User login
When practice-changing results don’t change practice
The highly favorable results of the CheckMate 816 trial of neoadjuvant chemotherapy plus nivolumab for resectable stage IB-IIIA non–small cell lung cancer (NSCLC) were impressive enough to prompt a Food and Drug Administration approval of this combination in March 2022.
For many, this led to a marked shift in how we approached these patients. But in my conversations with many care teams, they have expressed ambivalence about using the chemoimmunotherapy regimen. Some have conveyed to me that the lack of statistically significant improvement in overall survival is a sticking point. Others have expressed uncertainty about the true benefit of neoadjuvant chemotherapy alongside nivolumab for patients with earlier-stage disease, given that 64% of patients in the trial had stage IIIA disease. The benefit of the neoadjuvant combination in patients with low or negative tumor programmed death–ligand 1 (PD-L1) expression also remains a question mark, though the trial found no significant differences in outcomes by PD-L1 subset.
But among many of my colleagues who favor adjuvant over neoadjuvant therapy, it isn’t necessarily the fine points of the data that present the real barrier: it’s the sentiment that “we just don’t favor a neoadjuvant approach at my place.”
If the worry is that a subset of patients who are eligible for up-front surgery may be derailed from the operating room if they experience significant disease progression or a complication during preoperative therapy or that surgery will more difficult after chemoimmunotherapy, those concerns are not supported by evidence. In fact, data on surgical outcomes from CheckMate 816 assessing these issues found that surgery after chemoimmunotherapy was approximately 30 minutes faster than it was after chemotherapy alone. In addition, the combination neoadjuvant chemoimmunotherapy approach was associated with less extensive surgeries, particularly for patients with stage IIIA NSCLC, and patients experienced measurably lower reports of pain and dyspnea as well.
Though postoperative systemic therapy has been our general approach for resectable NSCLC for nearly 2 decades, there are several reasons to focus on neoadjuvant therapy.
First, immunotherapy may work more effectively when the tumor antigens as well as lymph nodes and lymphatic system are present in situ at the time.
Second, patients may be eager to complete their treatment within a 3-month period of just three cycles of systemic therapy followed by surgery rather than receiving their treatment over a prolonged chapter of their lives, starting with surgery followed by four cycles of chemotherapy and 1 year of immunotherapy.
Finally, we can’t ignore the fact that most neoadjuvant therapy is delivered exactly as intended, whereas planned adjuvant therapy is often not started or rarely completed as designed. At most, only about half of appropriate patients for adjuvant chemotherapy even start it, and far less complete a full four cycles or go on to complete prolonged adjuvant immunotherapy.
We also can’t underestimate the value of imaging and pathology findings after patients have completed neoadjuvant therapy. The pathologic complete response rate in CheckMate 816 is predictive of improved event-free survival over time.
And that isn’t just a binary variable of achieving a pathologic complete response or not. The degree of residual, viable tumor after surgery is a continuous variable associated along a spectrum with event-free survival. Our colleagues who treat breast cancer have been able to customize postoperative therapy to improve outcomes on the basis of the results achieved with neoadjuvant therapy. Multidisciplinary gastrointestinal oncology teams have revolutionized outcomes with rectal cancer by transitioning to total neoadjuvant therapy that makes it possible to deliver treatment more reliably and pursue organ-sparing approaches while achieving better survival.
Putting all of this together, I appreciate arguments against the generalizability or the maturity of the data supporting neoadjuvant chemoimmunotherapy for resectable NSCLC. However, sidestepping our most promising advances will harm our patients. Plus, what’s the point of generating practice-changing results if we don’t accept and implement them?
We owe it to our patients to follow the evolving evidence and not just stick to what we’ve always done.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. West serves as web editor for JAMA Oncology, edits and writes several sections on lung cancer for UpToDate, and leads a wide range of continuing medical education and other educational programs.
A version of this article first appeared on Medscape.com.
The highly favorable results of the CheckMate 816 trial of neoadjuvant chemotherapy plus nivolumab for resectable stage IB-IIIA non–small cell lung cancer (NSCLC) were impressive enough to prompt a Food and Drug Administration approval of this combination in March 2022.
For many, this led to a marked shift in how we approached these patients. But in my conversations with many care teams, they have expressed ambivalence about using the chemoimmunotherapy regimen. Some have conveyed to me that the lack of statistically significant improvement in overall survival is a sticking point. Others have expressed uncertainty about the true benefit of neoadjuvant chemotherapy alongside nivolumab for patients with earlier-stage disease, given that 64% of patients in the trial had stage IIIA disease. The benefit of the neoadjuvant combination in patients with low or negative tumor programmed death–ligand 1 (PD-L1) expression also remains a question mark, though the trial found no significant differences in outcomes by PD-L1 subset.
But among many of my colleagues who favor adjuvant over neoadjuvant therapy, it isn’t necessarily the fine points of the data that present the real barrier: it’s the sentiment that “we just don’t favor a neoadjuvant approach at my place.”
If the worry is that a subset of patients who are eligible for up-front surgery may be derailed from the operating room if they experience significant disease progression or a complication during preoperative therapy or that surgery will more difficult after chemoimmunotherapy, those concerns are not supported by evidence. In fact, data on surgical outcomes from CheckMate 816 assessing these issues found that surgery after chemoimmunotherapy was approximately 30 minutes faster than it was after chemotherapy alone. In addition, the combination neoadjuvant chemoimmunotherapy approach was associated with less extensive surgeries, particularly for patients with stage IIIA NSCLC, and patients experienced measurably lower reports of pain and dyspnea as well.
Though postoperative systemic therapy has been our general approach for resectable NSCLC for nearly 2 decades, there are several reasons to focus on neoadjuvant therapy.
First, immunotherapy may work more effectively when the tumor antigens as well as lymph nodes and lymphatic system are present in situ at the time.
Second, patients may be eager to complete their treatment within a 3-month period of just three cycles of systemic therapy followed by surgery rather than receiving their treatment over a prolonged chapter of their lives, starting with surgery followed by four cycles of chemotherapy and 1 year of immunotherapy.
Finally, we can’t ignore the fact that most neoadjuvant therapy is delivered exactly as intended, whereas planned adjuvant therapy is often not started or rarely completed as designed. At most, only about half of appropriate patients for adjuvant chemotherapy even start it, and far less complete a full four cycles or go on to complete prolonged adjuvant immunotherapy.
We also can’t underestimate the value of imaging and pathology findings after patients have completed neoadjuvant therapy. The pathologic complete response rate in CheckMate 816 is predictive of improved event-free survival over time.
And that isn’t just a binary variable of achieving a pathologic complete response or not. The degree of residual, viable tumor after surgery is a continuous variable associated along a spectrum with event-free survival. Our colleagues who treat breast cancer have been able to customize postoperative therapy to improve outcomes on the basis of the results achieved with neoadjuvant therapy. Multidisciplinary gastrointestinal oncology teams have revolutionized outcomes with rectal cancer by transitioning to total neoadjuvant therapy that makes it possible to deliver treatment more reliably and pursue organ-sparing approaches while achieving better survival.
Putting all of this together, I appreciate arguments against the generalizability or the maturity of the data supporting neoadjuvant chemoimmunotherapy for resectable NSCLC. However, sidestepping our most promising advances will harm our patients. Plus, what’s the point of generating practice-changing results if we don’t accept and implement them?
We owe it to our patients to follow the evolving evidence and not just stick to what we’ve always done.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. West serves as web editor for JAMA Oncology, edits and writes several sections on lung cancer for UpToDate, and leads a wide range of continuing medical education and other educational programs.
A version of this article first appeared on Medscape.com.
The highly favorable results of the CheckMate 816 trial of neoadjuvant chemotherapy plus nivolumab for resectable stage IB-IIIA non–small cell lung cancer (NSCLC) were impressive enough to prompt a Food and Drug Administration approval of this combination in March 2022.
For many, this led to a marked shift in how we approached these patients. But in my conversations with many care teams, they have expressed ambivalence about using the chemoimmunotherapy regimen. Some have conveyed to me that the lack of statistically significant improvement in overall survival is a sticking point. Others have expressed uncertainty about the true benefit of neoadjuvant chemotherapy alongside nivolumab for patients with earlier-stage disease, given that 64% of patients in the trial had stage IIIA disease. The benefit of the neoadjuvant combination in patients with low or negative tumor programmed death–ligand 1 (PD-L1) expression also remains a question mark, though the trial found no significant differences in outcomes by PD-L1 subset.
But among many of my colleagues who favor adjuvant over neoadjuvant therapy, it isn’t necessarily the fine points of the data that present the real barrier: it’s the sentiment that “we just don’t favor a neoadjuvant approach at my place.”
If the worry is that a subset of patients who are eligible for up-front surgery may be derailed from the operating room if they experience significant disease progression or a complication during preoperative therapy or that surgery will more difficult after chemoimmunotherapy, those concerns are not supported by evidence. In fact, data on surgical outcomes from CheckMate 816 assessing these issues found that surgery after chemoimmunotherapy was approximately 30 minutes faster than it was after chemotherapy alone. In addition, the combination neoadjuvant chemoimmunotherapy approach was associated with less extensive surgeries, particularly for patients with stage IIIA NSCLC, and patients experienced measurably lower reports of pain and dyspnea as well.
Though postoperative systemic therapy has been our general approach for resectable NSCLC for nearly 2 decades, there are several reasons to focus on neoadjuvant therapy.
First, immunotherapy may work more effectively when the tumor antigens as well as lymph nodes and lymphatic system are present in situ at the time.
Second, patients may be eager to complete their treatment within a 3-month period of just three cycles of systemic therapy followed by surgery rather than receiving their treatment over a prolonged chapter of their lives, starting with surgery followed by four cycles of chemotherapy and 1 year of immunotherapy.
Finally, we can’t ignore the fact that most neoadjuvant therapy is delivered exactly as intended, whereas planned adjuvant therapy is often not started or rarely completed as designed. At most, only about half of appropriate patients for adjuvant chemotherapy even start it, and far less complete a full four cycles or go on to complete prolonged adjuvant immunotherapy.
We also can’t underestimate the value of imaging and pathology findings after patients have completed neoadjuvant therapy. The pathologic complete response rate in CheckMate 816 is predictive of improved event-free survival over time.
And that isn’t just a binary variable of achieving a pathologic complete response or not. The degree of residual, viable tumor after surgery is a continuous variable associated along a spectrum with event-free survival. Our colleagues who treat breast cancer have been able to customize postoperative therapy to improve outcomes on the basis of the results achieved with neoadjuvant therapy. Multidisciplinary gastrointestinal oncology teams have revolutionized outcomes with rectal cancer by transitioning to total neoadjuvant therapy that makes it possible to deliver treatment more reliably and pursue organ-sparing approaches while achieving better survival.
Putting all of this together, I appreciate arguments against the generalizability or the maturity of the data supporting neoadjuvant chemoimmunotherapy for resectable NSCLC. However, sidestepping our most promising advances will harm our patients. Plus, what’s the point of generating practice-changing results if we don’t accept and implement them?
We owe it to our patients to follow the evolving evidence and not just stick to what we’ve always done.
Dr. West is an associate professor at City of Hope Comprehensive Cancer Center in Duarte, Calif., and vice president of network strategy at AccessHope in Los Angeles. Dr. West serves as web editor for JAMA Oncology, edits and writes several sections on lung cancer for UpToDate, and leads a wide range of continuing medical education and other educational programs.
A version of this article first appeared on Medscape.com.
For artificial intelligence, the future is finally here
We are currently on the verge of yet another societal “revolution” that will exert an unprecedented impact on our lives. It may surpass prior seismic cultural breakthroughs like the internet, smartphones, and social media. Artificial intelligence (AI) has been fermenting for several decades, gathering steam to become equivalent (and eventually superior) to human intelligence. The escalation of AI sophistication will be jarring and perhaps change human life in completely unpredictable ways.
Composing thoughts into words and coherent sentences has always been a uniquely human attribute among all living organisms. Now, that sublime feature of the human mind is being simulated, thanks to advances in AI software, ironically created by the human mind itself! On November 30, 2022, Open AI introduced ChatGPT (generative pre-trained transformer), which can generate an article on any topic a user requests. Within a few weeks, it was used by more than 100 million people. ChatGPT is taking the world by storm because it is a harbinger (some pessimists may label it an omen) of how human existence will be radically impacted in the future. Such AI breakthroughs to surpass human intelligence are, ironically, the product of the advanced human brain, which I previously described as concurrently a triumph and a blunder by evolution.1
How we got here, and what’s next
ChatGPT is a large language model based on neural networks.2 It generates realistic text responses to a wide range of questions by mimicking the pattern of language in gargantuan online databases. One Hong Kong–based, AI-powered drug discovery company (Insilico Medicine) declared it published articles generated by AI tools, even before ChatGPT became available. This indicates how AI can be misused in scientific publications and may be hard to detect as a new form of plagiarism.3
The roots of AI date back to the 1950s, when Alan Turing, now considered the father of AI, published a seminal article about creating a machine to “imitate the brain” and to “mimic the behavior of the human.”4 The term “artificial intelligence” was coined in 1989 by McCarthy,5 who defined it as “the science of engineering for making intelligent machines.” Since then, several subsets of AI have been developed:
- Machine learning: The study of computer algorithms to generate hypotheses
- Deep learning: A type of machine learning algorithm that uses multiple layers to progressively extract higher-level features from raw input. (Both machine learning and deep learning are used in the burgeoning fields of computational psychiatry6 and neuroscience research7)
- Expert knowledge system: A computer-based system that mimics human decision-making ability
- Neural networks: An interconnected group of artificial neurons that uses a math or computer model for information processing
- Predictive analytics: An algorithm to predict future outcomes based on historical data.
These subsets of AI have been used to identify psychiatric disorders using neuroimaging data8 and to classify brain disorders.9 There are many potential uses of AI in psychiatry.10,11 My first experience with AI was 13 years ago, when we conducted a project to distinguish fake suicide notes from genuine ones.12 AI was more successful in correctly identifying fake notes (78% correctly detected) than senior psychiatric residents (49%) or even faculty (53%).
AI will dramatically change how humans interact with the world and may lead to enhanced creativity and new explorations and forays into novel, previously unknown horizons. It is expected to significantly boost the global economy by many trillions of dollars over the next decade. Major high-tech companies are vigorously competing to develop their own AI tools like ChatGPT (Microsoft invested $10 billion in Open AI). Google, which owns DeepMind (an AI lab that invented the T in GPT) developed its own chatbot called Bard. Amazon has invested heavily in Stability AI by giving its founder and CEO Emad Mostaque 4,000 Nvidia AI chips to assemble the world’s largest supercomputer (1 year ago, Stability had only 32 AI chips!). Apple recently integrated Stable Diffusion into its latest operating system. Chinese tech giants Alibaba and Baidu also announced their own chatbots to be released soon.
Other competitors include Cohere, Hugging Face, Midjourney, GitHub Copilot, Game Changer, Jasper, and Anthropic, which released Claude as its chatbot at a lower cost than ChatGPT. Open AI also developed Dall-E2 in April 2022, which can generate very realistic images from text, one of which recently won an award at an art competition.
Continue to: One of the major...
One of the major concerns about these AI developments is that chatbots can make errors or disseminate misinformation and even enunciate racist or misogynist statements. The greatest worry is that the ultimate implicit goal of AI is what is called artificial general intelligence (AGI), which can think and learn better than humans. Some fear AGI may wipe out humans as a species, a grave outcome indeed. That’s why AI developers intend to align AGI with “basic human values” in the event it surpasses human intelligence. Some are even calling for a transition from AI to AW (artificial wisdom), with built-in empathy, kindness, self-reflection, acceptance of diverse perspectives, and promotion of prosocial ideas.13
Creating content: artificial intelligence vs human authors
ChatGPT has opened a Pandora’s box of concern about potential plagiarism by students or scientific authors. This has prompted several journals,14 including
- Anosognosia in schizophrenia (Box 1); based on “Is anosognosia a delusion, a negative symptom, or a cognitive deficit?”
Current Psychiatry , January 2022, p. 6-8,14. doi: 10.12788/cp.0210 - Benefits of metformin in psychiatry (Box 2); based on “Beyond diabetes: The beneficial uses of metformin in psychiatry,”
Current Psychiatry , March 2022, p. 7-9. doi: 10.12788/cp.0225 - Epidemic of intellectual constipation (Box 3); based on “From debate to stalemate and hate: An epidemic of intellectual constipation,”
Current Psychiatry , January 2023, p. 3-4. doi: 10.12788/cp.0321 - SWOT analysis of psychiatry (Box 4); based on “Contemporary psychiatry: A SWOT analysis,”
Current Psychiatry , January 2023, p. 16-19,27. doi: 10.12788/cp.0320.
These ChatGPT articles are verbatim as generated, without any copyediting, fact-checking, or addition of reference citations. One can easily notice that while factually acceptable, the ChatGPT articles tend to be rather synthetic, simple, bland, and lacking creative language or going beyond the facts to express personal viewpoints. However, I have no doubt that future versions of ChatGPT or other chatbots will evolve into far more sophisticated products and may match what a human can compose in terms of quality and complexity.
AI has arrived with a bang. Going forward, I predict it will continue to surprise us, with elements of “future shock.” The credit (or blame) belongs to the boundless creativity of human intelligence that is seeking to invent an intelligence higher than its own. Caveat emptor!
Box 1
Anosognosia is a condition in which a person is unaware or unable to recognize their own illness or disability. In schizophrenia, anosognosia can be present in up to 50% of cases and is characterized by a lack of insight into the presence and severity of symptoms.
People with anosognosia in schizophrenia may not believe that they have a mental illness, may deny the reality of their symptoms, or may attribute them to external causes. This can make it difficult for them to comply with treatment, as they may not see the need for medication or other interventions.
Anosognosia is thought to be caused by structural and functional changes in the brain, particularly in areas associated with self-awareness and insight. It is often more severe in people with more severe forms of schizophrenia and may be associated with poorer treatment outcomes.
Effective treatment for anosognosia in schizophrenia typically involves a combination of medication and therapy, as well as strategies for improving insight and awareness of symptoms. Family members and caregivers can also play an important role in helping people with schizophrenia to recognize the presence and impact of their illness, and encouraging them to engage in treatment.
a Based on “Is anosognosia a delusion, a negative symptom, or a cognitive deficit?” Current Psychiatry, January 2022, p. 6-8,14. doi: 10.12788/cp.0210
Box 2
Metformin is a medication commonly used in the treatment of type 2 diabetes. However, there is growing interest in its potential use in psychiatry, particularly in the treatment of certain mental health conditions. Some potential benefits of metformin in psychiatry include:
1. Treatment of mood disorders: Studies have suggested that metformin may be helpful in the treatment of mood disorders, such as depression and bipolar disorder. One proposed mechanism is that metformin may help to regulate glucose metabolism and insulin sensitivity, which in turn may help to stabilize mood.
