,” he added. “While there are a few agents used or being developed for patients failing both BTKi and venetoclax, it appears that CAR T-cell therapy has the unique potential to achieve long-term remissions in a subset of these patients.”
Discussant Carolyn Owen, MD, an associate professor in the division of hematology and hematological malignancies, University of Calgary (Alta.), and hematologist at the Tom Baker Cancer Centre, also in Calgary, also expressed enthusiasm over the encouraging results.
“The results of this study are very exciting,” she said during her discussion in the session.
“What is really important is that, even though this may be a small proportion of all of the patients, if we start offering this therapy a little bit earlier, and don’t wait for people to become completely refractory, we could increase the proportion of patients who are [not relapsing].”
Furthermore, “what’s most groundbreaking about this study is that patients could indeed have a really durable remission,” Dr. Owen added. “Hopefully not relapsing even beyond this 20-month follow up, which we haven’t seen with any of our other therapies.”
The results were also published in The Lancet.
The study was sponsored by Juno Therapeutics. Dr. Siddiqi disclosed relationships with Acerta Pharma, Ascentage Pharma, AstraZeneca, BeiGene, Bristol-Myers Squibb/Sanofi, Celgene, Juno Therapeutics, Kite, Oncternal Therapeutics, Pharmacyclics, and TG Therapeutics. Dr. Svoboda reported ties with Bristol-Myers Squibb. Dr. Owen disclosed relationships with Janssen, AstraZeneca, Roche Canada, AbbVie, Novartis Canada Pharmaceuticals, BeiGene, Merck, Incyte, and Seagen.
FROM ASCO 2023
Link between bipolar disorder and CVD mortality explained?
in new findings that may explain the “excessive and premature mortality” related to heart disease in this patient population.
The investigators found that higher reactive hyperemia index (RHI) scores, a measure of endothelial function, were tied to mood severity in patients with higher mania, but not depression scores. These findings persisted even after accounting for medications, obesity, and other cardiovascular risk factors (CVRFs).
“From a clinical perspective, these findings highlight the potential value of integrating vascular health in the assessment and management of youth with BD, and from a scientific perspective, these findings call for additional research focused on shared biological mechanisms linking vascular health and mood symptoms of BD,” senior investigator Benjamin Goldstein, MD, PhD, full professor of psychiatry, pharmacology, and psychological clinical science, University of Toronto, said in an interview.
The study was published online in the Journal of Clinical Psychiatry.
‘Excessively present’
BD is associated with “excessive and premature cardiovascular mortality” and CVD is “excessively present” in BD, exceeding what can be explained by traditional cardiovascular risk factors, psychiatric medications, and substance use, the researchers noted.
“In adults, more severe mood symptoms increase the risk of future CVD. Our focus on endothelial function rose due to the fact that CVD is rare in youth, whereas endothelial dysfunction – considered a precursor of CVD – can be assessed in youth,” said Dr. Goldstein, who holds the RBC Investments Chair in children’s mental health and developmental psychopathology at the Centre for Addiction and Mental Health, Toronto, where he is director of the Centre for Youth Bipolar Disorder.
For this reason, he and his colleagues were “interested in researching whether endothelial dysfunction is associated with mood symptoms in youth with BD.” Ultimately, the motivation was to “inspire new therapeutic opportunities that may improve both cardiovascular and mental health simultaneously.”
To investigate the question, the researchers studied 209 youth aged 13-20 years (n = 114 with BD and 94 healthy controls [HCs]).
In the BD group, there were 34 BD-euthymia, 36 BD-depressed, and 44 BD-hypomanic/mixed; and within the groups who had depression or hypomania/mixed features, 72 were experiencing clinically significant depression.
Participants had to be free of chronic inflammatory illness, use of medications that might be addressing traditional CVRFs, recent infectious diseases, or neurologic conditions.
Participants’ bipolar symptoms, psychosocial functioning, and family history were assessed. In addition, they were asked about treatment, physical and/or sexual abuse, smoking status, and socioeconomic status. Height, weight, waist circumference, blood pressure, and blood tests to assess CVRFs, including C-reactive protein (CRP), were also assessed. RHI was measured via pulse amplitude tonometry, with lower values indicating poorer endothelial function.
Positive affect beneficial?
Compared with HCs, there were fewer White participants in the BD group (78% vs. 55%; P < .001). The BD group also had higher Tanner stage development scores (stage 5: 65% vs. 35%; P = .03; V = 0.21), higher body mass index (BMI, 24.4 ± 4.6 vs. 22.0 ± 4.2; P < .001; d = 0.53), and higher CRP (1.94 ± 3.99 vs. 0.76 ± 0.86; P = .009; d = –0.40).
After controlling for age, sex, and BMI (F3,202 = 4.47; P = .005; np2 = 0.06), the researchers found significant between-group differences in RHI.
Post hoc pairwise comparisons showed RHI to be significantly lower in the BD-depressed versus the HC group (P = .04; d = 0.4). Moreover, the BD-hypomanic/mixed group had significantly higher RHI, compared with the other BD groups and the HC group.
RHI was associated with higher mania scores (beta, 0.26; P = .006), but there was no similar significant association with depression mood scores (beta, 0.01; P = .90).
The mood state differences in RHI and the RHI-mania association remained significant in sensitivity analyses examining the effect of current medication use as well as CVRFs, including lipids, CRP, and blood pressure on RHI.
“We found that youth with BD experiencing a depressive episode had lower endothelial function, whereas youth with BD experiencing a hypomanic/mixed episode had higher endothelial function, as compared to healthy youth,” Dr. Goldstein said.
There are several mechanisms potentially underlying the association between endothelial function and hypomania, the investigators noted. For example, positive affect is associated with increased endothelial function in normative samples, so hypomanic symptoms, including elation, may have similar beneficial associations, although those benefits likely do not extend to mania, which has been associated with cardiovascular risk.
They also point to several limitations in the study. The cross-sectional design “precludes making inferences regarding the temporal relationship between RHI and mood.” Moreover, the study focused only on hypomania, so “we cannot draw conclusions about mania.” In addition, the HC group had a “significantly higher proportion” of White participants, and a lower Tanner stage, so it “may not be a representative control sample.”
Nevertheless, the researchers concluded that the study “adds to the existing evidence for the potential value of integrating cardiovascular-related therapeutic approaches in BD,” noting that further research is needed to elucidate the mechanisms of the association.
Observable changes in youth
In a comment, Jess G Fiedorowicz, MD, PhD, head and chief, department of mental health, Ottawa Hospital Research Institute, noted that individuals with BD “have a much higher risk of CVD, which tends to develop earlier and shortens life expectancy by more than a decade.”
This cardiovascular risk “appears to be acquired over the long-term course of illness and proportionate to the persistence and severity of mood symptoms, which implies that mood syndromes, such as depression and mania, themselves may induce changes in the body relevant to CVD,” said Dr. Fiedorowicz, who is also a professor in the department of psychiatry and senior research chair in adult psychiatry at the Brain and Mind Research Institute, University of Ottawa, and was not involved with the study.
The study “adds to a growing body of evidence that mood syndromes may enact physiological changes that may be relevant to risk of CVD. One important aspect of this study is that this can even be observed in young sample,” he said.
This study was funded by the Canadian Institutes of Health Research and a Miner’s Lamp Innovation Fund from the University of Toronto. Dr. Goldstein and coauthors declare no relevant financial relationships. Dr. Fiedorowicz receives an honorarium from Elsevier for his work as editor-in-chief of the Journal of Psychosomatic Research.
A version of this article first appeared on Medscape.com.
in new findings that may explain the “excessive and premature mortality” related to heart disease in this patient population.
The investigators found that higher reactive hyperemia index (RHI) scores, a measure of endothelial function, were tied to mood severity in patients with higher mania, but not depression scores. These findings persisted even after accounting for medications, obesity, and other cardiovascular risk factors (CVRFs).
“From a clinical perspective, these findings highlight the potential value of integrating vascular health in the assessment and management of youth with BD, and from a scientific perspective, these findings call for additional research focused on shared biological mechanisms linking vascular health and mood symptoms of BD,” senior investigator Benjamin Goldstein, MD, PhD, full professor of psychiatry, pharmacology, and psychological clinical science, University of Toronto, said in an interview.
The study was published online in the Journal of Clinical Psychiatry.
‘Excessively present’
BD is associated with “excessive and premature cardiovascular mortality” and CVD is “excessively present” in BD, exceeding what can be explained by traditional cardiovascular risk factors, psychiatric medications, and substance use, the researchers noted.
“In adults, more severe mood symptoms increase the risk of future CVD. Our focus on endothelial function rose due to the fact that CVD is rare in youth, whereas endothelial dysfunction – considered a precursor of CVD – can be assessed in youth,” said Dr. Goldstein, who holds the RBC Investments Chair in children’s mental health and developmental psychopathology at the Centre for Addiction and Mental Health, Toronto, where he is director of the Centre for Youth Bipolar Disorder.
For this reason, he and his colleagues were “interested in researching whether endothelial dysfunction is associated with mood symptoms in youth with BD.” Ultimately, the motivation was to “inspire new therapeutic opportunities that may improve both cardiovascular and mental health simultaneously.”
To investigate the question, the researchers studied 209 youth aged 13-20 years (n = 114 with BD and 94 healthy controls [HCs]).
In the BD group, there were 34 BD-euthymia, 36 BD-depressed, and 44 BD-hypomanic/mixed; and within the groups who had depression or hypomania/mixed features, 72 were experiencing clinically significant depression.
Participants had to be free of chronic inflammatory illness, use of medications that might be addressing traditional CVRFs, recent infectious diseases, or neurologic conditions.
Participants’ bipolar symptoms, psychosocial functioning, and family history were assessed. In addition, they were asked about treatment, physical and/or sexual abuse, smoking status, and socioeconomic status. Height, weight, waist circumference, blood pressure, and blood tests to assess CVRFs, including C-reactive protein (CRP), were also assessed. RHI was measured via pulse amplitude tonometry, with lower values indicating poorer endothelial function.
Positive affect beneficial?
Compared with HCs, there were fewer White participants in the BD group (78% vs. 55%; P < .001). The BD group also had higher Tanner stage development scores (stage 5: 65% vs. 35%; P = .03; V = 0.21), higher body mass index (BMI, 24.4 ± 4.6 vs. 22.0 ± 4.2; P < .001; d = 0.53), and higher CRP (1.94 ± 3.99 vs. 0.76 ± 0.86; P = .009; d = –0.40).
After controlling for age, sex, and BMI (F3,202 = 4.47; P = .005; np2 = 0.06), the researchers found significant between-group differences in RHI.
Post hoc pairwise comparisons showed RHI to be significantly lower in the BD-depressed versus the HC group (P = .04; d = 0.4). Moreover, the BD-hypomanic/mixed group had significantly higher RHI, compared with the other BD groups and the HC group.
RHI was associated with higher mania scores (beta, 0.26; P = .006), but there was no similar significant association with depression mood scores (beta, 0.01; P = .90).
The mood state differences in RHI and the RHI-mania association remained significant in sensitivity analyses examining the effect of current medication use as well as CVRFs, including lipids, CRP, and blood pressure on RHI.
“We found that youth with BD experiencing a depressive episode had lower endothelial function, whereas youth with BD experiencing a hypomanic/mixed episode had higher endothelial function, as compared to healthy youth,” Dr. Goldstein said.
There are several mechanisms potentially underlying the association between endothelial function and hypomania, the investigators noted. For example, positive affect is associated with increased endothelial function in normative samples, so hypomanic symptoms, including elation, may have similar beneficial associations, although those benefits likely do not extend to mania, which has been associated with cardiovascular risk.
They also point to several limitations in the study. The cross-sectional design “precludes making inferences regarding the temporal relationship between RHI and mood.” Moreover, the study focused only on hypomania, so “we cannot draw conclusions about mania.” In addition, the HC group had a “significantly higher proportion” of White participants, and a lower Tanner stage, so it “may not be a representative control sample.”
Nevertheless, the researchers concluded that the study “adds to the existing evidence for the potential value of integrating cardiovascular-related therapeutic approaches in BD,” noting that further research is needed to elucidate the mechanisms of the association.
Observable changes in youth
In a comment, Jess G Fiedorowicz, MD, PhD, head and chief, department of mental health, Ottawa Hospital Research Institute, noted that individuals with BD “have a much higher risk of CVD, which tends to develop earlier and shortens life expectancy by more than a decade.”
This cardiovascular risk “appears to be acquired over the long-term course of illness and proportionate to the persistence and severity of mood symptoms, which implies that mood syndromes, such as depression and mania, themselves may induce changes in the body relevant to CVD,” said Dr. Fiedorowicz, who is also a professor in the department of psychiatry and senior research chair in adult psychiatry at the Brain and Mind Research Institute, University of Ottawa, and was not involved with the study.
The study “adds to a growing body of evidence that mood syndromes may enact physiological changes that may be relevant to risk of CVD. One important aspect of this study is that this can even be observed in young sample,” he said.
This study was funded by the Canadian Institutes of Health Research and a Miner’s Lamp Innovation Fund from the University of Toronto. Dr. Goldstein and coauthors declare no relevant financial relationships. Dr. Fiedorowicz receives an honorarium from Elsevier for his work as editor-in-chief of the Journal of Psychosomatic Research.
A version of this article first appeared on Medscape.com.
in new findings that may explain the “excessive and premature mortality” related to heart disease in this patient population.
The investigators found that higher reactive hyperemia index (RHI) scores, a measure of endothelial function, were tied to mood severity in patients with higher mania, but not depression scores. These findings persisted even after accounting for medications, obesity, and other cardiovascular risk factors (CVRFs).
“From a clinical perspective, these findings highlight the potential value of integrating vascular health in the assessment and management of youth with BD, and from a scientific perspective, these findings call for additional research focused on shared biological mechanisms linking vascular health and mood symptoms of BD,” senior investigator Benjamin Goldstein, MD, PhD, full professor of psychiatry, pharmacology, and psychological clinical science, University of Toronto, said in an interview.
The study was published online in the Journal of Clinical Psychiatry.
‘Excessively present’
BD is associated with “excessive and premature cardiovascular mortality” and CVD is “excessively present” in BD, exceeding what can be explained by traditional cardiovascular risk factors, psychiatric medications, and substance use, the researchers noted.
“In adults, more severe mood symptoms increase the risk of future CVD. Our focus on endothelial function rose due to the fact that CVD is rare in youth, whereas endothelial dysfunction – considered a precursor of CVD – can be assessed in youth,” said Dr. Goldstein, who holds the RBC Investments Chair in children’s mental health and developmental psychopathology at the Centre for Addiction and Mental Health, Toronto, where he is director of the Centre for Youth Bipolar Disorder.
For this reason, he and his colleagues were “interested in researching whether endothelial dysfunction is associated with mood symptoms in youth with BD.” Ultimately, the motivation was to “inspire new therapeutic opportunities that may improve both cardiovascular and mental health simultaneously.”
To investigate the question, the researchers studied 209 youth aged 13-20 years (n = 114 with BD and 94 healthy controls [HCs]).
In the BD group, there were 34 BD-euthymia, 36 BD-depressed, and 44 BD-hypomanic/mixed; and within the groups who had depression or hypomania/mixed features, 72 were experiencing clinically significant depression.
Participants had to be free of chronic inflammatory illness, use of medications that might be addressing traditional CVRFs, recent infectious diseases, or neurologic conditions.
Participants’ bipolar symptoms, psychosocial functioning, and family history were assessed. In addition, they were asked about treatment, physical and/or sexual abuse, smoking status, and socioeconomic status. Height, weight, waist circumference, blood pressure, and blood tests to assess CVRFs, including C-reactive protein (CRP), were also assessed. RHI was measured via pulse amplitude tonometry, with lower values indicating poorer endothelial function.
Positive affect beneficial?
Compared with HCs, there were fewer White participants in the BD group (78% vs. 55%; P < .001). The BD group also had higher Tanner stage development scores (stage 5: 65% vs. 35%; P = .03; V = 0.21), higher body mass index (BMI, 24.4 ± 4.6 vs. 22.0 ± 4.2; P < .001; d = 0.53), and higher CRP (1.94 ± 3.99 vs. 0.76 ± 0.86; P = .009; d = –0.40).
After controlling for age, sex, and BMI (F3,202 = 4.47; P = .005; np2 = 0.06), the researchers found significant between-group differences in RHI.
Post hoc pairwise comparisons showed RHI to be significantly lower in the BD-depressed versus the HC group (P = .04; d = 0.4). Moreover, the BD-hypomanic/mixed group had significantly higher RHI, compared with the other BD groups and the HC group.
RHI was associated with higher mania scores (beta, 0.26; P = .006), but there was no similar significant association with depression mood scores (beta, 0.01; P = .90).
The mood state differences in RHI and the RHI-mania association remained significant in sensitivity analyses examining the effect of current medication use as well as CVRFs, including lipids, CRP, and blood pressure on RHI.