2. Treatment of schizophrenia: Some studies have suggested that metformin may be helpful in reducing symptoms of schizophrenia, particularly negative symptoms such as social withdrawal and apathy. One proposed mechanism is that metformin may improve brain energy metabolism, which may in turn improve cognitive function and reduce symptoms.
3. Weight management: Metformin has been shown to be effective in weight management, which can be particularly important for people with certain mental health conditions, such as bipolar disorder, where weight gain can be a side effect of medication.
4. Neuroprotection: Metformin has been shown to have neuroprotective effects, which may be beneficial for people with certain mental health conditions, such as Alzheimer’s disease and Parkinson’s disease.
It is important to note that while there is some evidence for the potential benefits of metformin in psychiatry, further research is needed to fully understand its effectiveness and safety in this context. People with mental health conditions should not start taking metformin without first consulting with their healthcare provider.
a Based on “Beyond diabetes: The beneficial uses of metformin in psychiatry,” Current Psychiatry, March 2022, p. 7-9. doi: 10.12788/cp.0225
Box 3
The term “epidemic of intellectual constipation” refers to a phenomenon in which individuals, groups, or even entire societies are seen as lacking the ability to think critically, creatively, or expansively. It can be characterized by a lack of curiosity, a narrow range of interests, and a reluctance to engage with new or challenging ideas.
The cause of this phenomenon can be attributed to a variety of factors, including cultural, social, and educational influences. For example, some argue that a narrow and standardized educational system, as well as a lack of exposure to diverse perspectives, can limit creativity and critical thinking skills. Additionally, the prevalence of social media and other forms of digital media may encourage a focus on immediate gratification and quick information, rather than more in-depth and meaningful engagement with information.
The consequences of this epidemic can be far-reaching and can impact personal, social, and political aspects of life. For instance, a lack of critical thinking skills can lead to the spread of misinformation, while a narrow range of interests can limit personal growth and the ability to connect with others.
To combat the epidemic of intellectual constipation, it’s important to foster critical thinking skills, encourage exposure to diverse perspectives, and encourage a lifelong love of learning. This can be achieved through education, community engagement, and personal effort.
In conclusion, the “epidemic of intellectual constipation” refers to a phenomenon in which individuals, groups, or entire societies lack the ability to think critically, creatively, and expansively. To combat this epidemic, it’s important to foster critical thinking skills, encourage exposure to diverse perspectives, and encourage a lifelong love of learning.
a Based on “From debate to stalemate and hate: An epidemic of intellectual constipation,” Current Psychiatry, January 2023, p. 3-4. doi: 10.12788/cp.0321
Box 4
SWOT analysis is a tool used to assess the strengths, weaknesses, opportunities, and threats of a particular entity or industry. In this case, we will conduct a SWOT analysis of psychiatry as a field of medicine.
Strengths
• Psychiatry plays a crucial role in addressing mental health issues and improving the quality of life of individuals who struggle with them.
• Psychiatry has made significant advances in understanding the biological and psychological underpinnings of mental illness, which has led to the development of more effective treatments.
• There is growing public awareness and acceptance of the importance of mental health, which has led to increased demand for psychiatric services.
• The field of psychiatry attracts many talented and compassionate professionals who are dedicated to helping those in need.
Weaknesses
• There is still a significant stigma associated with mental illness, which can deter individuals from seeking treatment.
• The effectiveness of some psychiatric treatments can be limited, particularly in cases of severe mental illness.
• The shortage of mental health professionals in many areas means that access to psychiatric services may be limited, particularly for individuals with lower incomes.
• The cost of psychiatric treatment can be prohibitively expensive, particularly for individuals without insurance coverage.
Opportunities
• New advances in neuroscience and technology, such as brain imaging and genetic testing, hold promise for improving the accuracy of psychiatric diagnoses and developing more targeted treatments.
• Telepsychiatry and other online mental health services offer new ways to increase access to care and reach individuals in underserved areas.
• Greater collaboration with primary care physicians and other healthcare professionals could improve the integration of mental health services into routine healthcare.
• The ongoing destigmatization of mental illness could lead to greater public acceptance and support for mental health services.
Threats
• The ongoing COVID-19 pandemic has increased the prevalence of mental health issues and placed additional strain on mental health services.
• The shortage of mental health professionals, particularly in certain areas of the country, could worsen in the coming years.
• Changes in healthcare policy, such as cuts to mental health funding or changes to insurance coverage, could limit access to care.
• Misinformation and stigma surrounding mental illness could continue to deter individuals from seeking treatment.
a Based on “Contemporary psychiatry: A SWOT analysis,” Current Psychiatry, January 2023, p. 16-19,27. doi: 10.12788/cp.0320
1. Nasrallah HA. Is evolution’s greatest triumph its worst blunder? Current Psychiatry. 2022;21(11):5-11. doi: 10.12788/cp.0301
2. Macpherson T, Churchland A, Sejnowski T, et al. Natural and artificial intelligence: a brief introduction to the interplay between AI and neuroscience research. Neural Netw. 2021;144:603-613.
3. Dehbouche N. Plagiarism in the age of massive Generative Pre-trained Transformers (GPT-3): “The best time to act was yesterday. The next best time is now.” Ethics Sci Environ Polit. 2021;21:17-23.
4. Turing AM. Computing machinery and intelligence. Mind. 1950;59(236):433-460.
5. McCarthy J. Artificial intelligence, logic, and formulising common sense. In: Richard H. Thomason, ed. Philosophical Logic and Artificial Intelligence. Kluwer Academic Publishing; 1989:161-190.
6. Koppe G, Meyer-Lindenberg A, Durstewitz D. Deep learning for small and big data in psychiatry. Neuropsychopharmacology. 2021;46(1):176-190.
7. Dabney W, Kurth-Nelson Z, Uchida N, et al. A distributional code for value in dopamine-based reinforcement learning. Nature. 2020;577(7792):671-675.
8. Zhou Z, Wu TC, Wang B, et al. Machine learning methods in psychiatry: a brief introduction. Gen Psychiatr. 2020;33(1):e100171.
9. Sun J, Cao R, Zhou M, et al. A hybrid deep neural network for classification of schizophrenia using EEG Data. Sci Rep. 2021;11(1):4706.
10. Kalenderian H, Nasrallah HA. Artificial intelligence in psychiatry. Current Psychiatry. 2019;18(8):33-38.
11. Ray A, Bhardwaj A, Malik YK, et al. Artificial intelligence and psychiatry: an overview. Asian J Psychiatr. 2022;70:103021.
12. Pestian E, Nasrallah HA, Matykiewicz P, et al. Suicide note classification using natural language processing: a content analysis. Biomed Inform Insights. 2010(3):19-28.
13. Chen Y, Wei Z, Gou H, et al. How far is brain-inspired artificial intelligence away from brain? Frontiers Neurosci. 2022;16:1096737.
14. Tools such as ChatGPT threaten transparent science; here are our ground rules for their use. Nature. 2023;613(7945):612. doi:10.1038/d41586-023-00191-1
We are currently on the verge of yet another societal “revolution” that will exert an unprecedented impact on our lives. It may surpass prior seismic cultural breakthroughs like the internet, smartphones, and social media. Artificial intelligence (AI) has been fermenting for several decades, gathering steam to become equivalent (and eventually superior) to human intelligence. The escalation of AI sophistication will be jarring and perhaps change human life in completely unpredictable ways.
Composing thoughts into words and coherent sentences has always been a uniquely human attribute among all living organisms. Now, that sublime feature of the human mind is being simulated, thanks to advances in AI software, ironically created by the human mind itself! On November 30, 2022, Open AI introduced ChatGPT (generative pre-trained transformer), which can generate an article on any topic a user requests. Within a few weeks, it was used by more than 100 million people. ChatGPT is taking the world by storm because it is a harbinger (some pessimists may label it an omen) of how human existence will be radically impacted in the future. Such AI breakthroughs to surpass human intelligence are, ironically, the product of the advanced human brain, which I previously described as concurrently a triumph and a blunder by evolution.1
How we got here, and what’s next
ChatGPT is a large language model based on neural networks.2 It generates realistic text responses to a wide range of questions by mimicking the pattern of language in gargantuan online databases. One Hong Kong–based, AI-powered drug discovery company (Insilico Medicine) declared it published articles generated by AI tools, even before ChatGPT became available. This indicates how AI can be misused in scientific publications and may be hard to detect as a new form of plagiarism.3
The roots of AI date back to the 1950s, when Alan Turing, now considered the father of AI, published a seminal article about creating a machine to “imitate the brain” and to “mimic the behavior of the human.”4 The term “artificial intelligence” was coined in 1989 by McCarthy,5 who defined it as “the science of engineering for making intelligent machines.” Since then, several subsets of AI have been developed:
- Machine learning: The study of computer algorithms to generate hypotheses
- Deep learning: A type of machine learning algorithm that uses multiple layers to progressively extract higher-level features from raw input. (Both machine learning and deep learning are used in the burgeoning fields of computational psychiatry6 and neuroscience research7)
- Expert knowledge system: A computer-based system that mimics human decision-making ability
- Neural networks: An interconnected group of artificial neurons that uses a math or computer model for information processing
- Predictive analytics: An algorithm to predict future outcomes based on historical data.
These subsets of AI have been used to identify psychiatric disorders using neuroimaging data8 and to classify brain disorders.9 There are many potential uses of AI in psychiatry.10,11 My first experience with AI was 13 years ago, when we conducted a project to distinguish fake suicide notes from genuine ones.12 AI was more successful in correctly identifying fake notes (78% correctly detected) than senior psychiatric residents (49%) or even faculty (53%).
AI will dramatically change how humans interact with the world and may lead to enhanced creativity and new explorations and forays into novel, previously unknown horizons. It is expected to significantly boost the global economy by many trillions of dollars over the next decade. Major high-tech companies are vigorously competing to develop their own AI tools like ChatGPT (Microsoft invested $10 billion in Open AI). Google, which owns DeepMind (an AI lab that invented the T in GPT) developed its own chatbot called Bard. Amazon has invested heavily in Stability AI by giving its founder and CEO Emad Mostaque 4,000 Nvidia AI chips to assemble the world’s largest supercomputer (1 year ago, Stability had only 32 AI chips!). Apple recently integrated Stable Diffusion into its latest operating system. Chinese tech giants Alibaba and Baidu also announced their own chatbots to be released soon.
Other competitors include Cohere, Hugging Face, Midjourney, GitHub Copilot, Game Changer, Jasper, and Anthropic, which released Claude as its chatbot at a lower cost than ChatGPT. Open AI also developed Dall-E2 in April 2022, which can generate very realistic images from text, one of which recently won an award at an art competition.
Continue to: One of the major...
One of the major concerns about these AI developments is that chatbots can make errors or disseminate misinformation and even enunciate racist or misogynist statements. The greatest worry is that the ultimate implicit goal of AI is what is called artificial general intelligence (AGI), which can think and learn better than humans. Some fear AGI may wipe out humans as a species, a grave outcome indeed. That’s why AI developers intend to align AGI with “basic human values” in the event it surpasses human intelligence. Some are even calling for a transition from AI to AW (artificial wisdom), with built-in empathy, kindness, self-reflection, acceptance of diverse perspectives, and promotion of prosocial ideas.13
Creating content: artificial intelligence vs human authors
ChatGPT has opened a Pandora’s box of concern about potential plagiarism by students or scientific authors. This has prompted several journals,14 including
- Anosognosia in schizophrenia (Box 1); based on “Is anosognosia a delusion, a negative symptom, or a cognitive deficit?”
Current Psychiatry , January 2022, p. 6-8,14. doi: 10.12788/cp.0210 - Benefits of metformin in psychiatry (Box 2); based on “Beyond diabetes: The beneficial uses of metformin in psychiatry,”
Current Psychiatry , March 2022, p. 7-9. doi: 10.12788/cp.0225 - Epidemic of intellectual constipation (Box 3); based on “From debate to stalemate and hate: An epidemic of intellectual constipation,”
Current Psychiatry , January 2023, p. 3-4. doi: 10.12788/cp.0321 - SWOT analysis of psychiatry (Box 4); based on “Contemporary psychiatry: A SWOT analysis,”
Current Psychiatry , January 2023, p. 16-19,27. doi: 10.12788/cp.0320.
These ChatGPT articles are verbatim as generated, without any copyediting, fact-checking, or addition of reference citations. One can easily notice that while factually acceptable, the ChatGPT articles tend to be rather synthetic, simple, bland, and lacking creative language or going beyond the facts to express personal viewpoints. However, I have no doubt that future versions of ChatGPT or other chatbots will evolve into far more sophisticated products and may match what a human can compose in terms of quality and complexity.
AI has arrived with a bang. Going forward, I predict it will continue to surprise us, with elements of “future shock.” The credit (or blame) belongs to the boundless creativity of human intelligence that is seeking to invent an intelligence higher than its own. Caveat emptor!
Box 1
Anosognosia is a condition in which a person is unaware or unable to recognize their own illness or disability. In schizophrenia, anosognosia can be present in up to 50% of cases and is characterized by a lack of insight into the presence and severity of symptoms.
People with anosognosia in schizophrenia may not believe that they have a mental illness, may deny the reality of their symptoms, or may attribute them to external causes. This can make it difficult for them to comply with treatment, as they may not see the need for medication or other interventions.
Anosognosia is thought to be caused by structural and functional changes in the brain, particularly in areas associated with self-awareness and insight. It is often more severe in people with more severe forms of schizophrenia and may be associated with poorer treatment outcomes.
Effective treatment for anosognosia in schizophrenia typically involves a combination of medication and therapy, as well as strategies for improving insight and awareness of symptoms. Family members and caregivers can also play an important role in helping people with schizophrenia to recognize the presence and impact of their illness, and encouraging them to engage in treatment.
a Based on “Is anosognosia a delusion, a negative symptom, or a cognitive deficit?” Current Psychiatry, January 2022, p. 6-8,14. doi: 10.12788/cp.0210
Box 2
Metformin is a medication commonly used in the treatment of type 2 diabetes. However, there is growing interest in its potential use in psychiatry, particularly in the treatment of certain mental health conditions. Some potential benefits of metformin in psychiatry include:
1. Treatment of mood disorders: Studies have suggested that metformin may be helpful in the treatment of mood disorders, such as depression and bipolar disorder. One proposed mechanism is that metformin may help to regulate glucose metabolism and insulin sensitivity, which in turn may help to stabilize mood.
2. Treatment of schizophrenia: Some studies have suggested that metformin may be helpful in reducing symptoms of schizophrenia, particularly negative symptoms such as social withdrawal and apathy. One proposed mechanism is that metformin may improve brain energy metabolism, which may in turn improve cognitive function and reduce symptoms.
3. Weight management: Metformin has been shown to be effective in weight management, which can be particularly important for people with certain mental health conditions, such as bipolar disorder, where weight gain can be a side effect of medication.
4. Neuroprotection: Metformin has been shown to have neuroprotective effects, which may be beneficial for people with certain mental health conditions, such as Alzheimer’s disease and Parkinson’s disease.
It is important to note that while there is some evidence for the potential benefits of metformin in psychiatry, further research is needed to fully understand its effectiveness and safety in this context. People with mental health conditions should not start taking metformin without first consulting with their healthcare provider.
a Based on “Beyond diabetes: The beneficial uses of metformin in psychiatry,” Current Psychiatry, March 2022, p. 7-9. doi: 10.12788/cp.0225
Box 3
The term “epidemic of intellectual constipation” refers to a phenomenon in which individuals, groups, or even entire societies are seen as lacking the ability to think critically, creatively, or expansively. It can be characterized by a lack of curiosity, a narrow range of interests, and a reluctance to engage with new or challenging ideas.
The cause of this phenomenon can be attributed to a variety of factors, including cultural, social, and educational influences. For example, some argue that a narrow and standardized educational system, as well as a lack of exposure to diverse perspectives, can limit creativity and critical thinking skills. Additionally, the prevalence of social media and other forms of digital media may encourage a focus on immediate gratification and quick information, rather than more in-depth and meaningful engagement with information.
The consequences of this epidemic can be far-reaching and can impact personal, social, and political aspects of life. For instance, a lack of critical thinking skills can lead to the spread of misinformation, while a narrow range of interests can limit personal growth and the ability to connect with others.
To combat the epidemic of intellectual constipation, it’s important to foster critical thinking skills, encourage exposure to diverse perspectives, and encourage a lifelong love of learning. This can be achieved through education, community engagement, and personal effort.
In conclusion, the “epidemic of intellectual constipation” refers to a phenomenon in which individuals, groups, or entire societies lack the ability to think critically, creatively, and expansively. To combat this epidemic, it’s important to foster critical thinking skills, encourage exposure to diverse perspectives, and encourage a lifelong love of learning.
a Based on “From debate to stalemate and hate: An epidemic of intellectual constipation,” Current Psychiatry, January 2023, p. 3-4. doi: 10.12788/cp.0321
Box 4
SWOT analysis is a tool used to assess the strengths, weaknesses, opportunities, and threats of a particular entity or industry. In this case, we will conduct a SWOT analysis of psychiatry as a field of medicine.
Strengths
• Psychiatry plays a crucial role in addressing mental health issues and improving the quality of life of individuals who struggle with them.
• Psychiatry has made significant advances in understanding the biological and psychological underpinnings of mental illness, which has led to the development of more effective treatments.
• There is growing public awareness and acceptance of the importance of mental health, which has led to increased demand for psychiatric services.
• The field of psychiatry attracts many talented and compassionate professionals who are dedicated to helping those in need.
Weaknesses
• There is still a significant stigma associated with mental illness, which can deter individuals from seeking treatment.
• The effectiveness of some psychiatric treatments can be limited, particularly in cases of severe mental illness.
• The shortage of mental health professionals in many areas means that access to psychiatric services may be limited, particularly for individuals with lower incomes.
• The cost of psychiatric treatment can be prohibitively expensive, particularly for individuals without insurance coverage.
Opportunities
• New advances in neuroscience and technology, such as brain imaging and genetic testing, hold promise for improving the accuracy of psychiatric diagnoses and developing more targeted treatments.
• Telepsychiatry and other online mental health services offer new ways to increase access to care and reach individuals in underserved areas.
• Greater collaboration with primary care physicians and other healthcare professionals could improve the integration of mental health services into routine healthcare.
• The ongoing destigmatization of mental illness could lead to greater public acceptance and support for mental health services.
Threats
• The ongoing COVID-19 pandemic has increased the prevalence of mental health issues and placed additional strain on mental health services.