“We found that youth with BD experiencing a depressive episode had lower endothelial function, whereas youth with BD experiencing a hypomanic/mixed episode had higher endothelial function, as compared to healthy youth,” Dr. Goldstein said.
There are several mechanisms potentially underlying the association between endothelial function and hypomania, the investigators noted. For example, positive affect is associated with increased endothelial function in normative samples, so hypomanic symptoms, including elation, may have similar beneficial associations, although those benefits likely do not extend to mania, which has been associated with cardiovascular risk.
They also point to several limitations in the study. The cross-sectional design “precludes making inferences regarding the temporal relationship between RHI and mood.” Moreover, the study focused only on hypomania, so “we cannot draw conclusions about mania.” In addition, the HC group had a “significantly higher proportion” of White participants, and a lower Tanner stage, so it “may not be a representative control sample.”
Nevertheless, the researchers concluded that the study “adds to the existing evidence for the potential value of integrating cardiovascular-related therapeutic approaches in BD,” noting that further research is needed to elucidate the mechanisms of the association.
Observable changes in youth
In a comment, Jess G Fiedorowicz, MD, PhD, head and chief, department of mental health, Ottawa Hospital Research Institute, noted that individuals with BD “have a much higher risk of CVD, which tends to develop earlier and shortens life expectancy by more than a decade.”
This cardiovascular risk “appears to be acquired over the long-term course of illness and proportionate to the persistence and severity of mood symptoms, which implies that mood syndromes, such as depression and mania, themselves may induce changes in the body relevant to CVD,” said Dr. Fiedorowicz, who is also a professor in the department of psychiatry and senior research chair in adult psychiatry at the Brain and Mind Research Institute, University of Ottawa, and was not involved with the study.
The study “adds to a growing body of evidence that mood syndromes may enact physiological changes that may be relevant to risk of CVD. One important aspect of this study is that this can even be observed in young sample,” he said.
This study was funded by the Canadian Institutes of Health Research and a Miner’s Lamp Innovation Fund from the University of Toronto. Dr. Goldstein and coauthors declare no relevant financial relationships. Dr. Fiedorowicz receives an honorarium from Elsevier for his work as editor-in-chief of the Journal of Psychosomatic Research.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Survival similar with hearts donated after circulatory or brain death
in the first randomized trial comparing the two approaches.
“This randomized trial showing recipient survival with DCD to be similar to DBD should lead to DCD becoming the standard of care alongside DBD,” lead author Jacob Schroder, MD, surgical director, heart transplantation program, Duke University Medical Center, Durham, N.C., said in an interview.
“This should enable many more heart transplants to take place and for us to be able to cast the net further and wider for donors,” he said.
The trial was published online in the New England Journal of Medicine.
Dr. Schroder estimated that only around one-fifth of the 120 U.S. heart transplant centers currently carry out DCD transplants, but he is hopeful that the publication of this study will encourage more transplant centers to do these DCD procedures.
“The problem is there are many low-volume heart transplant centers, which may not be keen to do DCD transplants as they are a bit more complicated and expensive than DBD heart transplants,” he said. “But we need to look at the big picture of how many lives can be saved by increasing the number of heart transplant procedures and the money saved by getting more patients off the waiting list.”
The authors explain that heart transplantation has traditionally been limited to the use of hearts obtained from donors after brain death, which allows in situ assessment of cardiac function and of the suitability for transplantation of the donor allograft before surgical procurement.
But because the need for heart transplants far exceeds the availability of suitable donors, the use of DCD hearts has been investigated and this approach is now being pursued in many countries. In the DCD approach, the heart will have stopped beating in the donor, and perfusion techniques are used to restart the organ.
There are two different approaches to restarting the heart in DCD. The first approach involves the heart being removed from the donor and reanimated, preserved, assessed, and transported with the use of a portable extracorporeal perfusion and preservation system (Organ Care System, TransMedics). The second involves restarting the heart in the donor’s body for evaluation before removal and transportation under the traditional cold storage method used for donations after brain death.
The current trial was designed to compare clinical outcomes in patients who had received a heart from a circulatory death donor using the portable extracorporeal perfusion method for DCD transplantation, with outcomes from the traditional method of heart transplantation using organs donated after brain death.
For the randomized, noninferiority trial, adult candidates for heart transplantation were assigned to receive a heart after the circulatory death of the donor or a heart from a donor after brain death if that heart was available first (circulatory-death group) or to receive only a heart that had been preserved with the use of traditional cold storage after the brain death of the donor (brain-death group).
The primary end point was the risk-adjusted survival at 6 months in the as-treated circulatory-death group, as compared with the brain-death group. The primary safety end point was serious adverse events associated with the heart graft at 30 days after transplantation.
A total of 180 patients underwent transplantation, 90 of whom received a heart donated after circulatory death and 90 who received a heart donated after brain death. A total of 166 transplant recipients were included in the as-treated primary analysis (80 who received a heart from a circulatory-death donor and 86 who received a heart from a brain-death donor).
The risk-adjusted 6-month survival in the as-treated population was 94% among recipients of a heart from a circulatory-death donor, as compared with 90% among recipients of a heart from a brain-death donor (P < .001 for noninferiority).
There were no substantial between-group differences in the mean per-patient number of serious adverse events associated with the heart graft at 30 days after transplantation.
Of 101 hearts from circulatory-death donors that were preserved with the use of the perfusion system, 90 were successfully transplanted according to the criteria for lactate trend and overall contractility of the donor heart, which resulted in overall utilization percentage of 89%.
More patients who received a heart from a circulatory-death donor had moderate or severe primary graft dysfunction (22%) than those who received a heart from a brain-death donor (10%). However, graft failure that resulted in retransplantation occurred in two (2.3%) patients who received a heart from a brain-death donor versus zero patients who received a heart from a circulatory-death donor.
The researchers note that the higher incidence of primary graft dysfunction in the circulatory-death group is expected, given the period of warm ischemia that occurs in this approach. But they point out that this did not affect patient or graft survival at 30 days or 1 year.
“Primary graft dysfunction is when the heart doesn’t fully work immediately after transplant and some mechanical support is needed,” Dr. Schroder commented to this news organization. “This occurred more often in the DCD group, but this mechanical support is only temporary, and generally only needed for a day or two.
“It looks like it might take the heart a little longer to start fully functioning after DCD, but our results show this doesn’t seem to affect recipient survival.”
He added: “We’ve started to become more comfortable with DCD. Sometimes it may take a little longer to get the heart working properly on its own, but the rate of mechanical support is now much lower than when we first started doing these procedures. And cardiac MRI on the recipient patients before discharge have shown that the DCD hearts are not more damaged than those from DBD donors.”
The authors also report that there were six donor hearts in the DCD group for which there were protocol deviations of functional warm ischemic time greater than 30 minutes or continuously rising lactate levels and these hearts did not show primary graft dysfunction.
On this observation, Dr. Schroder said: “I think we need to do more work on understanding the ischemic time limits. The current 30 minutes time limit was estimated in animal studies. We need to look more closely at data from actual DCD transplants. While 30 minutes may be too long for a heart from an older donor, the heart from a younger donor may be fine for a longer period of ischemic time as it will be healthier.”
“Exciting” results
In an editorial, Nancy K. Sweitzer, MD, PhD, vice chair of clinical research, department of medicine, and director of clinical research, division of cardiology, Washington University in St. Louis, describes the results of the current study as “exciting,” adding that, “They clearly show the feasibility and safety of transplantation of hearts from circulatory-death donors.”
However, Dr. Sweitzer points out that the sickest patients in the study – those who were United Network for Organ Sharing (UNOS) status 1 and 2 – were more likely to receive a DBD heart and the more stable patients (UNOS 3-6) were more likely to receive a DCD heart.
“This imbalance undoubtedly contributed to the success of the trial in meeting its noninferiority end point. Whether transplantation of hearts from circulatory-death donors is truly safe in our sickest patients with heart failure is not clear,” she says.
However, she concludes, “Although caution and continuous evaluation of data are warranted, the increased use of hearts from circulatory-death donors appears to be safe in the hands of experienced transplantation teams and will launch an exciting phase of learning and improvement.”
“A safely expanded pool of heart donors has the potential to increase fairness and equity in heart transplantation, allowing more persons with heart failure to have access to this lifesaving therapy,” she adds. “Organ donors and transplantation teams will save increasing numbers of lives with this most precious gift.”
The current study was supported by TransMedics. Dr. Schroder reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
in the first randomized trial comparing the two approaches.