• The shortage of mental health professionals, particularly in certain areas of the country, could worsen in the coming years.
• Changes in healthcare policy, such as cuts to mental health funding or changes to insurance coverage, could limit access to care.
• Misinformation and stigma surrounding mental illness could continue to deter individuals from seeking treatment.
a Based on “Contemporary psychiatry: A SWOT analysis,” Current Psychiatry, January 2023, p. 16-19,27. doi: 10.12788/cp.0320
We are currently on the verge of yet another societal “revolution” that will exert an unprecedented impact on our lives. It may surpass prior seismic cultural breakthroughs like the internet, smartphones, and social media. Artificial intelligence (AI) has been fermenting for several decades, gathering steam to become equivalent (and eventually superior) to human intelligence. The escalation of AI sophistication will be jarring and perhaps change human life in completely unpredictable ways.
Composing thoughts into words and coherent sentences has always been a uniquely human attribute among all living organisms. Now, that sublime feature of the human mind is being simulated, thanks to advances in AI software, ironically created by the human mind itself! On November 30, 2022, Open AI introduced ChatGPT (generative pre-trained transformer), which can generate an article on any topic a user requests. Within a few weeks, it was used by more than 100 million people. ChatGPT is taking the world by storm because it is a harbinger (some pessimists may label it an omen) of how human existence will be radically impacted in the future. Such AI breakthroughs to surpass human intelligence are, ironically, the product of the advanced human brain, which I previously described as concurrently a triumph and a blunder by evolution.1
How we got here, and what’s next
ChatGPT is a large language model based on neural networks.2 It generates realistic text responses to a wide range of questions by mimicking the pattern of language in gargantuan online databases. One Hong Kong–based, AI-powered drug discovery company (Insilico Medicine) declared it published articles generated by AI tools, even before ChatGPT became available. This indicates how AI can be misused in scientific publications and may be hard to detect as a new form of plagiarism.3
The roots of AI date back to the 1950s, when Alan Turing, now considered the father of AI, published a seminal article about creating a machine to “imitate the brain” and to “mimic the behavior of the human.”4 The term “artificial intelligence” was coined in 1989 by McCarthy,5 who defined it as “the science of engineering for making intelligent machines.” Since then, several subsets of AI have been developed:
- Machine learning: The study of computer algorithms to generate hypotheses
- Deep learning: A type of machine learning algorithm that uses multiple layers to progressively extract higher-level features from raw input. (Both machine learning and deep learning are used in the burgeoning fields of computational psychiatry6 and neuroscience research7)
- Expert knowledge system: A computer-based system that mimics human decision-making ability
- Neural networks: An interconnected group of artificial neurons that uses a math or computer model for information processing
- Predictive analytics: An algorithm to predict future outcomes based on historical data.
These subsets of AI have been used to identify psychiatric disorders using neuroimaging data8 and to classify brain disorders.9 There are many potential uses of AI in psychiatry.10,11 My first experience with AI was 13 years ago, when we conducted a project to distinguish fake suicide notes from genuine ones.12 AI was more successful in correctly identifying fake notes (78% correctly detected) than senior psychiatric residents (49%) or even faculty (53%).
AI will dramatically change how humans interact with the world and may lead to enhanced creativity and new explorations and forays into novel, previously unknown horizons. It is expected to significantly boost the global economy by many trillions of dollars over the next decade. Major high-tech companies are vigorously competing to develop their own AI tools like ChatGPT (Microsoft invested $10 billion in Open AI). Google, which owns DeepMind (an AI lab that invented the T in GPT) developed its own chatbot called Bard. Amazon has invested heavily in Stability AI by giving its founder and CEO Emad Mostaque 4,000 Nvidia AI chips to assemble the world’s largest supercomputer (1 year ago, Stability had only 32 AI chips!). Apple recently integrated Stable Diffusion into its latest operating system. Chinese tech giants Alibaba and Baidu also announced their own chatbots to be released soon.
Other competitors include Cohere, Hugging Face, Midjourney, GitHub Copilot, Game Changer, Jasper, and Anthropic, which released Claude as its chatbot at a lower cost than ChatGPT. Open AI also developed Dall-E2 in April 2022, which can generate very realistic images from text, one of which recently won an award at an art competition.
Continue to: One of the major...
One of the major concerns about these AI developments is that chatbots can make errors or disseminate misinformation and even enunciate racist or misogynist statements. The greatest worry is that the ultimate implicit goal of AI is what is called artificial general intelligence (AGI), which can think and learn better than humans. Some fear AGI may wipe out humans as a species, a grave outcome indeed. That’s why AI developers intend to align AGI with “basic human values” in the event it surpasses human intelligence. Some are even calling for a transition from AI to AW (artificial wisdom), with built-in empathy, kindness, self-reflection, acceptance of diverse perspectives, and promotion of prosocial ideas.13
Creating content: artificial intelligence vs human authors
ChatGPT has opened a Pandora’s box of concern about potential plagiarism by students or scientific authors. This has prompted several journals,14 including
- Anosognosia in schizophrenia (Box 1); based on “Is anosognosia a delusion, a negative symptom, or a cognitive deficit?”
Current Psychiatry , January 2022, p. 6-8,14. doi: 10.12788/cp.0210 - Benefits of metformin in psychiatry (Box 2); based on “Beyond diabetes: The beneficial uses of metformin in psychiatry,”
Current Psychiatry , March 2022, p. 7-9. doi: 10.12788/cp.0225 - Epidemic of intellectual constipation (Box 3); based on “From debate to stalemate and hate: An epidemic of intellectual constipation,”
Current Psychiatry , January 2023, p. 3-4. doi: 10.12788/cp.0321 - SWOT analysis of psychiatry (Box 4); based on “Contemporary psychiatry: A SWOT analysis,”
Current Psychiatry , January 2023, p. 16-19,27. doi: 10.12788/cp.0320.
These ChatGPT articles are verbatim as generated, without any copyediting, fact-checking, or addition of reference citations. One can easily notice that while factually acceptable, the ChatGPT articles tend to be rather synthetic, simple, bland, and lacking creative language or going beyond the facts to express personal viewpoints. However, I have no doubt that future versions of ChatGPT or other chatbots will evolve into far more sophisticated products and may match what a human can compose in terms of quality and complexity.
AI has arrived with a bang. Going forward, I predict it will continue to surprise us, with elements of “future shock.” The credit (or blame) belongs to the boundless creativity of human intelligence that is seeking to invent an intelligence higher than its own. Caveat emptor!
Box 1
Anosognosia is a condition in which a person is unaware or unable to recognize their own illness or disability. In schizophrenia, anosognosia can be present in up to 50% of cases and is characterized by a lack of insight into the presence and severity of symptoms.
People with anosognosia in schizophrenia may not believe that they have a mental illness, may deny the reality of their symptoms, or may attribute them to external causes. This can make it difficult for them to comply with treatment, as they may not see the need for medication or other interventions.
Anosognosia is thought to be caused by structural and functional changes in the brain, particularly in areas associated with self-awareness and insight. It is often more severe in people with more severe forms of schizophrenia and may be associated with poorer treatment outcomes.
Effective treatment for anosognosia in schizophrenia typically involves a combination of medication and therapy, as well as strategies for improving insight and awareness of symptoms. Family members and caregivers can also play an important role in helping people with schizophrenia to recognize the presence and impact of their illness, and encouraging them to engage in treatment.
a Based on “Is anosognosia a delusion, a negative symptom, or a cognitive deficit?” Current Psychiatry, January 2022, p. 6-8,14. doi: 10.12788/cp.0210
Box 2
Metformin is a medication commonly used in the treatment of type 2 diabetes. However, there is growing interest in its potential use in psychiatry, particularly in the treatment of certain mental health conditions. Some potential benefits of metformin in psychiatry include:
1. Treatment of mood disorders: Studies have suggested that metformin may be helpful in the treatment of mood disorders, such as depression and bipolar disorder. One proposed mechanism is that metformin may help to regulate glucose metabolism and insulin sensitivity, which in turn may help to stabilize mood.
2. Treatment of schizophrenia: Some studies have suggested that metformin may be helpful in reducing symptoms of schizophrenia, particularly negative symptoms such as social withdrawal and apathy. One proposed mechanism is that metformin may improve brain energy metabolism, which may in turn improve cognitive function and reduce symptoms.
3. Weight management: Metformin has been shown to be effective in weight management, which can be particularly important for people with certain mental health conditions, such as bipolar disorder, where weight gain can be a side effect of medication.
4. Neuroprotection: Metformin has been shown to have neuroprotective effects, which may be beneficial for people with certain mental health conditions, such as Alzheimer’s disease and Parkinson’s disease.
It is important to note that while there is some evidence for the potential benefits of metformin in psychiatry, further research is needed to fully understand its effectiveness and safety in this context. People with mental health conditions should not start taking metformin without first consulting with their healthcare provider.
a Based on “Beyond diabetes: The beneficial uses of metformin in psychiatry,” Current Psychiatry, March 2022, p. 7-9. doi: 10.12788/cp.0225
Box 3
The term “epidemic of intellectual constipation” refers to a phenomenon in which individuals, groups, or even entire societies are seen as lacking the ability to think critically, creatively, or expansively. It can be characterized by a lack of curiosity, a narrow range of interests, and a reluctance to engage with new or challenging ideas.
The cause of this phenomenon can be attributed to a variety of factors, including cultural, social, and educational influences. For example, some argue that a narrow and standardized educational system, as well as a lack of exposure to diverse perspectives, can limit creativity and critical thinking skills. Additionally, the prevalence of social media and other forms of digital media may encourage a focus on immediate gratification and quick information, rather than more in-depth and meaningful engagement with information.
The consequences of this epidemic can be far-reaching and can impact personal, social, and political aspects of life. For instance, a lack of critical thinking skills can lead to the spread of misinformation, while a narrow range of interests can limit personal growth and the ability to connect with others.
To combat the epidemic of intellectual constipation, it’s important to foster critical thinking skills, encourage exposure to diverse perspectives, and encourage a lifelong love of learning. This can be achieved through education, community engagement, and personal effort.
In conclusion, the “epidemic of intellectual constipation” refers to a phenomenon in which individuals, groups, or entire societies lack the ability to think critically, creatively, and expansively. To combat this epidemic, it’s important to foster critical thinking skills, encourage exposure to diverse perspectives, and encourage a lifelong love of learning.
a Based on “From debate to stalemate and hate: An epidemic of intellectual constipation,” Current Psychiatry, January 2023, p. 3-4. doi: 10.12788/cp.0321
Box 4
SWOT analysis is a tool used to assess the strengths, weaknesses, opportunities, and threats of a particular entity or industry. In this case, we will conduct a SWOT analysis of psychiatry as a field of medicine.
Strengths
• Psychiatry plays a crucial role in addressing mental health issues and improving the quality of life of individuals who struggle with them.
• Psychiatry has made significant advances in understanding the biological and psychological underpinnings of mental illness, which has led to the development of more effective treatments.
• There is growing public awareness and acceptance of the importance of mental health, which has led to increased demand for psychiatric services.
• The field of psychiatry attracts many talented and compassionate professionals who are dedicated to helping those in need.
Weaknesses
• There is still a significant stigma associated with mental illness, which can deter individuals from seeking treatment.
• The effectiveness of some psychiatric treatments can be limited, particularly in cases of severe mental illness.
• The shortage of mental health professionals in many areas means that access to psychiatric services may be limited, particularly for individuals with lower incomes.
• The cost of psychiatric treatment can be prohibitively expensive, particularly for individuals without insurance coverage.
Opportunities
• New advances in neuroscience and technology, such as brain imaging and genetic testing, hold promise for improving the accuracy of psychiatric diagnoses and developing more targeted treatments.
• Telepsychiatry and other online mental health services offer new ways to increase access to care and reach individuals in underserved areas.
• Greater collaboration with primary care physicians and other healthcare professionals could improve the integration of mental health services into routine healthcare.
• The ongoing destigmatization of mental illness could lead to greater public acceptance and support for mental health services.
Threats
• The ongoing COVID-19 pandemic has increased the prevalence of mental health issues and placed additional strain on mental health services.
• The shortage of mental health professionals, particularly in certain areas of the country, could worsen in the coming years.
• Changes in healthcare policy, such as cuts to mental health funding or changes to insurance coverage, could limit access to care.
• Misinformation and stigma surrounding mental illness could continue to deter individuals from seeking treatment.
a Based on “Contemporary psychiatry: A SWOT analysis,” Current Psychiatry, January 2023, p. 16-19,27. doi: 10.12788/cp.0320
1. Nasrallah HA. Is evolution’s greatest triumph its worst blunder? Current Psychiatry. 2022;21(11):5-11. doi: 10.12788/cp.0301
2. Macpherson T, Churchland A, Sejnowski T, et al. Natural and artificial intelligence: a brief introduction to the interplay between AI and neuroscience research. Neural Netw. 2021;144:603-613.
3. Dehbouche N. Plagiarism in the age of massive Generative Pre-trained Transformers (GPT-3): “The best time to act was yesterday. The next best time is now.” Ethics Sci Environ Polit. 2021;21:17-23.
4. Turing AM. Computing machinery and intelligence. Mind. 1950;59(236):433-460.
5. McCarthy J. Artificial intelligence, logic, and formulising common sense. In: Richard H. Thomason, ed. Philosophical Logic and Artificial Intelligence. Kluwer Academic Publishing; 1989:161-190.
6. Koppe G, Meyer-Lindenberg A, Durstewitz D. Deep learning for small and big data in psychiatry. Neuropsychopharmacology. 2021;46(1):176-190.
7. Dabney W, Kurth-Nelson Z, Uchida N, et al. A distributional code for value in dopamine-based reinforcement learning. Nature. 2020;577(7792):671-675.
8. Zhou Z, Wu TC, Wang B, et al. Machine learning methods in psychiatry: a brief introduction. Gen Psychiatr. 2020;33(1):e100171.
9. Sun J, Cao R, Zhou M, et al. A hybrid deep neural network for classification of schizophrenia using EEG Data. Sci Rep. 2021;11(1):4706.
10. Kalenderian H, Nasrallah HA. Artificial intelligence in psychiatry. Current Psychiatry. 2019;18(8):33-38.
11. Ray A, Bhardwaj A, Malik YK, et al. Artificial intelligence and psychiatry: an overview. Asian J Psychiatr. 2022;70:103021.
12. Pestian E, Nasrallah HA, Matykiewicz P, et al. Suicide note classification using natural language processing: a content analysis. Biomed Inform Insights. 2010(3):19-28.
13. Chen Y, Wei Z, Gou H, et al. How far is brain-inspired artificial intelligence away from brain? Frontiers Neurosci. 2022;16:1096737.
14. Tools such as ChatGPT threaten transparent science; here are our ground rules for their use. Nature. 2023;613(7945):612. doi:10.1038/d41586-023-00191-1
1. Nasrallah HA. Is evolution’s greatest triumph its worst blunder? Current Psychiatry. 2022;21(11):5-11. doi: 10.12788/cp.0301
2. Macpherson T, Churchland A, Sejnowski T, et al. Natural and artificial intelligence: a brief introduction to the interplay between AI and neuroscience research. Neural Netw. 2021;144:603-613.
3. Dehbouche N. Plagiarism in the age of massive Generative Pre-trained Transformers (GPT-3): “The best time to act was yesterday. The next best time is now.” Ethics Sci Environ Polit. 2021;21:17-23.
4. Turing AM. Computing machinery and intelligence. Mind. 1950;59(236):433-460.
5. McCarthy J. Artificial intelligence, logic, and formulising common sense. In: Richard H. Thomason, ed. Philosophical Logic and Artificial Intelligence. Kluwer Academic Publishing; 1989:161-190.
6. Koppe G, Meyer-Lindenberg A, Durstewitz D. Deep learning for small and big data in psychiatry. Neuropsychopharmacology. 2021;46(1):176-190.
7. Dabney W, Kurth-Nelson Z, Uchida N, et al. A distributional code for value in dopamine-based reinforcement learning. Nature. 2020;577(7792):671-675.
8. Zhou Z, Wu TC, Wang B, et al. Machine learning methods in psychiatry: a brief introduction. Gen Psychiatr. 2020;33(1):e100171.
9. Sun J, Cao R, Zhou M, et al. A hybrid deep neural network for classification of schizophrenia using EEG Data. Sci Rep. 2021;11(1):4706.
10. Kalenderian H, Nasrallah HA. Artificial intelligence in psychiatry. Current Psychiatry. 2019;18(8):33-38.
11. Ray A, Bhardwaj A, Malik YK, et al. Artificial intelligence and psychiatry: an overview. Asian J Psychiatr. 2022;70:103021.
12. Pestian E, Nasrallah HA, Matykiewicz P, et al. Suicide note classification using natural language processing: a content analysis. Biomed Inform Insights. 2010(3):19-28.
13. Chen Y, Wei Z, Gou H, et al. How far is brain-inspired artificial intelligence away from brain? Frontiers Neurosci. 2022;16:1096737.
14. Tools such as ChatGPT threaten transparent science; here are our ground rules for their use. Nature. 2023;613(7945):612. doi:10.1038/d41586-023-00191-1

A ‘guest editorial’ … generated by ChatGPT?
The artificial intelligence (AI) program ChatGPT (generative pre-trained transformer) was introduced to the public by Open AI on November 30, 2022. It has been described as a game-changer for society, culture, literature, arts, and science, with a potential impact that rivals that of the internet and social media.
ChatGPT can produce human-like essays in response to queries. Some researchers used ChatGPT to generate abstracts based on the titles of articles published in 5 high-impact journals. These abstracts were so “real” that they escaped detection by expert peer reviewers in 32% of cases.1 In addition, several medical/science articles were published that included ChatGPT as a bylined author.2
Like other journals,3-7
- Nonhuman AI technologies do not qualify for named authorship.
- Authors should be transparent about the use of AI technologies to aid in writing content. Authors should disclose which tool was used and how it was applied in the article submitted to the journal.
- Human authors are responsible for the accuracy of work compiled by an AI tool, including the absence of plagiarism. Proper referencing of statements is necessary.
- Images created by AI tools are not permitted for publication.
Because the overwhelming majority of articles published in
Can AI generate an acceptable ‘guest editorial?’
In addition to creating formulaic writing, some of the concerns about using AI in scientific publishing is that the results might be outdated, incorrect, or lacking appropriate references, and that it can produce “plausible-sounding but incorrect or nonsensical” answers to questions.3 To test this, I asked ChatGPT to write an article on the same topic as 4 of my articles published in
Box
There are many myths and misconceptions surrounding psychiatry, the branch of medicine that deals with the diagnosis, treatment, and prevention of mental illness. Some of the most common myths include:
1. Psychiatry is not a real medical specialty: This is a false myth. Psychiatry is a recognized medical specialty, and psychiatrists are licensed medical doctors who have undergone extensive training in the diagnosis and treatment of mental illness.