“This randomized trial showing recipient survival with DCD to be similar to DBD should lead to DCD becoming the standard of care alongside DBD,” lead author Jacob Schroder, MD, surgical director, heart transplantation program, Duke University Medical Center, Durham, N.C., said in an interview.
“This should enable many more heart transplants to take place and for us to be able to cast the net further and wider for donors,” he said.
The trial was published online in the New England Journal of Medicine.
Dr. Schroder estimated that only around one-fifth of the 120 U.S. heart transplant centers currently carry out DCD transplants, but he is hopeful that the publication of this study will encourage more transplant centers to do these DCD procedures.
“The problem is there are many low-volume heart transplant centers, which may not be keen to do DCD transplants as they are a bit more complicated and expensive than DBD heart transplants,” he said. “But we need to look at the big picture of how many lives can be saved by increasing the number of heart transplant procedures and the money saved by getting more patients off the waiting list.”
The authors explain that heart transplantation has traditionally been limited to the use of hearts obtained from donors after brain death, which allows in situ assessment of cardiac function and of the suitability for transplantation of the donor allograft before surgical procurement.
But because the need for heart transplants far exceeds the availability of suitable donors, the use of DCD hearts has been investigated and this approach is now being pursued in many countries. In the DCD approach, the heart will have stopped beating in the donor, and perfusion techniques are used to restart the organ.
There are two different approaches to restarting the heart in DCD. The first approach involves the heart being removed from the donor and reanimated, preserved, assessed, and transported with the use of a portable extracorporeal perfusion and preservation system (Organ Care System, TransMedics). The second involves restarting the heart in the donor’s body for evaluation before removal and transportation under the traditional cold storage method used for donations after brain death.
The current trial was designed to compare clinical outcomes in patients who had received a heart from a circulatory death donor using the portable extracorporeal perfusion method for DCD transplantation, with outcomes from the traditional method of heart transplantation using organs donated after brain death.
For the randomized, noninferiority trial, adult candidates for heart transplantation were assigned to receive a heart after the circulatory death of the donor or a heart from a donor after brain death if that heart was available first (circulatory-death group) or to receive only a heart that had been preserved with the use of traditional cold storage after the brain death of the donor (brain-death group).
The primary end point was the risk-adjusted survival at 6 months in the as-treated circulatory-death group, as compared with the brain-death group. The primary safety end point was serious adverse events associated with the heart graft at 30 days after transplantation.
A total of 180 patients underwent transplantation, 90 of whom received a heart donated after circulatory death and 90 who received a heart donated after brain death. A total of 166 transplant recipients were included in the as-treated primary analysis (80 who received a heart from a circulatory-death donor and 86 who received a heart from a brain-death donor).
The risk-adjusted 6-month survival in the as-treated population was 94% among recipients of a heart from a circulatory-death donor, as compared with 90% among recipients of a heart from a brain-death donor (P < .001 for noninferiority).
There were no substantial between-group differences in the mean per-patient number of serious adverse events associated with the heart graft at 30 days after transplantation.
Of 101 hearts from circulatory-death donors that were preserved with the use of the perfusion system, 90 were successfully transplanted according to the criteria for lactate trend and overall contractility of the donor heart, which resulted in overall utilization percentage of 89%.
More patients who received a heart from a circulatory-death donor had moderate or severe primary graft dysfunction (22%) than those who received a heart from a brain-death donor (10%). However, graft failure that resulted in retransplantation occurred in two (2.3%) patients who received a heart from a brain-death donor versus zero patients who received a heart from a circulatory-death donor.
The researchers note that the higher incidence of primary graft dysfunction in the circulatory-death group is expected, given the period of warm ischemia that occurs in this approach. But they point out that this did not affect patient or graft survival at 30 days or 1 year.
“Primary graft dysfunction is when the heart doesn’t fully work immediately after transplant and some mechanical support is needed,” Dr. Schroder commented to this news organization. “This occurred more often in the DCD group, but this mechanical support is only temporary, and generally only needed for a day or two.
“It looks like it might take the heart a little longer to start fully functioning after DCD, but our results show this doesn’t seem to affect recipient survival.”
He added: “We’ve started to become more comfortable with DCD. Sometimes it may take a little longer to get the heart working properly on its own, but the rate of mechanical support is now much lower than when we first started doing these procedures. And cardiac MRI on the recipient patients before discharge have shown that the DCD hearts are not more damaged than those from DBD donors.”
The authors also report that there were six donor hearts in the DCD group for which there were protocol deviations of functional warm ischemic time greater than 30 minutes or continuously rising lactate levels and these hearts did not show primary graft dysfunction.
On this observation, Dr. Schroder said: “I think we need to do more work on understanding the ischemic time limits. The current 30 minutes time limit was estimated in animal studies. We need to look more closely at data from actual DCD transplants. While 30 minutes may be too long for a heart from an older donor, the heart from a younger donor may be fine for a longer period of ischemic time as it will be healthier.”
“Exciting” results
In an editorial, Nancy K. Sweitzer, MD, PhD, vice chair of clinical research, department of medicine, and director of clinical research, division of cardiology, Washington University in St. Louis, describes the results of the current study as “exciting,” adding that, “They clearly show the feasibility and safety of transplantation of hearts from circulatory-death donors.”
However, Dr. Sweitzer points out that the sickest patients in the study – those who were United Network for Organ Sharing (UNOS) status 1 and 2 – were more likely to receive a DBD heart and the more stable patients (UNOS 3-6) were more likely to receive a DCD heart.
“This imbalance undoubtedly contributed to the success of the trial in meeting its noninferiority end point. Whether transplantation of hearts from circulatory-death donors is truly safe in our sickest patients with heart failure is not clear,” she says.
However, she concludes, “Although caution and continuous evaluation of data are warranted, the increased use of hearts from circulatory-death donors appears to be safe in the hands of experienced transplantation teams and will launch an exciting phase of learning and improvement.”
“A safely expanded pool of heart donors has the potential to increase fairness and equity in heart transplantation, allowing more persons with heart failure to have access to this lifesaving therapy,” she adds. “Organ donors and transplantation teams will save increasing numbers of lives with this most precious gift.”
The current study was supported by TransMedics. Dr. Schroder reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
in the first randomized trial comparing the two approaches.
“This randomized trial showing recipient survival with DCD to be similar to DBD should lead to DCD becoming the standard of care alongside DBD,” lead author Jacob Schroder, MD, surgical director, heart transplantation program, Duke University Medical Center, Durham, N.C., said in an interview.
“This should enable many more heart transplants to take place and for us to be able to cast the net further and wider for donors,” he said.
The trial was published online in the New England Journal of Medicine.
Dr. Schroder estimated that only around one-fifth of the 120 U.S. heart transplant centers currently carry out DCD transplants, but he is hopeful that the publication of this study will encourage more transplant centers to do these DCD procedures.
“The problem is there are many low-volume heart transplant centers, which may not be keen to do DCD transplants as they are a bit more complicated and expensive than DBD heart transplants,” he said. “But we need to look at the big picture of how many lives can be saved by increasing the number of heart transplant procedures and the money saved by getting more patients off the waiting list.”
The authors explain that heart transplantation has traditionally been limited to the use of hearts obtained from donors after brain death, which allows in situ assessment of cardiac function and of the suitability for transplantation of the donor allograft before surgical procurement.
But because the need for heart transplants far exceeds the availability of suitable donors, the use of DCD hearts has been investigated and this approach is now being pursued in many countries. In the DCD approach, the heart will have stopped beating in the donor, and perfusion techniques are used to restart the organ.
There are two different approaches to restarting the heart in DCD. The first approach involves the heart being removed from the donor and reanimated, preserved, assessed, and transported with the use of a portable extracorporeal perfusion and preservation system (Organ Care System, TransMedics). The second involves restarting the heart in the donor’s body for evaluation before removal and transportation under the traditional cold storage method used for donations after brain death.
The current trial was designed to compare clinical outcomes in patients who had received a heart from a circulatory death donor using the portable extracorporeal perfusion method for DCD transplantation, with outcomes from the traditional method of heart transplantation using organs donated after brain death.
For the randomized, noninferiority trial, adult candidates for heart transplantation were assigned to receive a heart after the circulatory death of the donor or a heart from a donor after brain death if that heart was available first (circulatory-death group) or to receive only a heart that had been preserved with the use of traditional cold storage after the brain death of the donor (brain-death group).
The primary end point was the risk-adjusted survival at 6 months in the as-treated circulatory-death group, as compared with the brain-death group. The primary safety end point was serious adverse events associated with the heart graft at 30 days after transplantation.
A total of 180 patients underwent transplantation, 90 of whom received a heart donated after circulatory death and 90 who received a heart donated after brain death. A total of 166 transplant recipients were included in the as-treated primary analysis (80 who received a heart from a circulatory-death donor and 86 who received a heart from a brain-death donor).
The risk-adjusted 6-month survival in the as-treated population was 94% among recipients of a heart from a circulatory-death donor, as compared with 90% among recipients of a heart from a brain-death donor (P < .001 for noninferiority).
There were no substantial between-group differences in the mean per-patient number of serious adverse events associated with the heart graft at 30 days after transplantation.
Of 101 hearts from circulatory-death donors that were preserved with the use of the perfusion system, 90 were successfully transplanted according to the criteria for lactate trend and overall contractility of the donor heart, which resulted in overall utilization percentage of 89%.
More patients who received a heart from a circulatory-death donor had moderate or severe primary graft dysfunction (22%) than those who received a heart from a brain-death donor (10%). However, graft failure that resulted in retransplantation occurred in two (2.3%) patients who received a heart from a brain-death donor versus zero patients who received a heart from a circulatory-death donor.
The researchers note that the higher incidence of primary graft dysfunction in the circulatory-death group is expected, given the period of warm ischemia that occurs in this approach. But they point out that this did not affect patient or graft survival at 30 days or 1 year.
“Primary graft dysfunction is when the heart doesn’t fully work immediately after transplant and some mechanical support is needed,” Dr. Schroder commented to this news organization. “This occurred more often in the DCD group, but this mechanical support is only temporary, and generally only needed for a day or two.
“It looks like it might take the heart a little longer to start fully functioning after DCD, but our results show this doesn’t seem to affect recipient survival.”
He added: “We’ve started to become more comfortable with DCD. Sometimes it may take a little longer to get the heart working properly on its own, but the rate of mechanical support is now much lower than when we first started doing these procedures. And cardiac MRI on the recipient patients before discharge have shown that the DCD hearts are not more damaged than those from DBD donors.”
The authors also report that there were six donor hearts in the DCD group for which there were protocol deviations of functional warm ischemic time greater than 30 minutes or continuously rising lactate levels and these hearts did not show primary graft dysfunction.
On this observation, Dr. Schroder said: “I think we need to do more work on understanding the ischemic time limits. The current 30 minutes time limit was estimated in animal studies. We need to look more closely at data from actual DCD transplants. While 30 minutes may be too long for a heart from an older donor, the heart from a younger donor may be fine for a longer period of ischemic time as it will be healthier.”
“Exciting” results
In an editorial, Nancy K. Sweitzer, MD, PhD, vice chair of clinical research, department of medicine, and director of clinical research, division of cardiology, Washington University in St. Louis, describes the results of the current study as “exciting,” adding that, “They clearly show the feasibility and safety of transplantation of hearts from circulatory-death donors.”
However, Dr. Sweitzer points out that the sickest patients in the study – those who were United Network for Organ Sharing (UNOS) status 1 and 2 – were more likely to receive a DBD heart and the more stable patients (UNOS 3-6) were more likely to receive a DCD heart.
“This imbalance undoubtedly contributed to the success of the trial in meeting its noninferiority end point. Whether transplantation of hearts from circulatory-death donors is truly safe in our sickest patients with heart failure is not clear,” she says.
However, she concludes, “Although caution and continuous evaluation of data are warranted, the increased use of hearts from circulatory-death donors appears to be safe in the hands of experienced transplantation teams and will launch an exciting phase of learning and improvement.”
“A safely expanded pool of heart donors has the potential to increase fairness and equity in heart transplantation, allowing more persons with heart failure to have access to this lifesaving therapy,” she adds. “Organ donors and transplantation teams will save increasing numbers of lives with this most precious gift.”
The current study was supported by TransMedics. Dr. Schroder reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Unraveling the mechanisms behind FMT efficacy needed to expand its use
A deeper understanding of the mechanisms underlying the success of fecal microbiota transplantation (FMT) is needed to further improve its effectiveness, according to two recent reviews published in Cell Host and Microbe.
how closely the donor’s microbial composition matches the patient’s existing microbiome, and the presence of nonbacterial gut inhabitants like viruses and fungi – affect FMT success, according to a press release.
FMT is most often used to treat recurrent Clostridioides difficile infections, which don’t always respond to antibiotics. Success rates range from 60% to 90%, depending on the administration route and study design, notes an international research team led by Abbas Yadegar, PhD, a medical bacteriologist at the Shahid Beheshti University of Medical Sciences in Tehran, Iran.
The understanding of how FMT works is incomplete, however, and the reasons some patients fail to benefit is unclear, note Dr. Yadegar and colleagues. Little attention has been paid to the role that other components of the patient’s microbiome, along with outside factors, play in the treatment’s success, they add.
“We wanted other researchers to look beyond changes in stool microbial composition and function, which have been the focus of research in the past few years,” Dr. Yadegar’s team said in a statement provided to this news organization.
Dr. Yadegar and colleagues’ review of more than 130 studies summarizes recent evidence on the mechanisms contributing to FMT success against recurrent C. difficile infection, highlights knowledge gaps, and proposes future research directions in the field.
Factors that influence FMT’s effectiveness and the potential the procedure holds for treatment of other diseases associated with gut dysbiosis are the subject of a review of 149 studies by a team of researchers led by Serena Porcari, MD, a gastroenterologist at the Fondazione Policlinico Universitario Gemelli and Università Cattolica del Sacro Cuore, in Rome.
“Our main goal was not only to unravel the different mechanisms of FMT efficacy but also to introduce some mindset shifts that are needed to bring FMT forward, mainly covering the gap that exists between basic scientists and clinicians,” Gianluca Ianiro, MD, PhD, a senior researcher in digestive diseases who works with Dr. Porcari and is the review’s lead author, told this news organization.
Engraftment may influence success
Engraftment of donor microbial strains in recipients appears to be key to the therapeutic success of FMT, both reviews note.
Three factors influence engraftment: the donor’s bacteria fitness relative to the recipient, the bacteria already present in the recipient, and whether antibiotics are used prior to FMT to open a niche for the incoming donor microbes, according to Dr. Yadegar and colleagues.
How to calculate strain engraftment has not yet been standardized in the field, and the number of strains detected in the recipient’s fecal sample is dependent on the depth of sequencing techniques, Dr. Porcari and colleagues note.
The use of whole-genome sequencing has enabled more precise evaluation of engraftment, they add.
“With this approach, microbial engraftment has been associated with clinical success, regardless of the disease, in a large metagenomic metanalysis of 24 FMT trials and almost 1,400 fecal samples,” Dr. Porcari and colleagues write. However, these results have not been replicated, likely because of differences between the studies.
More study on the topic is needed, both articles note.
“Because the recent metagenomics studies compared pre- and post-FMT only in cases with successful treatment outcomes, it is not possible to link engraftment to clinical outcomes,” Dr. Yadegar and colleagues write in their statement to this news organization.
A closer look at donor-recipient pairings
Clinicians usually enlist healthy, carefully screened individuals as FMT donors.
However, both research groups conclude that fine-scale taxonomic and metabolic analyses of donor and recipient microbiomes would better inform clinical decisions, especially when treating diseases other than C. difficile.
This may call for a more personalized approach to choosing donor-recipient pairings. Investigators should assess the patient’s diet and genetic background and how closely the donor’s microbiome matches that of the patient.
“Most studies focused on profiling stool samples before and after FMT without also including functional analyses; therefore, there are still a lot of aspects of host microbial interactions that remain unknown,” write Dr. Yadegar and colleagues in their statement.
Ecologic factors, including diet and host genetics, are often not included in clinical studies of C. difficile, but they “may potentially be the missing links” to treatment failure in the small portion of patients whose condition doesn’t respond to FMT, they write.
Pairing donor-recipient combinations on the basis of dietary patterns and preferences could improve FMT efficacy because the donor microbiota would be preadapted to the recipient’s diet, Dr. Yadegar and colleagues write. The team is examining how donor and recipient diet may affect outcomes.
Dr. Porcari and colleagues add that while some studies support the existence of shared characteristics that make up super-donors, others found that the optimal donor is more patient specific. They call for personalized selection strategies that employ microbiome sequencing tools rather than a “one stool fits all” approach.
Currently, many clinicians aren’t familiar with microbiome sequencing and analysis, but they’ll need to be in the near future, note Dr. Porcari and colleagues.
“Identifying microbiome characteristics that maximize strain engraftment in the FMT will allow clinicians to select the best donor for each single patient,” they write.