2. Mental illness is not a real illness: Mental illness is a real and biologically based medical condition, just like physical illness. Research has shown that mental illness is caused by a combination of genetic, environmental, and lifestyle factors.
3. Antidepressants are not effective: Antidepressants have been shown to be effective in treating depression and other mental illnesses. While they are not a cure, they can provide significant symptom relief and improve quality of life for many people.
4. Psychiatric drugs are dangerous and have serious side effects: While all drugs have potential side effects, psychiatric medications have been proven to be safe and effective for many people. The risks and benefits of taking any medication should be carefully considered and discussed with a healthcare professional.
5. Therapy is not effective: Therapy, also known as psychotherapy, has been shown to be effective in treating a wide range of mental illnesses, including depression, anxiety, and post-traumatic stress disorder (PTSD).
6. People with mental illness are violent: People with mental illness are no more likely to be violent than the general population. In fact, people with mental illness are more likely to be victims of violence than perpetrators.
It is important to dispel these myths and misconceptions about psychiatry, as they can prevent people from seeking the help they need and can also contribute to stigma and discrimination towards those with mental illness.
In conclusion, there are many myths and misconceptions surrounding psychiatry. Dispelling these myths and increasing public understanding about mental illness and its treatment can help reduce stigma and encourage more people to seek the help they need.
What do you think? I encourage you to send me your take on this AI-generated “guest editorial,” and whether you deem its quality to be similar to that of an article authored by a human psychiatrist.
1. Else H. Abstracts written by ChatGPT fool scientists. Nature. 2023;613(7944):423. doi: 10.1038/d41586-023-00056-7
2. Stokel-Walker C. ChatGPT listed as author on research papers: many scientists disapprove. Nature. 2023;613(7945):620-621. doi:10.1038/d41586-023-00107-z
3. Flanagin A, Bibbins-Domingo K, Berkwits M, et al. Nonhuman “authors” and implications for the integrity of scientific publication and medical knowledge. JAMA. 2023;329(8):637-639. doi:10.1001/jama.2023.1344
4. Tools such as ChatGPT threaten transparent science; here are our ground rules for their use. Nature. 2023;613(7945):612. doi:10.1038/d41586-023-00191-1
5. Thorp HH. ChatGPT is fun, but not an author. Science. 2023;379(6630):313. doi:10.1126/science.adg7879
6. PNAS. The PNAS journals outline their policies for ChatGPT and generative AI. February 21, 2023. Accessed March 9, 2023. https://www.pnas.org/post/update/pnas-policy-for-chatgpt-generative-ai
7. Marušic’ A. JoGH policy on the use of artificial intelligence in scholarly manuscripts. J Glob Health. 2023;13:01002. doi:10.7189/jogh.13.01002
The artificial intelligence (AI) program ChatGPT (generative pre-trained transformer) was introduced to the public by Open AI on November 30, 2022. It has been described as a game-changer for society, culture, literature, arts, and science, with a potential impact that rivals that of the internet and social media.
ChatGPT can produce human-like essays in response to queries. Some researchers used ChatGPT to generate abstracts based on the titles of articles published in 5 high-impact journals. These abstracts were so “real” that they escaped detection by expert peer reviewers in 32% of cases.1 In addition, several medical/science articles were published that included ChatGPT as a bylined author.2
Like other journals,3-7
- Nonhuman AI technologies do not qualify for named authorship.
- Authors should be transparent about the use of AI technologies to aid in writing content. Authors should disclose which tool was used and how it was applied in the article submitted to the journal.
- Human authors are responsible for the accuracy of work compiled by an AI tool, including the absence of plagiarism. Proper referencing of statements is necessary.
- Images created by AI tools are not permitted for publication.
Because the overwhelming majority of articles published in
Can AI generate an acceptable ‘guest editorial?’
In addition to creating formulaic writing, some of the concerns about using AI in scientific publishing is that the results might be outdated, incorrect, or lacking appropriate references, and that it can produce “plausible-sounding but incorrect or nonsensical” answers to questions.3 To test this, I asked ChatGPT to write an article on the same topic as 4 of my articles published in
Box
There are many myths and misconceptions surrounding psychiatry, the branch of medicine that deals with the diagnosis, treatment, and prevention of mental illness. Some of the most common myths include:
1. Psychiatry is not a real medical specialty: This is a false myth. Psychiatry is a recognized medical specialty, and psychiatrists are licensed medical doctors who have undergone extensive training in the diagnosis and treatment of mental illness.
2. Mental illness is not a real illness: Mental illness is a real and biologically based medical condition, just like physical illness. Research has shown that mental illness is caused by a combination of genetic, environmental, and lifestyle factors.
3. Antidepressants are not effective: Antidepressants have been shown to be effective in treating depression and other mental illnesses. While they are not a cure, they can provide significant symptom relief and improve quality of life for many people.
4. Psychiatric drugs are dangerous and have serious side effects: While all drugs have potential side effects, psychiatric medications have been proven to be safe and effective for many people. The risks and benefits of taking any medication should be carefully considered and discussed with a healthcare professional.
5. Therapy is not effective: Therapy, also known as psychotherapy, has been shown to be effective in treating a wide range of mental illnesses, including depression, anxiety, and post-traumatic stress disorder (PTSD).
6. People with mental illness are violent: People with mental illness are no more likely to be violent than the general population. In fact, people with mental illness are more likely to be victims of violence than perpetrators.
It is important to dispel these myths and misconceptions about psychiatry, as they can prevent people from seeking the help they need and can also contribute to stigma and discrimination towards those with mental illness.
In conclusion, there are many myths and misconceptions surrounding psychiatry. Dispelling these myths and increasing public understanding about mental illness and its treatment can help reduce stigma and encourage more people to seek the help they need.
What do you think? I encourage you to send me your take on this AI-generated “guest editorial,” and whether you deem its quality to be similar to that of an article authored by a human psychiatrist.
The artificial intelligence (AI) program ChatGPT (generative pre-trained transformer) was introduced to the public by Open AI on November 30, 2022. It has been described as a game-changer for society, culture, literature, arts, and science, with a potential impact that rivals that of the internet and social media.
ChatGPT can produce human-like essays in response to queries. Some researchers used ChatGPT to generate abstracts based on the titles of articles published in 5 high-impact journals. These abstracts were so “real” that they escaped detection by expert peer reviewers in 32% of cases.1 In addition, several medical/science articles were published that included ChatGPT as a bylined author.2
Like other journals,3-7
- Nonhuman AI technologies do not qualify for named authorship.
- Authors should be transparent about the use of AI technologies to aid in writing content. Authors should disclose which tool was used and how it was applied in the article submitted to the journal.
- Human authors are responsible for the accuracy of work compiled by an AI tool, including the absence of plagiarism. Proper referencing of statements is necessary.
- Images created by AI tools are not permitted for publication.
Because the overwhelming majority of articles published in
Can AI generate an acceptable ‘guest editorial?’
In addition to creating formulaic writing, some of the concerns about using AI in scientific publishing is that the results might be outdated, incorrect, or lacking appropriate references, and that it can produce “plausible-sounding but incorrect or nonsensical” answers to questions.3 To test this, I asked ChatGPT to write an article on the same topic as 4 of my articles published in
Box
There are many myths and misconceptions surrounding psychiatry, the branch of medicine that deals with the diagnosis, treatment, and prevention of mental illness. Some of the most common myths include:
1. Psychiatry is not a real medical specialty: This is a false myth. Psychiatry is a recognized medical specialty, and psychiatrists are licensed medical doctors who have undergone extensive training in the diagnosis and treatment of mental illness.
2. Mental illness is not a real illness: Mental illness is a real and biologically based medical condition, just like physical illness. Research has shown that mental illness is caused by a combination of genetic, environmental, and lifestyle factors.
3. Antidepressants are not effective: Antidepressants have been shown to be effective in treating depression and other mental illnesses. While they are not a cure, they can provide significant symptom relief and improve quality of life for many people.
4. Psychiatric drugs are dangerous and have serious side effects: While all drugs have potential side effects, psychiatric medications have been proven to be safe and effective for many people. The risks and benefits of taking any medication should be carefully considered and discussed with a healthcare professional.
5. Therapy is not effective: Therapy, also known as psychotherapy, has been shown to be effective in treating a wide range of mental illnesses, including depression, anxiety, and post-traumatic stress disorder (PTSD).
6. People with mental illness are violent: People with mental illness are no more likely to be violent than the general population. In fact, people with mental illness are more likely to be victims of violence than perpetrators.
It is important to dispel these myths and misconceptions about psychiatry, as they can prevent people from seeking the help they need and can also contribute to stigma and discrimination towards those with mental illness.
In conclusion, there are many myths and misconceptions surrounding psychiatry. Dispelling these myths and increasing public understanding about mental illness and its treatment can help reduce stigma and encourage more people to seek the help they need.
What do you think? I encourage you to send me your take on this AI-generated “guest editorial,” and whether you deem its quality to be similar to that of an article authored by a human psychiatrist.
1. Else H. Abstracts written by ChatGPT fool scientists. Nature. 2023;613(7944):423. doi: 10.1038/d41586-023-00056-7
2. Stokel-Walker C. ChatGPT listed as author on research papers: many scientists disapprove. Nature. 2023;613(7945):620-621. doi:10.1038/d41586-023-00107-z
3. Flanagin A, Bibbins-Domingo K, Berkwits M, et al. Nonhuman “authors” and implications for the integrity of scientific publication and medical knowledge. JAMA. 2023;329(8):637-639. doi:10.1001/jama.2023.1344
4. Tools such as ChatGPT threaten transparent science; here are our ground rules for their use. Nature. 2023;613(7945):612. doi:10.1038/d41586-023-00191-1
5. Thorp HH. ChatGPT is fun, but not an author. Science. 2023;379(6630):313. doi:10.1126/science.adg7879
6. PNAS. The PNAS journals outline their policies for ChatGPT and generative AI. February 21, 2023. Accessed March 9, 2023. https://www.pnas.org/post/update/pnas-policy-for-chatgpt-generative-ai
7. Marušic’ A. JoGH policy on the use of artificial intelligence in scholarly manuscripts. J Glob Health. 2023;13:01002. doi:10.7189/jogh.13.01002
1. Else H. Abstracts written by ChatGPT fool scientists. Nature. 2023;613(7944):423. doi: 10.1038/d41586-023-00056-7
2. Stokel-Walker C. ChatGPT listed as author on research papers: many scientists disapprove. Nature. 2023;613(7945):620-621. doi:10.1038/d41586-023-00107-z
3. Flanagin A, Bibbins-Domingo K, Berkwits M, et al. Nonhuman “authors” and implications for the integrity of scientific publication and medical knowledge. JAMA. 2023;329(8):637-639. doi:10.1001/jama.2023.1344
4. Tools such as ChatGPT threaten transparent science; here are our ground rules for their use. Nature. 2023;613(7945):612. doi:10.1038/d41586-023-00191-1
5. Thorp HH. ChatGPT is fun, but not an author. Science. 2023;379(6630):313. doi:10.1126/science.adg7879
6. PNAS. The PNAS journals outline their policies for ChatGPT and generative AI. February 21, 2023. Accessed March 9, 2023. https://www.pnas.org/post/update/pnas-policy-for-chatgpt-generative-ai
7. Marušic’ A. JoGH policy on the use of artificial intelligence in scholarly manuscripts. J Glob Health. 2023;13:01002. doi:10.7189/jogh.13.01002

More on SWOT analysis, more
I enjoyed reading the optimistic outlook for psychiatry outlined in your SWOT analysis (“Contemporary psychiatry: A SWOT analysis,”
I think, though, you misplaced an opportunity as a threat in your assessment that the increase in the amount of advanced practice psychiatric nurses (PMHAPRNs) presents a threat to psychiatry. The presence of an increased number of PMHAPRNs provides access to a larger number of people needing treatment by qualified, skilled mental health professionals and an opportunity for psychiatrists to participate in highly effective teams of psychiatric clinicians. This workforce-building is of particular importance during our current clinician shortage, especially within psychiatry. Most research has shown that advanced practice nurses’ quality of care is competitive with that of physicians with similar experience, and that patient satisfaction is high. Advanced practice nurses are more likely than physicians to provide care in underserved populations and in rural communities. We are educated to practice independently within our scope, to standards established by our professional organizations as well as American Psychiatric Association (APA) clinical guidelines. I hope you will reconsider your view of your PMHAPRN colleagues as a threat and see them as a positive contribution to your chosen field of psychiatry, like the APA has shown in their choice of including a PMHAPRN as a clinical expert team member on the SMI Adviser initiative.
Stella Logan, APRN, PMHCNS-BC, PMHNP-BC
Austin, Texas
Dr. Nasrallah responds
Thank you for your letter regarding my SWOT article. It was originally written for the newsletter of the Ohio Psychiatric Physicians Association, comprised of 1,000 psychiatrists. To them, nurse practitioners (NPs) are regarded as a threat because some mental health care systems have been laying off psychiatrists and hiring NPs to lower costs. This obviously is perceived as a threat. I do agree with you that well-qualified NPs are providing needed mental health services in underserved areas (eg, inner cities and rural areas), where it is very difficult to recruit psychiatrists due to the severe shortage nationally.
Henry A. Nasrallah, MD, DLFAPA
Editor-in-Chief
Continue to: More on the transdiagnostic model
More on the transdiagnostic model
I just had the pleasure of reading your February 2023 editorial (“Depression and schizophrenia: Many biological and clinical similarities,”
David Krassner, MD
Phoenix, Arizona
I completely agree with your promotion of a unified transdiagnostic model. All of this makes sense on the continuum of consciousness—restricted consciousness represents fear, whereas wide consciousness represents complete connectivity (love in the spiritual sense). Therefore, a threat not resolved can lead to defeat and an unresolved painful defeat can lead to a psychotic projection. Is it no surprise, then, that a medication such as quetiapine can treat the whole continuum from anxiety at low doses to psychosis at high doses?
Mike Primc, MD
Chardon, Ohio
I enjoyed reading the optimistic outlook for psychiatry outlined in your SWOT analysis (“Contemporary psychiatry: A SWOT analysis,”
I think, though, you misplaced an opportunity as a threat in your assessment that the increase in the amount of advanced practice psychiatric nurses (PMHAPRNs) presents a threat to psychiatry. The presence of an increased number of PMHAPRNs provides access to a larger number of people needing treatment by qualified, skilled mental health professionals and an opportunity for psychiatrists to participate in highly effective teams of psychiatric clinicians. This workforce-building is of particular importance during our current clinician shortage, especially within psychiatry. Most research has shown that advanced practice nurses’ quality of care is competitive with that of physicians with similar experience, and that patient satisfaction is high. Advanced practice nurses are more likely than physicians to provide care in underserved populations and in rural communities. We are educated to practice independently within our scope, to standards established by our professional organizations as well as American Psychiatric Association (APA) clinical guidelines. I hope you will reconsider your view of your PMHAPRN colleagues as a threat and see them as a positive contribution to your chosen field of psychiatry, like the APA has shown in their choice of including a PMHAPRN as a clinical expert team member on the SMI Adviser initiative.
Stella Logan, APRN, PMHCNS-BC, PMHNP-BC
Austin, Texas
Dr. Nasrallah responds
Thank you for your letter regarding my SWOT article. It was originally written for the newsletter of the Ohio Psychiatric Physicians Association, comprised of 1,000 psychiatrists. To them, nurse practitioners (NPs) are regarded as a threat because some mental health care systems have been laying off psychiatrists and hiring NPs to lower costs. This obviously is perceived as a threat. I do agree with you that well-qualified NPs are providing needed mental health services in underserved areas (eg, inner cities and rural areas), where it is very difficult to recruit psychiatrists due to the severe shortage nationally.
Henry A. Nasrallah, MD, DLFAPA
Editor-in-Chief
Continue to: More on the transdiagnostic model
More on the transdiagnostic model
I just had the pleasure of reading your February 2023 editorial (“Depression and schizophrenia: Many biological and clinical similarities,”
David Krassner, MD
Phoenix, Arizona
I completely agree with your promotion of a unified transdiagnostic model. All of this makes sense on the continuum of consciousness—restricted consciousness represents fear, whereas wide consciousness represents complete connectivity (love in the spiritual sense). Therefore, a threat not resolved can lead to defeat and an unresolved painful defeat can lead to a psychotic projection. Is it no surprise, then, that a medication such as quetiapine can treat the whole continuum from anxiety at low doses to psychosis at high doses?
Mike Primc, MD
Chardon, Ohio
I enjoyed reading the optimistic outlook for psychiatry outlined in your SWOT analysis (“Contemporary psychiatry: A SWOT analysis,”
I think, though, you misplaced an opportunity as a threat in your assessment that the increase in the amount of advanced practice psychiatric nurses (PMHAPRNs) presents a threat to psychiatry. The presence of an increased number of PMHAPRNs provides access to a larger number of people needing treatment by qualified, skilled mental health professionals and an opportunity for psychiatrists to participate in highly effective teams of psychiatric clinicians. This workforce-building is of particular importance during our current clinician shortage, especially within psychiatry. Most research has shown that advanced practice nurses’ quality of care is competitive with that of physicians with similar experience, and that patient satisfaction is high. Advanced practice nurses are more likely than physicians to provide care in underserved populations and in rural communities. We are educated to practice independently within our scope, to standards established by our professional organizations as well as American Psychiatric Association (APA) clinical guidelines. I hope you will reconsider your view of your PMHAPRN colleagues as a threat and see them as a positive contribution to your chosen field of psychiatry, like the APA has shown in their choice of including a PMHAPRN as a clinical expert team member on the SMI Adviser initiative.
Stella Logan, APRN, PMHCNS-BC, PMHNP-BC
Austin, Texas
Dr. Nasrallah responds
Thank you for your letter regarding my SWOT article. It was originally written for the newsletter of the Ohio Psychiatric Physicians Association, comprised of 1,000 psychiatrists. To them, nurse practitioners (NPs) are regarded as a threat because some mental health care systems have been laying off psychiatrists and hiring NPs to lower costs. This obviously is perceived as a threat. I do agree with you that well-qualified NPs are providing needed mental health services in underserved areas (eg, inner cities and rural areas), where it is very difficult to recruit psychiatrists due to the severe shortage nationally.
Henry A. Nasrallah, MD, DLFAPA
Editor-in-Chief
Continue to: More on the transdiagnostic model
More on the transdiagnostic model
I just had the pleasure of reading your February 2023 editorial (“Depression and schizophrenia: Many biological and clinical similarities,”
David Krassner, MD
Phoenix, Arizona
I completely agree with your promotion of a unified transdiagnostic model. All of this makes sense on the continuum of consciousness—restricted consciousness represents fear, whereas wide consciousness represents complete connectivity (love in the spiritual sense). Therefore, a threat not resolved can lead to defeat and an unresolved painful defeat can lead to a psychotic projection. Is it no surprise, then, that a medication such as quetiapine can treat the whole continuum from anxiety at low doses to psychosis at high doses?
Mike Primc, MD
Chardon, Ohio

Implicit bias in medicine and beyond
Recently, I reported to the Washtenaw County Circuit Courthouse in Ann Arbor, Mich., to fulfill my civic responsibility of jury duty. After check-in, a pool of 250 potential jurors were shown a video about implicit bias and shuttled off to different courtrooms for the jury selection process (voir dire, or “to speak the truth” in French). While not personally called up to the juror box on this day, I did have the opportunity to observe the attorneys and judge as they questioned potential jurors to uncover any indication that they might not be fair or impartial in judging the facts of this criminal case. After over 3 hours of questioning and several peremptory challenges, a jury was empaneled, and the rest of us were dismissed for the day.
In the legal system, implicit bias can adversely affect legal outcomes by impacting the beliefs and attitudes of multiple stakeholders, including attorneys and judges, litigants, witnesses, and of course jurors, threatening one of our society’s most fundamental principles of equal justice under the law. In the health care arena, implicit bias has been shown to impact patient-clinician communication and contribute to racial and ethnic disparities in patient outcomes. As a medical community, acknowledging and accepting the existence of implicit bias, its manifestations, and its impact is a critical first step to ensuring that every patient that walks into our exam rooms receives equitable care, and we can begin to move the needle in addressing persistent health disparities in patients with gastrointestinal diseases and beyond. While this is regrettably a politically charged topic in our current environment, I urge you to join me in reflecting on whether and how unconscious attitudes or stereotypes may unintentionally color the way in which you interact with patients in the clinic and serve to create or perpetuate inequities in treatment. (I also urge you to show up for jury duty!)
Turning to our April issue, we highlight two recent studies from AGA’s flagship journals, one showing an unexpected rise in pancreatic cancer incidence among women under the age of 55, and another evaluating survival outcomes by fibrosis stage in biopsy-proven nonalcoholic fatty liver disease. In this month’s Member Spotlight column, we introduce you to gastroenterologist Daniel Leffler, MD, who shares his experiences transitioning from a traditional academic career to a job in industry to further scientific advancements in celiac disease treatment. We hope you enjoy these articles and all the content included in our April issue!
Megan A. Adams, MD, JD, MSc
Recently, I reported to the Washtenaw County Circuit Courthouse in Ann Arbor, Mich., to fulfill my civic responsibility of jury duty. After check-in, a pool of 250 potential jurors were shown a video about implicit bias and shuttled off to different courtrooms for the jury selection process (voir dire, or “to speak the truth” in French). While not personally called up to the juror box on this day, I did have the opportunity to observe the attorneys and judge as they questioned potential jurors to uncover any indication that they might not be fair or impartial in judging the facts of this criminal case. After over 3 hours of questioning and several peremptory challenges, a jury was empaneled, and the rest of us were dismissed for the day.
In the legal system, implicit bias can adversely affect legal outcomes by impacting the beliefs and attitudes of multiple stakeholders, including attorneys and judges, litigants, witnesses, and of course jurors, threatening one of our society’s most fundamental principles of equal justice under the law. In the health care arena, implicit bias has been shown to impact patient-clinician communication and contribute to racial and ethnic disparities in patient outcomes. As a medical community, acknowledging and accepting the existence of implicit bias, its manifestations, and its impact is a critical first step to ensuring that every patient that walks into our exam rooms receives equitable care, and we can begin to move the needle in addressing persistent health disparities in patients with gastrointestinal diseases and beyond. While this is regrettably a politically charged topic in our current environment, I urge you to join me in reflecting on whether and how unconscious attitudes or stereotypes may unintentionally color the way in which you interact with patients in the clinic and serve to create or perpetuate inequities in treatment. (I also urge you to show up for jury duty!)
Turning to our April issue, we highlight two recent studies from AGA’s flagship journals, one showing an unexpected rise in pancreatic cancer incidence among women under the age of 55, and another evaluating survival outcomes by fibrosis stage in biopsy-proven nonalcoholic fatty liver disease. In this month’s Member Spotlight column, we introduce you to gastroenterologist Daniel Leffler, MD, who shares his experiences transitioning from a traditional academic career to a job in industry to further scientific advancements in celiac disease treatment. We hope you enjoy these articles and all the content included in our April issue!
Megan A. Adams, MD, JD, MSc
Recently, I reported to the Washtenaw County Circuit Courthouse in Ann Arbor, Mich., to fulfill my civic responsibility of jury duty. After check-in, a pool of 250 potential jurors were shown a video about implicit bias and shuttled off to different courtrooms for the jury selection process (voir dire, or “to speak the truth” in French). While not personally called up to the juror box on this day, I did have the opportunity to observe the attorneys and judge as they questioned potential jurors to uncover any indication that they might not be fair or impartial in judging the facts of this criminal case. After over 3 hours of questioning and several peremptory challenges, a jury was empaneled, and the rest of us were dismissed for the day.
In the legal system, implicit bias can adversely affect legal outcomes by impacting the beliefs and attitudes of multiple stakeholders, including attorneys and judges, litigants, witnesses, and of course jurors, threatening one of our society’s most fundamental principles of equal justice under the law. In the health care arena, implicit bias has been shown to impact patient-clinician communication and contribute to racial and ethnic disparities in patient outcomes. As a medical community, acknowledging and accepting the existence of implicit bias, its manifestations, and its impact is a critical first step to ensuring that every patient that walks into our exam rooms receives equitable care, and we can begin to move the needle in addressing persistent health disparities in patients with gastrointestinal diseases and beyond. While this is regrettably a politically charged topic in our current environment, I urge you to join me in reflecting on whether and how unconscious attitudes or stereotypes may unintentionally color the way in which you interact with patients in the clinic and serve to create or perpetuate inequities in treatment. (I also urge you to show up for jury duty!)
Turning to our April issue, we highlight two recent studies from AGA’s flagship journals, one showing an unexpected rise in pancreatic cancer incidence among women under the age of 55, and another evaluating survival outcomes by fibrosis stage in biopsy-proven nonalcoholic fatty liver disease. In this month’s Member Spotlight column, we introduce you to gastroenterologist Daniel Leffler, MD, who shares his experiences transitioning from a traditional academic career to a job in industry to further scientific advancements in celiac disease treatment. We hope you enjoy these articles and all the content included in our April issue!
Megan A. Adams, MD, JD, MSc
Are parents infecting their children with contagious negativity?
A couple of weeks ago I stumbled across a report of a Pew Research Center’s survey titled “Parenting in America today” (Pew Research Center. Jan. 24, 2023), which found that 40% of parents in the United States with children younger than 18 are “extremely or very worried” that at some point their children might struggle with anxiety or depression. Thirty-six percent replied that they were “somewhat” worried. This total of more than 75% represents a significant change from the 2015 Pew Center survey in which only 54% of parents were “somewhat” worried about their children’s mental health.
Prompted by these findings I began work on a column in which I planned to encourage pediatricians to think more like family physicians when we were working with children who were experiencing serious mental health problems. My primary message was going to be that we should turn more of our attention to the mental health of the anxious parents who must endure the often long and frustrating path toward effective psychiatric care for their children. This might come in the form of some simple suggestions about nonpharmacologic self-help strategies. Or, it could mean encouraging parents to seek psychiatric care or counseling for themselves as they wait for help for their child.

However, as I began that column, my thoughts kept drifting toward a broader consideration of the relationship between parents and pediatric mental health. If mental health of children is causing their parents to be anxious and depressed isn’t it just as likely that this is a bidirectional connection? This was not exactly an “aha” moment for me because it is a relationship I have considered for sometime. However, it is a concept that I have come to realize is receiving far too little attention.
There are exceptions. For example, a recent opinion piece in the New York Times by David French, “What if Kids Are Sad and Stressed Because Their Parents Are?” (March 19, 2023) echoes many of my concerns. Drawing on his experiences traveling around college campuses, Mr. French observes, “Just as parents are upset about their children’s anxiety and depression, children are anxious about their parent’s mental health.”
He notes that an August 2022 NBC News poll found that 58% of registered voters feel this country’s best days are behind it and joins me in imagining that this negative mind set is filtering down to the pediatric population. He acknowledges that there are other likely contributors to teen unhappiness including the ubiquity of smart phones, the secularization of society, and the media’s focus on the political divide. However, Mr. French wonders if the parenting style that results in childhood experiences that are dominated by adult supervision and protection may also be playing a large role.
In his conclusion, Mr. French asks us to consider “How much fear and anxiety should we import to our lives and homes?” as we adults search for an answer.
As I continued to drill down for other possible solutions, I encountered an avenue of psychological research that suggests that instead of, or in addition to, filtering out the anxiety-generating deluge of information, we begin to give some thought to how our beliefs may be coloring our perception of reality.
Jeremy D.W. Clifton, PhD, a psychologist at the University of Pennsylvania Positive Psychology Center has done extensive research on the relationship between our basic beliefs about the world (known as primal beliefs or simply primals in psychologist lingo) and how we interpret reality. For example, one of your primal beliefs may be that the world is a dangerous place. I, on the other hand, may see the world as a stimulating environment offering me endless opportunities to explore. I may see the world as an abundant resource limited only by my creativity. You, however, see it as a barren wasteland.
Dr. Clifton’s research has shown that our primals (at least those of adults) are relatively immutable through one’s lifetime and “do not appear to be the consequence of our experiences.” For example, living in a ZIP code with a high crime rate does not predict that you will see the world as a dangerous place. Nor does being affluent guarantee that an adult sees the world rich with opportunities.
It is unclear exactly when and by what process we develop our primal beliefs, but it is safe to say our parents probably play a large role. Exactly to what degree the tsunami of bad news we are allowing to inundate our children’s lives plays a role is unclear. However, it is reasonable to assume that news about climate change, school shootings, and the pandemic must be a contributor.
According to Dr. Clifton, there is some evidence that certain mind exercises, when applied diligently, can occasionally modify the primal beliefs of an individual who sees the world as dangerous and barren. Until such strategies become more readily accessible, the best we can do is acknowledge that our children are like canaries in a coal mine full of negative perceptions, then do our best to clear the air.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
A couple of weeks ago I stumbled across a report of a Pew Research Center’s survey titled “Parenting in America today” (Pew Research Center. Jan. 24, 2023), which found that 40% of parents in the United States with children younger than 18 are “extremely or very worried” that at some point their children might struggle with anxiety or depression. Thirty-six percent replied that they were “somewhat” worried. This total of more than 75% represents a significant change from the 2015 Pew Center survey in which only 54% of parents were “somewhat” worried about their children’s mental health.
Prompted by these findings I began work on a column in which I planned to encourage pediatricians to think more like family physicians when we were working with children who were experiencing serious mental health problems. My primary message was going to be that we should turn more of our attention to the mental health of the anxious parents who must endure the often long and frustrating path toward effective psychiatric care for their children. This might come in the form of some simple suggestions about nonpharmacologic self-help strategies. Or, it could mean encouraging parents to seek psychiatric care or counseling for themselves as they wait for help for their child.
However, as I began that column, my thoughts kept drifting toward a broader consideration of the relationship between parents and pediatric mental health. If mental health of children is causing their parents to be anxious and depressed isn’t it just as likely that this is a bidirectional connection? This was not exactly an “aha” moment for me because it is a relationship I have considered for sometime. However, it is a concept that I have come to realize is receiving far too little attention.
There are exceptions. For example, a recent opinion piece in the New York Times by David French, “What if Kids Are Sad and Stressed Because Their Parents Are?” (March 19, 2023) echoes many of my concerns. Drawing on his experiences traveling around college campuses, Mr. French observes, “Just as parents are upset about their children’s anxiety and depression, children are anxious about their parent’s mental health.”
He notes that an August 2022 NBC News poll found that 58% of registered voters feel this country’s best days are behind it and joins me in imagining that this negative mind set is filtering down to the pediatric population. He acknowledges that there are other likely contributors to teen unhappiness including the ubiquity of smart phones, the secularization of society, and the media’s focus on the political divide. However, Mr. French wonders if the parenting style that results in childhood experiences that are dominated by adult supervision and protection may also be playing a large role.
In his conclusion, Mr. French asks us to consider “How much fear and anxiety should we import to our lives and homes?” as we adults search for an answer.
As I continued to drill down for other possible solutions, I encountered an avenue of psychological research that suggests that instead of, or in addition to, filtering out the anxiety-generating deluge of information, we begin to give some thought to how our beliefs may be coloring our perception of reality.
Jeremy D.W. Clifton, PhD, a psychologist at the University of Pennsylvania Positive Psychology Center has done extensive research on the relationship between our basic beliefs about the world (known as primal beliefs or simply primals in psychologist lingo) and how we interpret reality. For example, one of your primal beliefs may be that the world is a dangerous place. I, on the other hand, may see the world as a stimulating environment offering me endless opportunities to explore. I may see the world as an abundant resource limited only by my creativity. You, however, see it as a barren wasteland.
Dr. Clifton’s research has shown that our primals (at least those of adults) are relatively immutable through one’s lifetime and “do not appear to be the consequence of our experiences.” For example, living in a ZIP code with a high crime rate does not predict that you will see the world as a dangerous place. Nor does being affluent guarantee that an adult sees the world rich with opportunities.
It is unclear exactly when and by what process we develop our primal beliefs, but it is safe to say our parents probably play a large role. Exactly to what degree the tsunami of bad news we are allowing to inundate our children’s lives plays a role is unclear. However, it is reasonable to assume that news about climate change, school shootings, and the pandemic must be a contributor.
According to Dr. Clifton, there is some evidence that certain mind exercises, when applied diligently, can occasionally modify the primal beliefs of an individual who sees the world as dangerous and barren. Until such strategies become more readily accessible, the best we can do is acknowledge that our children are like canaries in a coal mine full of negative perceptions, then do our best to clear the air.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
A couple of weeks ago I stumbled across a report of a Pew Research Center’s survey titled “Parenting in America today” (Pew Research Center. Jan. 24, 2023), which found that 40% of parents in the United States with children younger than 18 are “extremely or very worried” that at some point their children might struggle with anxiety or depression. Thirty-six percent replied that they were “somewhat” worried. This total of more than 75% represents a significant change from the 2015 Pew Center survey in which only 54% of parents were “somewhat” worried about their children’s mental health.
Prompted by these findings I began work on a column in which I planned to encourage pediatricians to think more like family physicians when we were working with children who were experiencing serious mental health problems. My primary message was going to be that we should turn more of our attention to the mental health of the anxious parents who must endure the often long and frustrating path toward effective psychiatric care for their children. This might come in the form of some simple suggestions about nonpharmacologic self-help strategies. Or, it could mean encouraging parents to seek psychiatric care or counseling for themselves as they wait for help for their child.
However, as I began that column, my thoughts kept drifting toward a broader consideration of the relationship between parents and pediatric mental health. If mental health of children is causing their parents to be anxious and depressed isn’t it just as likely that this is a bidirectional connection? This was not exactly an “aha” moment for me because it is a relationship I have considered for sometime. However, it is a concept that I have come to realize is receiving far too little attention.
There are exceptions. For example, a recent opinion piece in the New York Times by David French, “What if Kids Are Sad and Stressed Because Their Parents Are?” (March 19, 2023) echoes many of my concerns. Drawing on his experiences traveling around college campuses, Mr. French observes, “Just as parents are upset about their children’s anxiety and depression, children are anxious about their parent’s mental health.”
He notes that an August 2022 NBC News poll found that 58% of registered voters feel this country’s best days are behind it and joins me in imagining that this negative mind set is filtering down to the pediatric population. He acknowledges that there are other likely contributors to teen unhappiness including the ubiquity of smart phones, the secularization of society, and the media’s focus on the political divide. However, Mr. French wonders if the parenting style that results in childhood experiences that are dominated by adult supervision and protection may also be playing a large role.
In his conclusion, Mr. French asks us to consider “How much fear and anxiety should we import to our lives and homes?” as we adults search for an answer.
As I continued to drill down for other possible solutions, I encountered an avenue of psychological research that suggests that instead of, or in addition to, filtering out the anxiety-generating deluge of information, we begin to give some thought to how our beliefs may be coloring our perception of reality.
Jeremy D.W. Clifton, PhD, a psychologist at the University of Pennsylvania Positive Psychology Center has done extensive research on the relationship between our basic beliefs about the world (known as primal beliefs or simply primals in psychologist lingo) and how we interpret reality. For example, one of your primal beliefs may be that the world is a dangerous place. I, on the other hand, may see the world as a stimulating environment offering me endless opportunities to explore. I may see the world as an abundant resource limited only by my creativity. You, however, see it as a barren wasteland.
Dr. Clifton’s research has shown that our primals (at least those of adults) are relatively immutable through one’s lifetime and “do not appear to be the consequence of our experiences.” For example, living in a ZIP code with a high crime rate does not predict that you will see the world as a dangerous place. Nor does being affluent guarantee that an adult sees the world rich with opportunities.
It is unclear exactly when and by what process we develop our primal beliefs, but it is safe to say our parents probably play a large role. Exactly to what degree the tsunami of bad news we are allowing to inundate our children’s lives plays a role is unclear. However, it is reasonable to assume that news about climate change, school shootings, and the pandemic must be a contributor.
According to Dr. Clifton, there is some evidence that certain mind exercises, when applied diligently, can occasionally modify the primal beliefs of an individual who sees the world as dangerous and barren. Until such strategies become more readily accessible, the best we can do is acknowledge that our children are like canaries in a coal mine full of negative perceptions, then do our best to clear the air.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
New antiobesity drugs will benefit many. Is that bad?
where some economists opined that their coverage would be disastrous for Medicare.
Among their concerns? The drugs need to be taken long term (just like drugs for any other chronic condition). The new drugs are more expensive than the old drugs (just like new drugs for any other chronic condition). Lots of people will want to take them (just like highly effective drugs for any other chronic condition that has a significant quality-of-life or clinical impact). The U.K. recommended that they be covered only for 2 years (unlike drugs for any other chronic condition). And the Institute for Clinical and Economic Review (ICER) on which they lean heavily decided that $13,618 annually was too expensive for a medication that leads to sustained 15%-20% weight losses and those losses’ consequential benefits.