The possible role of viruses and fungi
In FMT research, investigators tend to focus on the bacteria in the human microbiome. However, viruses and fungi also appear to play a role, both articles note.
“Other microbial kingdoms that inhabit the intestine should be taken into account when considering predictors of post-FMT microbial transfer,” write Dr. Porcari and colleagues.
Although few studies have examined the gut virome’s impact on FMT effectiveness against C. difficile, the existing research, although limited, indicates that bacteriophage viruses could play a role, Dr. Yadegar and colleagues note. For example, high levels of donor-derived Caudoviralesbacteriophages in recipients were associated with FMT efficacy in one preliminary study, they write.
In a small human study, fecal filtrate from healthy donors who had bacteriophages but no live bacteria successfully treated five patients with recurrent C. difficile infection, Dr. Yadegar and colleagues write.
“Therefore, the idea that viruses may play a role is very provocative,” write Dr. Yadegar’s team in their statement.
It’s important to note that these studies are associative, which means they can’t definitively answer the question of how or whether viruses play a role, Dr. Yadegar’s team added.
Researchers “know even less about how fungi may or may not play a role,” write Dr. Yadegar and colleagues. However, in early research that involved patients who had successfully undergone FMT for C. difficile, there was higher relative abundance of Saccharomyces and Aspergillus, whereas Candida, if prominent, may impede response, they write in their article.
Additionally, to explore whether live bacteria are necessary for FMT to work, Dr. Yadegar and colleagues informed this news organization that they are conducting a study “comparing traditional FMT to a fecal filtrate that contains no live bacteria, but has all other components, to see if we can achieve similar success rates in recurrent C. difficile infection.”
Repeat treatment for sustained response
Dr. Yadegar’s team offered another important takeaway: A single FMT treatment will not sustain a positive response, especially when treating chronic noncommunicable conditions in which intestinal dysbiosis may play a role. Repeat treatment will be needed, as with other chronic conditions. This has been shown even in C. difficile infection.
“Recent studies have documented a significant advantage of repeated FMT over single FMT on the cure rates of recurrent C. difficile,” especially for patients with inflammatory bowel disorder, Dr. Yadegar’s team told this news organization.
“What we don’t know is which patient is likely to respond to microbial-based therapy, or what the dose or frequency should be, or which bacteria are responsible for the effects,” Dr. Yadegar and team said.
Dr. Porcari and colleagues are examining whether FMT could be refined to improve its success against other diseases. This may involve selecting specific donors, monitoring the gut microbiome of both donors and recipients, or using a specific means of delivery, such as lyophilized capsules, Dr. Ianiro said.
A response to FMT for chronic, noncommunicable disorders typically is not sustained long term, note Dr. Porcari and colleagues. However, they add that “sequential transplants have been applied in this setting with promising results, suggesting that chronic modulation of the patient microbiome may be beneficial in noncommunicable chronic disorders.” Dr. Porcari and colleagues point to the success of repeated, long-term FMT in studies of patients with ulcerative colitis and irritable bowel syndrome.
The use of cutting-edge technologies for microbiome assessment and a change in the view of FMT as only an acute, single-use therapy could improve FMT protocols and outcomes for noncommunicable conditions, they write.
Expanding FMT beyond C. difficile
Dr. Yadegar and colleagues’ article “really breaks down what is known about the mechanisms of FMT in C. difficile infection, which is important as other live biotherapeutic products are developed,” Colleen Kelly, MD, an associate professor of medicine at Brown University in Providence, R.I., who was not involved with the reviews, said in an interview.
Dr. Yadegar and colleagues concur. They note in a press release that as the mechanisms behind FMT success are understood, that information should be used to design new standardized therapies.
“Although highly effective, there are substantial drawbacks with [FMT], including infectious risks and sparse long-term safety data,” they write. “Better treatment options for recurrent C. difficile infections that are targeted, safe, and donor-independent are thus desired.”
In December 2022, the U.S. Food and Drug Administration approved the first fecal microbiota product, Rebyota, to prevent recurrence of C. difficile. More recently, in April 2023, the FDA approved Vowst, a pill for treating recurrent C. difficile infections.
Dr. Kelly also noted that the article by Dr. Yadegar and colleagues “may help us understand why a small percentage of patients fail to achieve cure after FMT.”
Regarding Dr. Porcari and colleagues’ article, Dr. Kelly said, “There is a lot of hope that FMT or other gut microbiome therapies will be beneficial for conditions outside of C. difficile.
“They do a good job reviewing the state of the science of FMT and highlight the many unknowns around the use of FMT in conditions outside of C. difficile,” added Dr. Kelly, who has been using FMT to treat C. difficile for more than 15 years.
Data supporting FMT for conditions such as ulcerative colitis and autism are compelling, Dr. Kelly acknowledged. But in her view, FMT isn’t ready for “prime time” outside of C. difficile – at least not yet.
“Academic investigators and those in industry are actively conducting research in many non–C. difficile indications, and I predict we will see the emergence of gut microbiome–based therapies for other indications within the next 5-10 years,” Dr. Kelly said.
Dr. Yadegar reports no relevant financial relationships. One coauthor of the Yadegar study has served on the adjudication board for Finch Therapeutics and has received consulting fees and a speaking honorarium from Rebiotix/Ferring Pharmaceuticals. Dr. Ianiro reports no relevant financial relationships. Dr. Kelly has consulted for Sebela Pharmaceuticals and is one of the principal investigators for the FMT National Patient Registry funded by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
A deeper understanding of the mechanisms underlying the success of fecal microbiota transplantation (FMT) is needed to further improve its effectiveness, according to two recent reviews published in Cell Host and Microbe.
how closely the donor’s microbial composition matches the patient’s existing microbiome, and the presence of nonbacterial gut inhabitants like viruses and fungi – affect FMT success, according to a press release.
FMT is most often used to treat recurrent Clostridioides difficile infections, which don’t always respond to antibiotics. Success rates range from 60% to 90%, depending on the administration route and study design, notes an international research team led by Abbas Yadegar, PhD, a medical bacteriologist at the Shahid Beheshti University of Medical Sciences in Tehran, Iran.
The understanding of how FMT works is incomplete, however, and the reasons some patients fail to benefit is unclear, note Dr. Yadegar and colleagues. Little attention has been paid to the role that other components of the patient’s microbiome, along with outside factors, play in the treatment’s success, they add.
“We wanted other researchers to look beyond changes in stool microbial composition and function, which have been the focus of research in the past few years,” Dr. Yadegar’s team said in a statement provided to this news organization.
Dr. Yadegar and colleagues’ review of more than 130 studies summarizes recent evidence on the mechanisms contributing to FMT success against recurrent C. difficile infection, highlights knowledge gaps, and proposes future research directions in the field.
Factors that influence FMT’s effectiveness and the potential the procedure holds for treatment of other diseases associated with gut dysbiosis are the subject of a review of 149 studies by a team of researchers led by Serena Porcari, MD, a gastroenterologist at the Fondazione Policlinico Universitario Gemelli and Università Cattolica del Sacro Cuore, in Rome.
“Our main goal was not only to unravel the different mechanisms of FMT efficacy but also to introduce some mindset shifts that are needed to bring FMT forward, mainly covering the gap that exists between basic scientists and clinicians,” Gianluca Ianiro, MD, PhD, a senior researcher in digestive diseases who works with Dr. Porcari and is the review’s lead author, told this news organization.
Engraftment may influence success
Engraftment of donor microbial strains in recipients appears to be key to the therapeutic success of FMT, both reviews note.
Three factors influence engraftment: the donor’s bacteria fitness relative to the recipient, the bacteria already present in the recipient, and whether antibiotics are used prior to FMT to open a niche for the incoming donor microbes, according to Dr. Yadegar and colleagues.
How to calculate strain engraftment has not yet been standardized in the field, and the number of strains detected in the recipient’s fecal sample is dependent on the depth of sequencing techniques, Dr. Porcari and colleagues note.
The use of whole-genome sequencing has enabled more precise evaluation of engraftment, they add.
“With this approach, microbial engraftment has been associated with clinical success, regardless of the disease, in a large metagenomic metanalysis of 24 FMT trials and almost 1,400 fecal samples,” Dr. Porcari and colleagues write. However, these results have not been replicated, likely because of differences between the studies.
More study on the topic is needed, both articles note.
“Because the recent metagenomics studies compared pre- and post-FMT only in cases with successful treatment outcomes, it is not possible to link engraftment to clinical outcomes,” Dr. Yadegar and colleagues write in their statement to this news organization.
A closer look at donor-recipient pairings
Clinicians usually enlist healthy, carefully screened individuals as FMT donors.