As a clinician working with patients who sustain those levels of weight loss, I find that conclusion confusing. Whether by way of lifestyle alone, or more often by way of lifestyle efforts plus medication or lifestyle efforts plus surgery, the benefits reported and seen with 15%-20% weight losses are almost uniformly huge. Patients are regularly seen discontinuing or reducing the dosage of multiple medications as a result of improvements to multiple weight-responsive comorbidities, and they also report objective benefits to mood, sleep, mobility, pain, and energy. Losing that much weight changes lives. Not to mention the impact that that degree of loss has on the primary prevention of so many diseases, including plausible reductions in many common cancers – reductions that have been shown to occur after surgery-related weight losses and for which there’s no plausible reason to imagine that they wouldn’t occur with pharmaceutical-related losses.
Are those discussions found in the NEJM op-ed or in the ICER report? Well, yes, sort of. However, in the NEJM op-ed, the word “prevention” isn’t used once, and unlike with oral hypoglycemics or antihypertensives, the authors state that with antiobesity medications, additional research is needed to determine whether medication-induced changes to A1c, blood pressure, and waist circumference would have clinical benefits: “Antiobesity medications have been shown to improve the surrogate end points of weight, glycated hemoglobin levels, systolic blood pressure, and waist circumference. Long-term studies are needed, however, to clarify how medication-induced changes in these surrogate markers translate to health outcomes.”
Primary prevention is mentioned in the ICER review, but in the “limitations” section where the authors explain that they didn’t include it in their modeling: “The long-term benefits of preventing other comorbidities including cancer, chronic kidney disease, osteoarthritis, and sleep apnea were not explicitly modeled in the base case.”
And they pretended that the impact on existing weight-responsive comorbidities mostly didn’t exist, too: “To limit the complexity of the cost-effectiveness model and to prevent double-counting of treatment benefits, we limited the long-term effects of treatments for weight management to cardiovascular risk and delays in the onset and/or diagnosis of diabetes mellitus.”
As far as cardiovascular disease (CVD) benefits go, you might have thought that it would be a slam dunk on that basis alone, at least according to a recent simple back-of-the-envelope math exercise presented at a recent American College of Cardiology conference, which applied the semaglutide treatment group weight changes in the STEP 1 trial to estimate the population impact on weight and obesity in 30- to 74-year-olds without prior CVD, and estimated 10-year CVD risks utilizing the BMI-based Framingham CVD risk scores. By their accounting, semaglutide treatment in eligible American patients has the potential to prevent over 1.6 million CVD events over 10 years.
Finally, even putting aside ICER’s admittedly and exceedingly narrow base case, what lifestyle-alone studies could ICER possibly be comparing with drug efficacy? And what does “alone” mean? Does “alone” mean with a months- or years long interprofessional behavioral program? Does “alone” mean by way of diet books? Does “alone” mean by way of simply “moving more and eating less”? I’m not aware of robust studies demonstrating any long-term meaningful, predictable, reproducible, durable weight loss outcomes for any lifestyle-only approach, intensive or otherwise.
It’s difficult for me to imagine a situation in which a drug other than an antiobesity drug would be found to have too many benefits to include in your cost-effectiveness analysis but where you’d be comfortable to run that analysis anyhow, and then come out against the drug’s recommendation and fearmonger about its use.
But then again, systemic weight bias is a hell of a drug.
Dr. Freedhoff is associate professor, department of family medicine, University of Ottawa, and medical director, Bariatric Medical Institute, Ottawa. He disclosed ties with Constant Health and Novo Nordisk, and has shared opinions via Weighty Matters and social media.
A version of this article originally appeared on Medscape.com.
where some economists opined that their coverage would be disastrous for Medicare.
Among their concerns? The drugs need to be taken long term (just like drugs for any other chronic condition). The new drugs are more expensive than the old drugs (just like new drugs for any other chronic condition). Lots of people will want to take them (just like highly effective drugs for any other chronic condition that has a significant quality-of-life or clinical impact). The U.K. recommended that they be covered only for 2 years (unlike drugs for any other chronic condition). And the Institute for Clinical and Economic Review (ICER) on which they lean heavily decided that $13,618 annually was too expensive for a medication that leads to sustained 15%-20% weight losses and those losses’ consequential benefits.
As a clinician working with patients who sustain those levels of weight loss, I find that conclusion confusing. Whether by way of lifestyle alone, or more often by way of lifestyle efforts plus medication or lifestyle efforts plus surgery, the benefits reported and seen with 15%-20% weight losses are almost uniformly huge. Patients are regularly seen discontinuing or reducing the dosage of multiple medications as a result of improvements to multiple weight-responsive comorbidities, and they also report objective benefits to mood, sleep, mobility, pain, and energy. Losing that much weight changes lives. Not to mention the impact that that degree of loss has on the primary prevention of so many diseases, including plausible reductions in many common cancers – reductions that have been shown to occur after surgery-related weight losses and for which there’s no plausible reason to imagine that they wouldn’t occur with pharmaceutical-related losses.
Are those discussions found in the NEJM op-ed or in the ICER report? Well, yes, sort of. However, in the NEJM op-ed, the word “prevention” isn’t used once, and unlike with oral hypoglycemics or antihypertensives, the authors state that with antiobesity medications, additional research is needed to determine whether medication-induced changes to A1c, blood pressure, and waist circumference would have clinical benefits: “Antiobesity medications have been shown to improve the surrogate end points of weight, glycated hemoglobin levels, systolic blood pressure, and waist circumference. Long-term studies are needed, however, to clarify how medication-induced changes in these surrogate markers translate to health outcomes.”
Primary prevention is mentioned in the ICER review, but in the “limitations” section where the authors explain that they didn’t include it in their modeling: “The long-term benefits of preventing other comorbidities including cancer, chronic kidney disease, osteoarthritis, and sleep apnea were not explicitly modeled in the base case.”
And they pretended that the impact on existing weight-responsive comorbidities mostly didn’t exist, too: “To limit the complexity of the cost-effectiveness model and to prevent double-counting of treatment benefits, we limited the long-term effects of treatments for weight management to cardiovascular risk and delays in the onset and/or diagnosis of diabetes mellitus.”
As far as cardiovascular disease (CVD) benefits go, you might have thought that it would be a slam dunk on that basis alone, at least according to a recent simple back-of-the-envelope math exercise presented at a recent American College of Cardiology conference, which applied the semaglutide treatment group weight changes in the STEP 1 trial to estimate the population impact on weight and obesity in 30- to 74-year-olds without prior CVD, and estimated 10-year CVD risks utilizing the BMI-based Framingham CVD risk scores. By their accounting, semaglutide treatment in eligible American patients has the potential to prevent over 1.6 million CVD events over 10 years.
Finally, even putting aside ICER’s admittedly and exceedingly narrow base case, what lifestyle-alone studies could ICER possibly be comparing with drug efficacy? And what does “alone” mean? Does “alone” mean with a months- or years long interprofessional behavioral program? Does “alone” mean by way of diet books? Does “alone” mean by way of simply “moving more and eating less”? I’m not aware of robust studies demonstrating any long-term meaningful, predictable, reproducible, durable weight loss outcomes for any lifestyle-only approach, intensive or otherwise.
It’s difficult for me to imagine a situation in which a drug other than an antiobesity drug would be found to have too many benefits to include in your cost-effectiveness analysis but where you’d be comfortable to run that analysis anyhow, and then come out against the drug’s recommendation and fearmonger about its use.
But then again, systemic weight bias is a hell of a drug.
Dr. Freedhoff is associate professor, department of family medicine, University of Ottawa, and medical director, Bariatric Medical Institute, Ottawa. He disclosed ties with Constant Health and Novo Nordisk, and has shared opinions via Weighty Matters and social media.
A version of this article originally appeared on Medscape.com.
where some economists opined that their coverage would be disastrous for Medicare.
Among their concerns? The drugs need to be taken long term (just like drugs for any other chronic condition). The new drugs are more expensive than the old drugs (just like new drugs for any other chronic condition). Lots of people will want to take them (just like highly effective drugs for any other chronic condition that has a significant quality-of-life or clinical impact). The U.K. recommended that they be covered only for 2 years (unlike drugs for any other chronic condition). And the Institute for Clinical and Economic Review (ICER) on which they lean heavily decided that $13,618 annually was too expensive for a medication that leads to sustained 15%-20% weight losses and those losses’ consequential benefits.
As a clinician working with patients who sustain those levels of weight loss, I find that conclusion confusing. Whether by way of lifestyle alone, or more often by way of lifestyle efforts plus medication or lifestyle efforts plus surgery, the benefits reported and seen with 15%-20% weight losses are almost uniformly huge. Patients are regularly seen discontinuing or reducing the dosage of multiple medications as a result of improvements to multiple weight-responsive comorbidities, and they also report objective benefits to mood, sleep, mobility, pain, and energy. Losing that much weight changes lives. Not to mention the impact that that degree of loss has on the primary prevention of so many diseases, including plausible reductions in many common cancers – reductions that have been shown to occur after surgery-related weight losses and for which there’s no plausible reason to imagine that they wouldn’t occur with pharmaceutical-related losses.
Are those discussions found in the NEJM op-ed or in the ICER report? Well, yes, sort of. However, in the NEJM op-ed, the word “prevention” isn’t used once, and unlike with oral hypoglycemics or antihypertensives, the authors state that with antiobesity medications, additional research is needed to determine whether medication-induced changes to A1c, blood pressure, and waist circumference would have clinical benefits: “Antiobesity medications have been shown to improve the surrogate end points of weight, glycated hemoglobin levels, systolic blood pressure, and waist circumference. Long-term studies are needed, however, to clarify how medication-induced changes in these surrogate markers translate to health outcomes.”
Primary prevention is mentioned in the ICER review, but in the “limitations” section where the authors explain that they didn’t include it in their modeling: “The long-term benefits of preventing other comorbidities including cancer, chronic kidney disease, osteoarthritis, and sleep apnea were not explicitly modeled in the base case.”
And they pretended that the impact on existing weight-responsive comorbidities mostly didn’t exist, too: “To limit the complexity of the cost-effectiveness model and to prevent double-counting of treatment benefits, we limited the long-term effects of treatments for weight management to cardiovascular risk and delays in the onset and/or diagnosis of diabetes mellitus.”
As far as cardiovascular disease (CVD) benefits go, you might have thought that it would be a slam dunk on that basis alone, at least according to a recent simple back-of-the-envelope math exercise presented at a recent American College of Cardiology conference, which applied the semaglutide treatment group weight changes in the STEP 1 trial to estimate the population impact on weight and obesity in 30- to 74-year-olds without prior CVD, and estimated 10-year CVD risks utilizing the BMI-based Framingham CVD risk scores. By their accounting, semaglutide treatment in eligible American patients has the potential to prevent over 1.6 million CVD events over 10 years.
Finally, even putting aside ICER’s admittedly and exceedingly narrow base case, what lifestyle-alone studies could ICER possibly be comparing with drug efficacy? And what does “alone” mean? Does “alone” mean with a months- or years long interprofessional behavioral program? Does “alone” mean by way of diet books? Does “alone” mean by way of simply “moving more and eating less”? I’m not aware of robust studies demonstrating any long-term meaningful, predictable, reproducible, durable weight loss outcomes for any lifestyle-only approach, intensive or otherwise.
It’s difficult for me to imagine a situation in which a drug other than an antiobesity drug would be found to have too many benefits to include in your cost-effectiveness analysis but where you’d be comfortable to run that analysis anyhow, and then come out against the drug’s recommendation and fearmonger about its use.
But then again, systemic weight bias is a hell of a drug.
Dr. Freedhoff is associate professor, department of family medicine, University of Ottawa, and medical director, Bariatric Medical Institute, Ottawa. He disclosed ties with Constant Health and Novo Nordisk, and has shared opinions via Weighty Matters and social media.
A version of this article originally appeared on Medscape.com.
Don’t fear testing for, and delabeling, penicillin allergy
You are seeing a 28-year-old man for a same-day appointment. He has a history of opioid use disorder and chronic hepatitis C virus infection. He has been using injections of heroin and fentanyl for more than 6 years, and you can see in his medical record that he has had four outpatient appointments for cutaneous infections along with three emergency department visits for same in the past 2 years. His chief complaint today is pain over his left forearm for the past 3 days. He does not report fever or other constitutional symptoms.
Examination of the left forearm reveals 8 cm of erythema with induration and calor but no fluctuance. The area is moderately tender to palpation. He has no other abnormal findings on exam.
What’s your course of action?
Dr. Vega’s take
You want to treat this patient with antibiotics and close follow-up, and you note that he has a history of penicillin allergy. A note in his record states that he had a rash after receiving amoxicillin as a child.
Sometimes, we have to take the most expedient action in health care. But most of the time, we should do the right thing, even if it’s harder. I would gather more history of this reaction to penicillin and consider an oral challenge, hoping that the work that we put in to testing him for penicillin allergy pays dividends for him now and for years to come.
Penicillin allergy is very commonly listed in patient health records. In a retrospective analysis of the charts of 11,761 patients seen at a single U.S. urban outpatient system in 2012, 11.5% had documentation of penicillin allergy. Rash was the most common manifestation listed for allergy (37% of cases), followed by unknown symptoms (20%), hives (19%), swelling/angioedema (12%), and anaphylaxis (7%). Women were nearly twice as likely as men were to report a history of penicillin allergy, and patients of Asian descent had half the reported prevalence of penicillin allergy, compared with White patients.
Only 6% of the patients reporting penicillin allergy in this study had been referred to an allergy specialist. Given the consequences of true penicillin allergy, this rate is far too low. Patients with a history of penicillin allergy have higher risks for mortality from coexisting hematologic malignancies and penicillin-sensitive infections such as Staphylococcus species. They more frequently develop resistance to multiple antimicrobials and have longer average lengths of stay in the hospital.
Getting a good history for penicillin allergy can be challenging. Approximately three-quarters of penicillin allergies are diagnosed prior to age 3 years. Some children with a family history of penicillin allergy are mislabeled as having an active allergy, even though family history is not a significant contributor to penicillin allergy. Most rashes blamed on penicillin among children are actually not immunoglobulin (Ig) E–mediated and instead represent viral exanthems.
In response to these challenges, at the end of 2022, the American Academy of Allergy, Asthma & Immunology along with the American College of Allergy, Asthma and Immunology published new recommendations for the management of drug allergy. These recommendations provide an algorithm for the active reassessment of penicillin allergy. Like other recommendations in recent years, they call for a proactive approach in questioning the potential clinical consequences of the penicillin allergy listed in the health record.
First, the guidelines recommend against needing any testing for previous adverse reactions to penicillin, such as headache, nausea/vomiting, or diarrhea, that are not IgE-mediated. However, patients who have experienced these adverse reactions may still be reticent to take penicillin. For them and for adults with a history of mild to moderate reactions to penicillin more than 5 years ago, a single oral challenge test with amoxicillin is practical and can be used to exclude penicillin allergy.
The oral amoxicillin challenge
After patients take a treatment dose of oral amoxicillin, they should be observed for 1 hour for any objective reaction. The clinical setting should be able to support patients in the rare case of a more severe reaction to penicillin. Subjective symptoms such as pruritus without objective findings such as rash may be considered a successful challenge, and penicillin may be taken off the list of allergies. The treating team can bill CPT codes for drug challenge testing.
Some research has supported multidose testing with amoxicillin to assess for late reactions to a penicillin oral challenge, but the current guidelines recommend against this approach based on the very limited yield in finding additional cases of true allergy with extra doses of antibiotics. One method to address this issue is to have patients advise the practice if symptoms develop within 10 days of the oral challenge, with photos or prompt clinical evaluation to assess for an IgE-mediated reaction.
Many patients, and certainly some clinicians, will have significant trepidation regarding an oral challenge, despite the low risk for complications. For these patients, as well as children with a history of penicillin allergy and patients with a history of anaphylaxis to penicillin or probable IgE-mediated reaction to penicillin in the past several years, skin testing is recommended. Lower-risk patients might feel reassured to complete an oral challenge test after a negative skin test.
Penicillin skin testing is more reliable than a radioallergosorbent test or an enzyme-linked immunoassay and carries a high specificity. However, skin testing requires the specialized care of an allergy clinic, and this resource is limited in many communities.
Many patients will have negative oral challenge or skin testing for penicillin allergy, but there are still some critical responsibilities for the clinician after testing is complete. First, the label of penicillin allergy should be expunged from all available health records. Second, the clinician should communicate clearly and with empathy to the patient that they can take penicillin-based antibiotics safely and with confidence. Repeat testing is unnecessary unless new symptoms develop.
But the application of this policy to clinical practice is challenging on several levels, from patient and clinician fear to practical constraints on time.
Dr. Vega is health sciences clinical professor, family medicine, University of California, Irvine. He has disclosed ties with McNeil Pharmaceuticals.
A version of this article originally appeared on Medscape.com.
You are seeing a 28-year-old man for a same-day appointment. He has a history of opioid use disorder and chronic hepatitis C virus infection. He has been using injections of heroin and fentanyl for more than 6 years, and you can see in his medical record that he has had four outpatient appointments for cutaneous infections along with three emergency department visits for same in the past 2 years. His chief complaint today is pain over his left forearm for the past 3 days. He does not report fever or other constitutional symptoms.
Examination of the left forearm reveals 8 cm of erythema with induration and calor but no fluctuance. The area is moderately tender to palpation. He has no other abnormal findings on exam.
What’s your course of action?
Dr. Vega’s take
You want to treat this patient with antibiotics and close follow-up, and you note that he has a history of penicillin allergy. A note in his record states that he had a rash after receiving amoxicillin as a child.
Sometimes, we have to take the most expedient action in health care. But most of the time, we should do the right thing, even if it’s harder. I would gather more history of this reaction to penicillin and consider an oral challenge, hoping that the work that we put in to testing him for penicillin allergy pays dividends for him now and for years to come.
Penicillin allergy is very commonly listed in patient health records. In a retrospective analysis of the charts of 11,761 patients seen at a single U.S. urban outpatient system in 2012, 11.5% had documentation of penicillin allergy. Rash was the most common manifestation listed for allergy (37% of cases), followed by unknown symptoms (20%), hives (19%), swelling/angioedema (12%), and anaphylaxis (7%). Women were nearly twice as likely as men were to report a history of penicillin allergy, and patients of Asian descent had half the reported prevalence of penicillin allergy, compared with White patients.
Only 6% of the patients reporting penicillin allergy in this study had been referred to an allergy specialist. Given the consequences of true penicillin allergy, this rate is far too low. Patients with a history of penicillin allergy have higher risks for mortality from coexisting hematologic malignancies and penicillin-sensitive infections such as Staphylococcus species. They more frequently develop resistance to multiple antimicrobials and have longer average lengths of stay in the hospital.
Getting a good history for penicillin allergy can be challenging. Approximately three-quarters of penicillin allergies are diagnosed prior to age 3 years. Some children with a family history of penicillin allergy are mislabeled as having an active allergy, even though family history is not a significant contributor to penicillin allergy. Most rashes blamed on penicillin among children are actually not immunoglobulin (Ig) E–mediated and instead represent viral exanthems.
In response to these challenges, at the end of 2022, the American Academy of Allergy, Asthma & Immunology along with the American College of Allergy, Asthma and Immunology published new recommendations for the management of drug allergy. These recommendations provide an algorithm for the active reassessment of penicillin allergy. Like other recommendations in recent years, they call for a proactive approach in questioning the potential clinical consequences of the penicillin allergy listed in the health record.
First, the guidelines recommend against needing any testing for previous adverse reactions to penicillin, such as headache, nausea/vomiting, or diarrhea, that are not IgE-mediated. However, patients who have experienced these adverse reactions may still be reticent to take penicillin. For them and for adults with a history of mild to moderate reactions to penicillin more than 5 years ago, a single oral challenge test with amoxicillin is practical and can be used to exclude penicillin allergy.
The oral amoxicillin challenge
After patients take a treatment dose of oral amoxicillin, they should be observed for 1 hour for any objective reaction. The clinical setting should be able to support patients in the rare case of a more severe reaction to penicillin. Subjective symptoms such as pruritus without objective findings such as rash may be considered a successful challenge, and penicillin may be taken off the list of allergies. The treating team can bill CPT codes for drug challenge testing.
Some research has supported multidose testing with amoxicillin to assess for late reactions to a penicillin oral challenge, but the current guidelines recommend against this approach based on the very limited yield in finding additional cases of true allergy with extra doses of antibiotics. One method to address this issue is to have patients advise the practice if symptoms develop within 10 days of the oral challenge, with photos or prompt clinical evaluation to assess for an IgE-mediated reaction.
Many patients, and certainly some clinicians, will have significant trepidation regarding an oral challenge, despite the low risk for complications. For these patients, as well as children with a history of penicillin allergy and patients with a history of anaphylaxis to penicillin or probable IgE-mediated reaction to penicillin in the past several years, skin testing is recommended. Lower-risk patients might feel reassured to complete an oral challenge test after a negative skin test.
Penicillin skin testing is more reliable than a radioallergosorbent test or an enzyme-linked immunoassay and carries a high specificity. However, skin testing requires the specialized care of an allergy clinic, and this resource is limited in many communities.
Many patients will have negative oral challenge or skin testing for penicillin allergy, but there are still some critical responsibilities for the clinician after testing is complete. First, the label of penicillin allergy should be expunged from all available health records. Second, the clinician should communicate clearly and with empathy to the patient that they can take penicillin-based antibiotics safely and with confidence. Repeat testing is unnecessary unless new symptoms develop.
But the application of this policy to clinical practice is challenging on several levels, from patient and clinician fear to practical constraints on time.
Dr. Vega is health sciences clinical professor, family medicine, University of California, Irvine. He has disclosed ties with McNeil Pharmaceuticals.
A version of this article originally appeared on Medscape.com.
You are seeing a 28-year-old man for a same-day appointment. He has a history of opioid use disorder and chronic hepatitis C virus infection. He has been using injections of heroin and fentanyl for more than 6 years, and you can see in his medical record that he has had four outpatient appointments for cutaneous infections along with three emergency department visits for same in the past 2 years. His chief complaint today is pain over his left forearm for the past 3 days. He does not report fever or other constitutional symptoms.
Examination of the left forearm reveals 8 cm of erythema with induration and calor but no fluctuance. The area is moderately tender to palpation. He has no other abnormal findings on exam.
What’s your course of action?
Dr. Vega’s take
You want to treat this patient with antibiotics and close follow-up, and you note that he has a history of penicillin allergy. A note in his record states that he had a rash after receiving amoxicillin as a child.
Sometimes, we have to take the most expedient action in health care. But most of the time, we should do the right thing, even if it’s harder. I would gather more history of this reaction to penicillin and consider an oral challenge, hoping that the work that we put in to testing him for penicillin allergy pays dividends for him now and for years to come.
Penicillin allergy is very commonly listed in patient health records. In a retrospective analysis of the charts of 11,761 patients seen at a single U.S. urban outpatient system in 2012, 11.5% had documentation of penicillin allergy. Rash was the most common manifestation listed for allergy (37% of cases), followed by unknown symptoms (20%), hives (19%), swelling/angioedema (12%), and anaphylaxis (7%). Women were nearly twice as likely as men were to report a history of penicillin allergy, and patients of Asian descent had half the reported prevalence of penicillin allergy, compared with White patients.
Only 6% of the patients reporting penicillin allergy in this study had been referred to an allergy specialist. Given the consequences of true penicillin allergy, this rate is far too low. Patients with a history of penicillin allergy have higher risks for mortality from coexisting hematologic malignancies and penicillin-sensitive infections such as Staphylococcus species. They more frequently develop resistance to multiple antimicrobials and have longer average lengths of stay in the hospital.
Getting a good history for penicillin allergy can be challenging. Approximately three-quarters of penicillin allergies are diagnosed prior to age 3 years. Some children with a family history of penicillin allergy are mislabeled as having an active allergy, even though family history is not a significant contributor to penicillin allergy. Most rashes blamed on penicillin among children are actually not immunoglobulin (Ig) E–mediated and instead represent viral exanthems.
In response to these challenges, at the end of 2022, the American Academy of Allergy, Asthma & Immunology along with the American College of Allergy, Asthma and Immunology published new recommendations for the management of drug allergy. These recommendations provide an algorithm for the active reassessment of penicillin allergy. Like other recommendations in recent years, they call for a proactive approach in questioning the potential clinical consequences of the penicillin allergy listed in the health record.
First, the guidelines recommend against needing any testing for previous adverse reactions to penicillin, such as headache, nausea/vomiting, or diarrhea, that are not IgE-mediated. However, patients who have experienced these adverse reactions may still be reticent to take penicillin. For them and for adults with a history of mild to moderate reactions to penicillin more than 5 years ago, a single oral challenge test with amoxicillin is practical and can be used to exclude penicillin allergy.
The oral amoxicillin challenge
After patients take a treatment dose of oral amoxicillin, they should be observed for 1 hour for any objective reaction. The clinical setting should be able to support patients in the rare case of a more severe reaction to penicillin. Subjective symptoms such as pruritus without objective findings such as rash may be considered a successful challenge, and penicillin may be taken off the list of allergies. The treating team can bill CPT codes for drug challenge testing.
Some research has supported multidose testing with amoxicillin to assess for late reactions to a penicillin oral challenge, but the current guidelines recommend against this approach based on the very limited yield in finding additional cases of true allergy with extra doses of antibiotics. One method to address this issue is to have patients advise the practice if symptoms develop within 10 days of the oral challenge, with photos or prompt clinical evaluation to assess for an IgE-mediated reaction.
Many patients, and certainly some clinicians, will have significant trepidation regarding an oral challenge, despite the low risk for complications. For these patients, as well as children with a history of penicillin allergy and patients with a history of anaphylaxis to penicillin or probable IgE-mediated reaction to penicillin in the past several years, skin testing is recommended. Lower-risk patients might feel reassured to complete an oral challenge test after a negative skin test.
Penicillin skin testing is more reliable than a radioallergosorbent test or an enzyme-linked immunoassay and carries a high specificity. However, skin testing requires the specialized care of an allergy clinic, and this resource is limited in many communities.
Many patients will have negative oral challenge or skin testing for penicillin allergy, but there are still some critical responsibilities for the clinician after testing is complete. First, the label of penicillin allergy should be expunged from all available health records. Second, the clinician should communicate clearly and with empathy to the patient that they can take penicillin-based antibiotics safely and with confidence. Repeat testing is unnecessary unless new symptoms develop.
But the application of this policy to clinical practice is challenging on several levels, from patient and clinician fear to practical constraints on time.
Dr. Vega is health sciences clinical professor, family medicine, University of California, Irvine. He has disclosed ties with McNeil Pharmaceuticals.
A version of this article originally appeared on Medscape.com.
‘Excess’ deaths surging, but why?
This transcript has been edited for clarity.
“Excess deaths.” You’ve heard the phrase countless times by now. It is one of the myriad of previously esoteric epidemiology terms that the pandemic brought squarely into the zeitgeist.
As a sort of standard candle of the performance of a state or a region or a country in terms of health care, it has a lot of utility – if for nothing more than Monday-morning quarterbacking. But this week, I want to dig in on the concept a bit because, according to a new study, the excess death gap between the United States and Western Europe has never been higher.
You might imagine that the best way to figure this out is for some group of intelligent people to review each death and decide, somehow, whether it was expected or not. But aside from being impractical, this would end up being somewhat subjective. That older person who died from pneumonia – was that an expected death? Could it have been avoided?
Rather, the calculation of excess mortality relies on large numbers and statistical inference to compare an expected number of deaths with those that are observed.
The difference is excess mortality, even if you can never be sure whether any particular death was expected or not.
As always, however, the devil is in the details. What data do you use to define the expected number of deaths?
There are options here. Probably the most straightforward analysis uses past data from the country of interest. You look at annual deaths over some historical period of time and compare those numbers with the rates today. Two issues need to be accounted for here: population growth – a larger population will have more deaths, so you need to adjust the historical population with current levels, and demographic shifts – an older or more male population will have more deaths, so you need to adjust for that as well.
But provided you take care of those factors, you can estimate fairly well how many deaths you can expect to see in any given period of time.
Still, you should see right away that excess mortality is a relative concept. If you think that, just perhaps, the United States has some systematic failure to deliver care that has been stable and persistent over time, you wouldn’t capture that failing in an excess mortality calculation that uses U.S. historical data as the baseline.
The best way to get around that is to use data from other countries, and that’s just what this article – a rare single-author piece by Patrick Heuveline – does, calculating excess deaths in the United States by standardizing our mortality rates to the five largest Western European countries: the United Kingdom, France, Germany, Italy, and Spain.
Controlling for the differences in the demographics of that European population, here is the expected number of deaths in the United States over the past 5 years.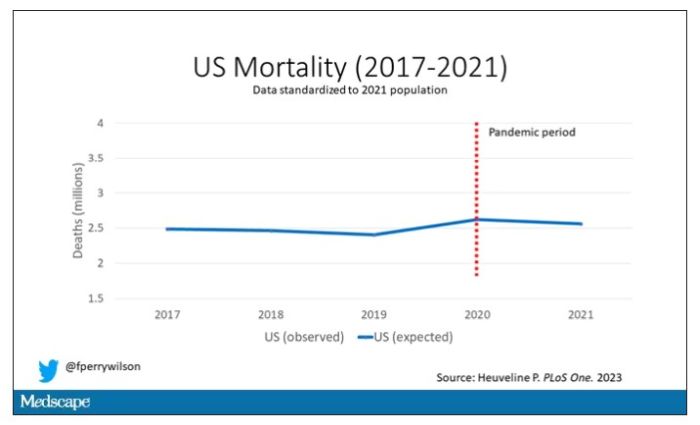
Note that there is a small uptick in expected deaths in 2020, reflecting the pandemic, which returns to baseline levels by 2021. This is because that’s what happened in Europe; by 2021, the excess mortality due to COVID-19 was quite low.
Here are the actual deaths in the US during that time.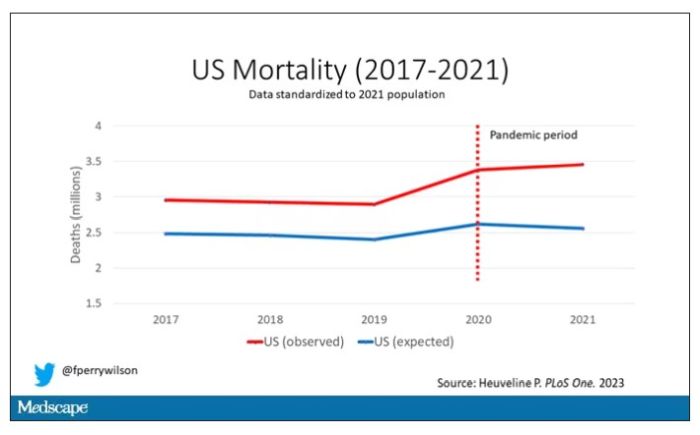
Highlighted here in green, then, is the excess mortality over time in the United States.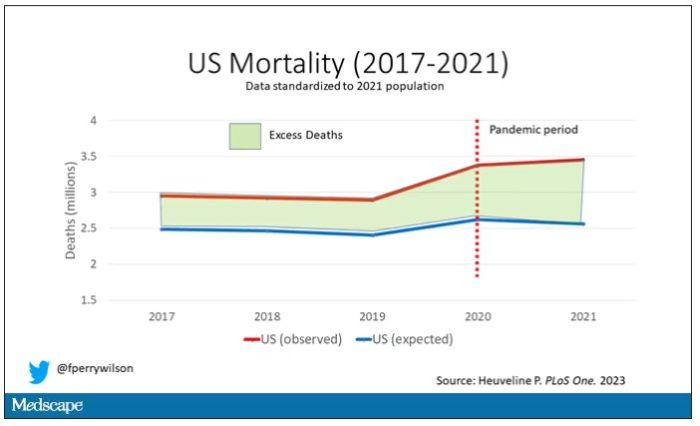
There are some fascinating and concerning findings here.
First of all, you can see that even before the pandemic, the United States has an excess mortality problem. This is not entirely a surprise; we’ve known that so-called “deaths of despair,” those due to alcohol abuse, drug overdoses, and suicide, are at an all-time high and tend to affect a “prime of life” population that would not otherwise be expected to die. In fact, fully 50% of the excess deaths in the United States occur in those between ages 15 and 64.
Excess deaths are also a concerning percentage of total deaths. In 2017, 17% of total deaths in the United States could be considered “excess.” In 2021, that number had doubled to 35%. Nearly 900,000 individuals in the United States died in 2021 who perhaps didn’t need to.
The obvious culprit to blame here is COVID, but COVID-associated excess deaths only explain about 50% of the excess we see in 2021. The rest reflect something even more concerning: a worsening of the failures of the past, perhaps exacerbated by the pandemic but not due to the virus itself.
Of course, we started this discussion acknowledging that the calculation of excess mortality is exquisitely dependent on how you model the expected number of deaths, and I’m sure some will take issue with the use of European numbers when applied to Americans. After all, Europe has, by and large, a robust public health service, socialized medicine, and healthcare that does not run the risk of bankrupting its citizens. How can we compare our outcomes to a place like that?
How indeed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven,Conn. He reported no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
“Excess deaths.” You’ve heard the phrase countless times by now. It is one of the myriad of previously esoteric epidemiology terms that the pandemic brought squarely into the zeitgeist.
As a sort of standard candle of the performance of a state or a region or a country in terms of health care, it has a lot of utility – if for nothing more than Monday-morning quarterbacking. But this week, I want to dig in on the concept a bit because, according to a new study, the excess death gap between the United States and Western Europe has never been higher.
You might imagine that the best way to figure this out is for some group of intelligent people to review each death and decide, somehow, whether it was expected or not. But aside from being impractical, this would end up being somewhat subjective. That older person who died from pneumonia – was that an expected death? Could it have been avoided?
Rather, the calculation of excess mortality relies on large numbers and statistical inference to compare an expected number of deaths with those that are observed.
The difference is excess mortality, even if you can never be sure whether any particular death was expected or not.
As always, however, the devil is in the details. What data do you use to define the expected number of deaths?
There are options here. Probably the most straightforward analysis uses past data from the country of interest. You look at annual deaths over some historical period of time and compare those numbers with the rates today. Two issues need to be accounted for here: population growth – a larger population will have more deaths, so you need to adjust the historical population with current levels, and demographic shifts – an older or more male population will have more deaths, so you need to adjust for that as well.
But provided you take care of those factors, you can estimate fairly well how many deaths you can expect to see in any given period of time.
Still, you should see right away that excess mortality is a relative concept. If you think that, just perhaps, the United States has some systematic failure to deliver care that has been stable and persistent over time, you wouldn’t capture that failing in an excess mortality calculation that uses U.S. historical data as the baseline.
The best way to get around that is to use data from other countries, and that’s just what this article – a rare single-author piece by Patrick Heuveline – does, calculating excess deaths in the United States by standardizing our mortality rates to the five largest Western European countries: the United Kingdom, France, Germany, Italy, and Spain.
Controlling for the differences in the demographics of that European population, here is the expected number of deaths in the United States over the past 5 years.
Note that there is a small uptick in expected deaths in 2020, reflecting the pandemic, which returns to baseline levels by 2021. This is because that’s what happened in Europe; by 2021, the excess mortality due to COVID-19 was quite low.
Here are the actual deaths in the US during that time.
Highlighted here in green, then, is the excess mortality over time in the United States.
There are some fascinating and concerning findings here.
First of all, you can see that even before the pandemic, the United States has an excess mortality problem. This is not entirely a surprise; we’ve known that so-called “deaths of despair,” those due to alcohol abuse, drug overdoses, and suicide, are at an all-time high and tend to affect a “prime of life” population that would not otherwise be expected to die. In fact, fully 50% of the excess deaths in the United States occur in those between ages 15 and 64.
Excess deaths are also a concerning percentage of total deaths. In 2017, 17% of total deaths in the United States could be considered “excess.” In 2021, that number had doubled to 35%. Nearly 900,000 individuals in the United States died in 2021 who perhaps didn’t need to.
The obvious culprit to blame here is COVID, but COVID-associated excess deaths only explain about 50% of the excess we see in 2021. The rest reflect something even more concerning: a worsening of the failures of the past, perhaps exacerbated by the pandemic but not due to the virus itself.
Of course, we started this discussion acknowledging that the calculation of excess mortality is exquisitely dependent on how you model the expected number of deaths, and I’m sure some will take issue with the use of European numbers when applied to Americans. After all, Europe has, by and large, a robust public health service, socialized medicine, and healthcare that does not run the risk of bankrupting its citizens. How can we compare our outcomes to a place like that?
How indeed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven,Conn. He reported no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
This transcript has been edited for clarity.
“Excess deaths.” You’ve heard the phrase countless times by now. It is one of the myriad of previously esoteric epidemiology terms that the pandemic brought squarely into the zeitgeist.
As a sort of standard candle of the performance of a state or a region or a country in terms of health care, it has a lot of utility – if for nothing more than Monday-morning quarterbacking. But this week, I want to dig in on the concept a bit because, according to a new study, the excess death gap between the United States and Western Europe has never been higher.