However, both research groups conclude that fine-scale taxonomic and metabolic analyses of donor and recipient microbiomes would better inform clinical decisions, especially when treating diseases other than C. difficile.
This may call for a more personalized approach to choosing donor-recipient pairings. Investigators should assess the patient’s diet and genetic background and how closely the donor’s microbiome matches that of the patient.
“Most studies focused on profiling stool samples before and after FMT without also including functional analyses; therefore, there are still a lot of aspects of host microbial interactions that remain unknown,” write Dr. Yadegar and colleagues in their statement.
Ecologic factors, including diet and host genetics, are often not included in clinical studies of C. difficile, but they “may potentially be the missing links” to treatment failure in the small portion of patients whose condition doesn’t respond to FMT, they write.
Pairing donor-recipient combinations on the basis of dietary patterns and preferences could improve FMT efficacy because the donor microbiota would be preadapted to the recipient’s diet, Dr. Yadegar and colleagues write. The team is examining how donor and recipient diet may affect outcomes.
Dr. Porcari and colleagues add that while some studies support the existence of shared characteristics that make up super-donors, others found that the optimal donor is more patient specific. They call for personalized selection strategies that employ microbiome sequencing tools rather than a “one stool fits all” approach.
Currently, many clinicians aren’t familiar with microbiome sequencing and analysis, but they’ll need to be in the near future, note Dr. Porcari and colleagues.
“Identifying microbiome characteristics that maximize strain engraftment in the FMT will allow clinicians to select the best donor for each single patient,” they write.
The possible role of viruses and fungi
In FMT research, investigators tend to focus on the bacteria in the human microbiome. However, viruses and fungi also appear to play a role, both articles note.
“Other microbial kingdoms that inhabit the intestine should be taken into account when considering predictors of post-FMT microbial transfer,” write Dr. Porcari and colleagues.
Although few studies have examined the gut virome’s impact on FMT effectiveness against C. difficile, the existing research, although limited, indicates that bacteriophage viruses could play a role, Dr. Yadegar and colleagues note. For example, high levels of donor-derived Caudoviralesbacteriophages in recipients were associated with FMT efficacy in one preliminary study, they write.
In a small human study, fecal filtrate from healthy donors who had bacteriophages but no live bacteria successfully treated five patients with recurrent C. difficile infection, Dr. Yadegar and colleagues write.
“Therefore, the idea that viruses may play a role is very provocative,” write Dr. Yadegar’s team in their statement.
It’s important to note that these studies are associative, which means they can’t definitively answer the question of how or whether viruses play a role, Dr. Yadegar’s team added.
Researchers “know even less about how fungi may or may not play a role,” write Dr. Yadegar and colleagues. However, in early research that involved patients who had successfully undergone FMT for C. difficile, there was higher relative abundance of Saccharomyces and Aspergillus, whereas Candida, if prominent, may impede response, they write in their article.
Additionally, to explore whether live bacteria are necessary for FMT to work, Dr. Yadegar and colleagues informed this news organization that they are conducting a study “comparing traditional FMT to a fecal filtrate that contains no live bacteria, but has all other components, to see if we can achieve similar success rates in recurrent C. difficile infection.”
Repeat treatment for sustained response
Dr. Yadegar’s team offered another important takeaway: A single FMT treatment will not sustain a positive response, especially when treating chronic noncommunicable conditions in which intestinal dysbiosis may play a role. Repeat treatment will be needed, as with other chronic conditions. This has been shown even in C. difficile infection.
“Recent studies have documented a significant advantage of repeated FMT over single FMT on the cure rates of recurrent C. difficile,” especially for patients with inflammatory bowel disorder, Dr. Yadegar’s team told this news organization.
“What we don’t know is which patient is likely to respond to microbial-based therapy, or what the dose or frequency should be, or which bacteria are responsible for the effects,” Dr. Yadegar and team said.
Dr. Porcari and colleagues are examining whether FMT could be refined to improve its success against other diseases. This may involve selecting specific donors, monitoring the gut microbiome of both donors and recipients, or using a specific means of delivery, such as lyophilized capsules, Dr. Ianiro said.
A response to FMT for chronic, noncommunicable disorders typically is not sustained long term, note Dr. Porcari and colleagues. However, they add that “sequential transplants have been applied in this setting with promising results, suggesting that chronic modulation of the patient microbiome may be beneficial in noncommunicable chronic disorders.” Dr. Porcari and colleagues point to the success of repeated, long-term FMT in studies of patients with ulcerative colitis and irritable bowel syndrome.
The use of cutting-edge technologies for microbiome assessment and a change in the view of FMT as only an acute, single-use therapy could improve FMT protocols and outcomes for noncommunicable conditions, they write.
Expanding FMT beyond C. difficile
Dr. Yadegar and colleagues’ article “really breaks down what is known about the mechanisms of FMT in C. difficile infection, which is important as other live biotherapeutic products are developed,” Colleen Kelly, MD, an associate professor of medicine at Brown University in Providence, R.I., who was not involved with the reviews, said in an interview.
Dr. Yadegar and colleagues concur. They note in a press release that as the mechanisms behind FMT success are understood, that information should be used to design new standardized therapies.
“Although highly effective, there are substantial drawbacks with [FMT], including infectious risks and sparse long-term safety data,” they write. “Better treatment options for recurrent C. difficile infections that are targeted, safe, and donor-independent are thus desired.”
In December 2022, the U.S. Food and Drug Administration approved the first fecal microbiota product, Rebyota, to prevent recurrence of C. difficile. More recently, in April 2023, the FDA approved Vowst, a pill for treating recurrent C. difficile infections.
Dr. Kelly also noted that the article by Dr. Yadegar and colleagues “may help us understand why a small percentage of patients fail to achieve cure after FMT.”
Regarding Dr. Porcari and colleagues’ article, Dr. Kelly said, “There is a lot of hope that FMT or other gut microbiome therapies will be beneficial for conditions outside of C. difficile.
“They do a good job reviewing the state of the science of FMT and highlight the many unknowns around the use of FMT in conditions outside of C. difficile,” added Dr. Kelly, who has been using FMT to treat C. difficile for more than 15 years.
Data supporting FMT for conditions such as ulcerative colitis and autism are compelling, Dr. Kelly acknowledged. But in her view, FMT isn’t ready for “prime time” outside of C. difficile – at least not yet.
“Academic investigators and those in industry are actively conducting research in many non–C. difficile indications, and I predict we will see the emergence of gut microbiome–based therapies for other indications within the next 5-10 years,” Dr. Kelly said.
Dr. Yadegar reports no relevant financial relationships. One coauthor of the Yadegar study has served on the adjudication board for Finch Therapeutics and has received consulting fees and a speaking honorarium from Rebiotix/Ferring Pharmaceuticals. Dr. Ianiro reports no relevant financial relationships. Dr. Kelly has consulted for Sebela Pharmaceuticals and is one of the principal investigators for the FMT National Patient Registry funded by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
A deeper understanding of the mechanisms underlying the success of fecal microbiota transplantation (FMT) is needed to further improve its effectiveness, according to two recent reviews published in Cell Host and Microbe.
how closely the donor’s microbial composition matches the patient’s existing microbiome, and the presence of nonbacterial gut inhabitants like viruses and fungi – affect FMT success, according to a press release.
FMT is most often used to treat recurrent Clostridioides difficile infections, which don’t always respond to antibiotics. Success rates range from 60% to 90%, depending on the administration route and study design, notes an international research team led by Abbas Yadegar, PhD, a medical bacteriologist at the Shahid Beheshti University of Medical Sciences in Tehran, Iran.
The understanding of how FMT works is incomplete, however, and the reasons some patients fail to benefit is unclear, note Dr. Yadegar and colleagues. Little attention has been paid to the role that other components of the patient’s microbiome, along with outside factors, play in the treatment’s success, they add.
“We wanted other researchers to look beyond changes in stool microbial composition and function, which have been the focus of research in the past few years,” Dr. Yadegar’s team said in a statement provided to this news organization.
Dr. Yadegar and colleagues’ review of more than 130 studies summarizes recent evidence on the mechanisms contributing to FMT success against recurrent C. difficile infection, highlights knowledge gaps, and proposes future research directions in the field.
Factors that influence FMT’s effectiveness and the potential the procedure holds for treatment of other diseases associated with gut dysbiosis are the subject of a review of 149 studies by a team of researchers led by Serena Porcari, MD, a gastroenterologist at the Fondazione Policlinico Universitario Gemelli and Università Cattolica del Sacro Cuore, in Rome.
“Our main goal was not only to unravel the different mechanisms of FMT efficacy but also to introduce some mindset shifts that are needed to bring FMT forward, mainly covering the gap that exists between basic scientists and clinicians,” Gianluca Ianiro, MD, PhD, a senior researcher in digestive diseases who works with Dr. Porcari and is the review’s lead author, told this news organization.
Engraftment may influence success
Engraftment of donor microbial strains in recipients appears to be key to the therapeutic success of FMT, both reviews note.
Three factors influence engraftment: the donor’s bacteria fitness relative to the recipient, the bacteria already present in the recipient, and whether antibiotics are used prior to FMT to open a niche for the incoming donor microbes, according to Dr. Yadegar and colleagues.
How to calculate strain engraftment has not yet been standardized in the field, and the number of strains detected in the recipient’s fecal sample is dependent on the depth of sequencing techniques, Dr. Porcari and colleagues note.
The use of whole-genome sequencing has enabled more precise evaluation of engraftment, they add.
“With this approach, microbial engraftment has been associated with clinical success, regardless of the disease, in a large metagenomic metanalysis of 24 FMT trials and almost 1,400 fecal samples,” Dr. Porcari and colleagues write. However, these results have not been replicated, likely because of differences between the studies.
More study on the topic is needed, both articles note.
“Because the recent metagenomics studies compared pre- and post-FMT only in cases with successful treatment outcomes, it is not possible to link engraftment to clinical outcomes,” Dr. Yadegar and colleagues write in their statement to this news organization.
A closer look at donor-recipient pairings
Clinicians usually enlist healthy, carefully screened individuals as FMT donors.
However, both research groups conclude that fine-scale taxonomic and metabolic analyses of donor and recipient microbiomes would better inform clinical decisions, especially when treating diseases other than C. difficile.
This may call for a more personalized approach to choosing donor-recipient pairings. Investigators should assess the patient’s diet and genetic background and how closely the donor’s microbiome matches that of the patient.
“Most studies focused on profiling stool samples before and after FMT without also including functional analyses; therefore, there are still a lot of aspects of host microbial interactions that remain unknown,” write Dr. Yadegar and colleagues in their statement.
Ecologic factors, including diet and host genetics, are often not included in clinical studies of C. difficile, but they “may potentially be the missing links” to treatment failure in the small portion of patients whose condition doesn’t respond to FMT, they write.
Pairing donor-recipient combinations on the basis of dietary patterns and preferences could improve FMT efficacy because the donor microbiota would be preadapted to the recipient’s diet, Dr. Yadegar and colleagues write. The team is examining how donor and recipient diet may affect outcomes.
Dr. Porcari and colleagues add that while some studies support the existence of shared characteristics that make up super-donors, others found that the optimal donor is more patient specific. They call for personalized selection strategies that employ microbiome sequencing tools rather than a “one stool fits all” approach.
Currently, many clinicians aren’t familiar with microbiome sequencing and analysis, but they’ll need to be in the near future, note Dr. Porcari and colleagues.
“Identifying microbiome characteristics that maximize strain engraftment in the FMT will allow clinicians to select the best donor for each single patient,” they write.
The possible role of viruses and fungi
In FMT research, investigators tend to focus on the bacteria in the human microbiome. However, viruses and fungi also appear to play a role, both articles note.
“Other microbial kingdoms that inhabit the intestine should be taken into account when considering predictors of post-FMT microbial transfer,” write Dr. Porcari and colleagues.
Although few studies have examined the gut virome’s impact on FMT effectiveness against C. difficile, the existing research, although limited, indicates that bacteriophage viruses could play a role, Dr. Yadegar and colleagues note. For example, high levels of donor-derived Caudoviralesbacteriophages in recipients were associated with FMT efficacy in one preliminary study, they write.
In a small human study, fecal filtrate from healthy donors who had bacteriophages but no live bacteria successfully treated five patients with recurrent C. difficile infection, Dr. Yadegar and colleagues write.
“Therefore, the idea that viruses may play a role is very provocative,” write Dr. Yadegar’s team in their statement.
It’s important to note that these studies are associative, which means they can’t definitively answer the question of how or whether viruses play a role, Dr. Yadegar’s team added.
Researchers “know even less about how fungi may or may not play a role,” write Dr. Yadegar and colleagues. However, in early research that involved patients who had successfully undergone FMT for C. difficile, there was higher relative abundance of Saccharomyces and Aspergillus, whereas Candida, if prominent, may impede response, they write in their article.
Additionally, to explore whether live bacteria are necessary for FMT to work, Dr. Yadegar and colleagues informed this news organization that they are conducting a study “comparing traditional FMT to a fecal filtrate that contains no live bacteria, but has all other components, to see if we can achieve similar success rates in recurrent C. difficile infection.”
Repeat treatment for sustained response
Dr. Yadegar’s team offered another important takeaway: A single FMT treatment will not sustain a positive response, especially when treating chronic noncommunicable conditions in which intestinal dysbiosis may play a role. Repeat treatment will be needed, as with other chronic conditions. This has been shown even in C. difficile infection.
“Recent studies have documented a significant advantage of repeated FMT over single FMT on the cure rates of recurrent C. difficile,” especially for patients with inflammatory bowel disorder, Dr. Yadegar’s team told this news organization.
“What we don’t know is which patient is likely to respond to microbial-based therapy, or what the dose or frequency should be, or which bacteria are responsible for the effects,” Dr. Yadegar and team said.
Dr. Porcari and colleagues are examining whether FMT could be refined to improve its success against other diseases. This may involve selecting specific donors, monitoring the gut microbiome of both donors and recipients, or using a specific means of delivery, such as lyophilized capsules, Dr. Ianiro said.
A response to FMT for chronic, noncommunicable disorders typically is not sustained long term, note Dr. Porcari and colleagues. However, they add that “sequential transplants have been applied in this setting with promising results, suggesting that chronic modulation of the patient microbiome may be beneficial in noncommunicable chronic disorders.” Dr. Porcari and colleagues point to the success of repeated, long-term FMT in studies of patients with ulcerative colitis and irritable bowel syndrome.
The use of cutting-edge technologies for microbiome assessment and a change in the view of FMT as only an acute, single-use therapy could improve FMT protocols and outcomes for noncommunicable conditions, they write.
Expanding FMT beyond C. difficile
Dr. Yadegar and colleagues’ article “really breaks down what is known about the mechanisms of FMT in C. difficile infection, which is important as other live biotherapeutic products are developed,” Colleen Kelly, MD, an associate professor of medicine at Brown University in Providence, R.I., who was not involved with the reviews, said in an interview.
Dr. Yadegar and colleagues concur. They note in a press release that as the mechanisms behind FMT success are understood, that information should be used to design new standardized therapies.
“Although highly effective, there are substantial drawbacks with [FMT], including infectious risks and sparse long-term safety data,” they write. “Better treatment options for recurrent C. difficile infections that are targeted, safe, and donor-independent are thus desired.”
In December 2022, the U.S. Food and Drug Administration approved the first fecal microbiota product, Rebyota, to prevent recurrence of C. difficile. More recently, in April 2023, the FDA approved Vowst, a pill for treating recurrent C. difficile infections.
Dr. Kelly also noted that the article by Dr. Yadegar and colleagues “may help us understand why a small percentage of patients fail to achieve cure after FMT.”
Regarding Dr. Porcari and colleagues’ article, Dr. Kelly said, “There is a lot of hope that FMT or other gut microbiome therapies will be beneficial for conditions outside of C. difficile.
“They do a good job reviewing the state of the science of FMT and highlight the many unknowns around the use of FMT in conditions outside of C. difficile,” added Dr. Kelly, who has been using FMT to treat C. difficile for more than 15 years.
Data supporting FMT for conditions such as ulcerative colitis and autism are compelling, Dr. Kelly acknowledged. But in her view, FMT isn’t ready for “prime time” outside of C. difficile – at least not yet.
“Academic investigators and those in industry are actively conducting research in many non–C. difficile indications, and I predict we will see the emergence of gut microbiome–based therapies for other indications within the next 5-10 years,” Dr. Kelly said.
Dr. Yadegar reports no relevant financial relationships. One coauthor of the Yadegar study has served on the adjudication board for Finch Therapeutics and has received consulting fees and a speaking honorarium from Rebiotix/Ferring Pharmaceuticals. Dr. Ianiro reports no relevant financial relationships. Dr. Kelly has consulted for Sebela Pharmaceuticals and is one of the principal investigators for the FMT National Patient Registry funded by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health.
A version of this article originally appeared on Medscape.com.