You might imagine that the best way to figure this out is for some group of intelligent people to review each death and decide, somehow, whether it was expected or not. But aside from being impractical, this would end up being somewhat subjective. That older person who died from pneumonia – was that an expected death? Could it have been avoided?
Rather, the calculation of excess mortality relies on large numbers and statistical inference to compare an expected number of deaths with those that are observed.
The difference is excess mortality, even if you can never be sure whether any particular death was expected or not.
As always, however, the devil is in the details. What data do you use to define the expected number of deaths?
There are options here. Probably the most straightforward analysis uses past data from the country of interest. You look at annual deaths over some historical period of time and compare those numbers with the rates today. Two issues need to be accounted for here: population growth – a larger population will have more deaths, so you need to adjust the historical population with current levels, and demographic shifts – an older or more male population will have more deaths, so you need to adjust for that as well.
But provided you take care of those factors, you can estimate fairly well how many deaths you can expect to see in any given period of time.
Still, you should see right away that excess mortality is a relative concept. If you think that, just perhaps, the United States has some systematic failure to deliver care that has been stable and persistent over time, you wouldn’t capture that failing in an excess mortality calculation that uses U.S. historical data as the baseline.
The best way to get around that is to use data from other countries, and that’s just what this article – a rare single-author piece by Patrick Heuveline – does, calculating excess deaths in the United States by standardizing our mortality rates to the five largest Western European countries: the United Kingdom, France, Germany, Italy, and Spain.
Controlling for the differences in the demographics of that European population, here is the expected number of deaths in the United States over the past 5 years.
Note that there is a small uptick in expected deaths in 2020, reflecting the pandemic, which returns to baseline levels by 2021. This is because that’s what happened in Europe; by 2021, the excess mortality due to COVID-19 was quite low.
Here are the actual deaths in the US during that time.
Highlighted here in green, then, is the excess mortality over time in the United States.
There are some fascinating and concerning findings here.
First of all, you can see that even before the pandemic, the United States has an excess mortality problem. This is not entirely a surprise; we’ve known that so-called “deaths of despair,” those due to alcohol abuse, drug overdoses, and suicide, are at an all-time high and tend to affect a “prime of life” population that would not otherwise be expected to die. In fact, fully 50% of the excess deaths in the United States occur in those between ages 15 and 64.
Excess deaths are also a concerning percentage of total deaths. In 2017, 17% of total deaths in the United States could be considered “excess.” In 2021, that number had doubled to 35%. Nearly 900,000 individuals in the United States died in 2021 who perhaps didn’t need to.
The obvious culprit to blame here is COVID, but COVID-associated excess deaths only explain about 50% of the excess we see in 2021. The rest reflect something even more concerning: a worsening of the failures of the past, perhaps exacerbated by the pandemic but not due to the virus itself.
Of course, we started this discussion acknowledging that the calculation of excess mortality is exquisitely dependent on how you model the expected number of deaths, and I’m sure some will take issue with the use of European numbers when applied to Americans. After all, Europe has, by and large, a robust public health service, socialized medicine, and healthcare that does not run the risk of bankrupting its citizens. How can we compare our outcomes to a place like that?
How indeed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven,Conn. He reported no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
Is it time to stop treating high triglycerides?
The publication of the PROMINENT trial, where pemafibrate successfully lowered high levels but was not associated with a lower risk for cardiovascular events, reinforced the point. Is it time to stop measuring and treating high triglycerides?
There may be noncardiovascular reasons to treat hypertriglyceridemia. Pancreatitis is the most cited one, given that the risk for pancreatitis increases with increasing triglyceride levels, especially in patients with a prior episode.
There may also be practical reasons to lower trigs. Because most cholesterol panels use the Friedewald equation to calculate low-density lipoprotein cholesterol (LDL-C) rather than measuring it directly, very high triglyceride levels can invalidate the calculation and return error messages on lab reports.
But we now have alternatives to measuring LDL-C, including non–high-density lipoprotein cholesterol (HDL-C) and apolipoprotein B (apoB), that better predict risk and are usable even in the setting of nonfasting samples when triglycerides are elevated.
Independent cardiovascular risk factor?
If we are going to measure and treat high triglycerides for cardiovascular reasons, the relevant question is, are high triglycerides an independent risk factor for cardiovascular disease?
Proponents have a broad swath of supportive literature to point at. Multiple studies have shown an association between triglyceride levels and cardiovascular risk. The evidence even extends beyond traditional epidemiologic analyses, to genetic studies that should be free from some of the problems seen in observational cohorts.
But it is difficult to be certain whether these associations are causal or merely confounding. An unhealthy diet will increase triglycerides, as will alcohol. Patients with diabetes or metabolic syndrome have high triglycerides. So do patients with nephrotic syndrome or hypothyroidism, or hypertensive patients taking thiazide diuretics. Adjusting for these baseline factors is possible but imperfect, and residual confounding is always an issue. An analysis of the Reykjavik and the EPIC-Norfolk studies found an association between triglyceride levels and cardiovascular risk. That risk was attenuated, but not eliminated, when adjusted for traditional risk factors such as age, smoking, blood pressure, diabetes, and cholesterol.
Randomized trials of triglyceride-lowering therapies would help resolve the question of whether hypertriglyceridemia contributes to coronary disease or simply identifies high-risk patients. Early trials seemed to support the idea of a causal link. The Helsinki Heart Study randomized patients to gemfibrozil or placebo and found a 34% relative risk reduction in coronary artery disease with the fibrate. But gemfibrozil didn’t only reduce triglycerides. It also increased HDL-C and lowered LDL-C relative to placebo, which may explain the observed benefit.
Gemfibrozil is rarely used today because we can achieve much greater LDL-C reductions with statins, as well as ezetimibe and PCSK9 inhibitors. The success of these drugs may not leave any room for triglyceride-lowering medications.
The pre- vs. post-statin era
In the 2005 FIELD study, participants were randomized to receive fenofibrate or placebo. Although patients weren’t taking statin at study entry, 17% of the placebo group started taking one during the trial. Fenofibrate wasn’t associated with a reduction in the primary endpoint, a combination of coronary heart disease death or nonfatal myocardial infarction (MI). Among the many secondary endpoints, nonfatal MI was lower but cardiovascular mortality was not in the fibrate-treated patients. In the same vein, the 2010 ACCORD study randomized patients to receive simvastatin plus fenofibrate or simvastatin alone. The composite primary outcome of MI, stroke, and cardiovascular mortality was not lowered nor were any secondary outcomes with the combination therapy. In the statin era, triglyceride-lowering therapies have not shown much benefit.
The final nail in the coffin may very well be the aforementioned PROMINENT trial. The new agent, pemafibrate, fared no better than its predecessor fenofibrate. Pemafibrate had no impact on the study’s primary composite outcome of nonfatal MI, stroke, coronary revascularization, or cardiovascular death despite being very effective at lowering triglycerides (by more than 25%). Patients treated with pemafibrate had increased LDL-C and apoB compared with the placebo group. When you realize that, the results of the study are not very surprising.
Some point to the results of REDUCE-IT as proof that triglycerides are still a valid target for pharmacotherapy. The debate on whether REDUCE-IT tested a good drug or a bad placebo is one for another day. The salient point for today is that the benefits of eicosapentaenoic acid (EPA) were seen regardless of either baseline or final triglyceride level. EPA may lower cardiac risk, but there is no widespread consensus that it does so by lowering triglycerides. There may be other mechanisms at work.
You could still argue that high triglycerides have value as a risk prediction tool even if their role as a target for drug therapy is questionable. There was a time when medications to lower triglycerides had a benefit. But this is the post-statin era, and that time has passed.
If you see patients with high triglycerides, treating them with triglyceride-lowering medication probably isn’t going to reduce their cardiovascular risk. Dietary interventions, encouraging exercise, and reducing alcohol consumption are better options. Not only will they lead to lower cholesterol levels, but they’ll lower cardiovascular risk, too.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal, with a degree in epidemiology. He has disclosed no relevant financial relationships. He spends most of his time doing things that he doesn’t get paid for, like research, teaching, and podcasting. Occasionally he finds time to practice cardiology to pay the rent. He realizes that half of his research findings will be disproved in 5 years; he just doesn’t know which half. He is a regular contributor to the Montreal Gazette, CJAD radio, and CTV television in Montreal and is host of the award-winning podcast The Body of Evidence. The Body of Evidence.
A version of this article originally appeared on Medscape.com.
The publication of the PROMINENT trial, where pemafibrate successfully lowered high levels but was not associated with a lower risk for cardiovascular events, reinforced the point. Is it time to stop measuring and treating high triglycerides?
There may be noncardiovascular reasons to treat hypertriglyceridemia. Pancreatitis is the most cited one, given that the risk for pancreatitis increases with increasing triglyceride levels, especially in patients with a prior episode.
There may also be practical reasons to lower trigs. Because most cholesterol panels use the Friedewald equation to calculate low-density lipoprotein cholesterol (LDL-C) rather than measuring it directly, very high triglyceride levels can invalidate the calculation and return error messages on lab reports.
But we now have alternatives to measuring LDL-C, including non–high-density lipoprotein cholesterol (HDL-C) and apolipoprotein B (apoB), that better predict risk and are usable even in the setting of nonfasting samples when triglycerides are elevated.
Independent cardiovascular risk factor?
If we are going to measure and treat high triglycerides for cardiovascular reasons, the relevant question is, are high triglycerides an independent risk factor for cardiovascular disease?
Proponents have a broad swath of supportive literature to point at. Multiple studies have shown an association between triglyceride levels and cardiovascular risk. The evidence even extends beyond traditional epidemiologic analyses, to genetic studies that should be free from some of the problems seen in observational cohorts.
But it is difficult to be certain whether these associations are causal or merely confounding. An unhealthy diet will increase triglycerides, as will alcohol. Patients with diabetes or metabolic syndrome have high triglycerides. So do patients with nephrotic syndrome or hypothyroidism, or hypertensive patients taking thiazide diuretics. Adjusting for these baseline factors is possible but imperfect, and residual confounding is always an issue. An analysis of the Reykjavik and the EPIC-Norfolk studies found an association between triglyceride levels and cardiovascular risk. That risk was attenuated, but not eliminated, when adjusted for traditional risk factors such as age, smoking, blood pressure, diabetes, and cholesterol.
Randomized trials of triglyceride-lowering therapies would help resolve the question of whether hypertriglyceridemia contributes to coronary disease or simply identifies high-risk patients. Early trials seemed to support the idea of a causal link. The Helsinki Heart Study randomized patients to gemfibrozil or placebo and found a 34% relative risk reduction in coronary artery disease with the fibrate. But gemfibrozil didn’t only reduce triglycerides. It also increased HDL-C and lowered LDL-C relative to placebo, which may explain the observed benefit.
Gemfibrozil is rarely used today because we can achieve much greater LDL-C reductions with statins, as well as ezetimibe and PCSK9 inhibitors. The success of these drugs may not leave any room for triglyceride-lowering medications.
The pre- vs. post-statin era
In the 2005 FIELD study, participants were randomized to receive fenofibrate or placebo. Although patients weren’t taking statin at study entry, 17% of the placebo group started taking one during the trial. Fenofibrate wasn’t associated with a reduction in the primary endpoint, a combination of coronary heart disease death or nonfatal myocardial infarction (MI). Among the many secondary endpoints, nonfatal MI was lower but cardiovascular mortality was not in the fibrate-treated patients. In the same vein, the 2010 ACCORD study randomized patients to receive simvastatin plus fenofibrate or simvastatin alone. The composite primary outcome of MI, stroke, and cardiovascular mortality was not lowered nor were any secondary outcomes with the combination therapy. In the statin era, triglyceride-lowering therapies have not shown much benefit.
The final nail in the coffin may very well be the aforementioned PROMINENT trial. The new agent, pemafibrate, fared no better than its predecessor fenofibrate. Pemafibrate had no impact on the study’s primary composite outcome of nonfatal MI, stroke, coronary revascularization, or cardiovascular death despite being very effective at lowering triglycerides (by more than 25%). Patients treated with pemafibrate had increased LDL-C and apoB compared with the placebo group. When you realize that, the results of the study are not very surprising.
Some point to the results of REDUCE-IT as proof that triglycerides are still a valid target for pharmacotherapy. The debate on whether REDUCE-IT tested a good drug or a bad placebo is one for another day. The salient point for today is that the benefits of eicosapentaenoic acid (EPA) were seen regardless of either baseline or final triglyceride level. EPA may lower cardiac risk, but there is no widespread consensus that it does so by lowering triglycerides. There may be other mechanisms at work.
You could still argue that high triglycerides have value as a risk prediction tool even if their role as a target for drug therapy is questionable. There was a time when medications to lower triglycerides had a benefit. But this is the post-statin era, and that time has passed.
If you see patients with high triglycerides, treating them with triglyceride-lowering medication probably isn’t going to reduce their cardiovascular risk. Dietary interventions, encouraging exercise, and reducing alcohol consumption are better options. Not only will they lead to lower cholesterol levels, but they’ll lower cardiovascular risk, too.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal, with a degree in epidemiology. He has disclosed no relevant financial relationships. He spends most of his time doing things that he doesn’t get paid for, like research, teaching, and podcasting. Occasionally he finds time to practice cardiology to pay the rent. He realizes that half of his research findings will be disproved in 5 years; he just doesn’t know which half. He is a regular contributor to the Montreal Gazette, CJAD radio, and CTV television in Montreal and is host of the award-winning podcast The Body of Evidence. The Body of Evidence.
A version of this article originally appeared on Medscape.com.
The publication of the PROMINENT trial, where pemafibrate successfully lowered high levels but was not associated with a lower risk for cardiovascular events, reinforced the point. Is it time to stop measuring and treating high triglycerides?
There may be noncardiovascular reasons to treat hypertriglyceridemia. Pancreatitis is the most cited one, given that the risk for pancreatitis increases with increasing triglyceride levels, especially in patients with a prior episode.
There may also be practical reasons to lower trigs. Because most cholesterol panels use the Friedewald equation to calculate low-density lipoprotein cholesterol (LDL-C) rather than measuring it directly, very high triglyceride levels can invalidate the calculation and return error messages on lab reports.
But we now have alternatives to measuring LDL-C, including non–high-density lipoprotein cholesterol (HDL-C) and apolipoprotein B (apoB), that better predict risk and are usable even in the setting of nonfasting samples when triglycerides are elevated.
Independent cardiovascular risk factor?
If we are going to measure and treat high triglycerides for cardiovascular reasons, the relevant question is, are high triglycerides an independent risk factor for cardiovascular disease?
Proponents have a broad swath of supportive literature to point at. Multiple studies have shown an association between triglyceride levels and cardiovascular risk. The evidence even extends beyond traditional epidemiologic analyses, to genetic studies that should be free from some of the problems seen in observational cohorts.
But it is difficult to be certain whether these associations are causal or merely confounding. An unhealthy diet will increase triglycerides, as will alcohol. Patients with diabetes or metabolic syndrome have high triglycerides. So do patients with nephrotic syndrome or hypothyroidism, or hypertensive patients taking thiazide diuretics. Adjusting for these baseline factors is possible but imperfect, and residual confounding is always an issue. An analysis of the Reykjavik and the EPIC-Norfolk studies found an association between triglyceride levels and cardiovascular risk. That risk was attenuated, but not eliminated, when adjusted for traditional risk factors such as age, smoking, blood pressure, diabetes, and cholesterol.
Randomized trials of triglyceride-lowering therapies would help resolve the question of whether hypertriglyceridemia contributes to coronary disease or simply identifies high-risk patients. Early trials seemed to support the idea of a causal link. The Helsinki Heart Study randomized patients to gemfibrozil or placebo and found a 34% relative risk reduction in coronary artery disease with the fibrate. But gemfibrozil didn’t only reduce triglycerides. It also increased HDL-C and lowered LDL-C relative to placebo, which may explain the observed benefit.
Gemfibrozil is rarely used today because we can achieve much greater LDL-C reductions with statins, as well as ezetimibe and PCSK9 inhibitors. The success of these drugs may not leave any room for triglyceride-lowering medications.
The pre- vs. post-statin era
In the 2005 FIELD study, participants were randomized to receive fenofibrate or placebo. Although patients weren’t taking statin at study entry, 17% of the placebo group started taking one during the trial. Fenofibrate wasn’t associated with a reduction in the primary endpoint, a combination of coronary heart disease death or nonfatal myocardial infarction (MI). Among the many secondary endpoints, nonfatal MI was lower but cardiovascular mortality was not in the fibrate-treated patients. In the same vein, the 2010 ACCORD study randomized patients to receive simvastatin plus fenofibrate or simvastatin alone. The composite primary outcome of MI, stroke, and cardiovascular mortality was not lowered nor were any secondary outcomes with the combination therapy. In the statin era, triglyceride-lowering therapies have not shown much benefit.
The final nail in the coffin may very well be the aforementioned PROMINENT trial. The new agent, pemafibrate, fared no better than its predecessor fenofibrate. Pemafibrate had no impact on the study’s primary composite outcome of nonfatal MI, stroke, coronary revascularization, or cardiovascular death despite being very effective at lowering triglycerides (by more than 25%). Patients treated with pemafibrate had increased LDL-C and apoB compared with the placebo group. When you realize that, the results of the study are not very surprising.
Some point to the results of REDUCE-IT as proof that triglycerides are still a valid target for pharmacotherapy. The debate on whether REDUCE-IT tested a good drug or a bad placebo is one for another day. The salient point for today is that the benefits of eicosapentaenoic acid (EPA) were seen regardless of either baseline or final triglyceride level. EPA may lower cardiac risk, but there is no widespread consensus that it does so by lowering triglycerides. There may be other mechanisms at work.
You could still argue that high triglycerides have value as a risk prediction tool even if their role as a target for drug therapy is questionable. There was a time when medications to lower triglycerides had a benefit. But this is the post-statin era, and that time has passed.
If you see patients with high triglycerides, treating them with triglyceride-lowering medication probably isn’t going to reduce their cardiovascular risk. Dietary interventions, encouraging exercise, and reducing alcohol consumption are better options. Not only will they lead to lower cholesterol levels, but they’ll lower cardiovascular risk, too.
Dr. Labos is a cardiologist at Hôpital Notre-Dame, Montreal, with a degree in epidemiology. He has disclosed no relevant financial relationships. He spends most of his time doing things that he doesn’t get paid for, like research, teaching, and podcasting. Occasionally he finds time to practice cardiology to pay the rent. He realizes that half of his research findings will be disproved in 5 years; he just doesn’t know which half. He is a regular contributor to the Montreal Gazette, CJAD radio, and CTV television in Montreal and is host of the award-winning podcast The Body of Evidence. The Body of Evidence.
A version of this article originally appeared on Medscape.com.