User login
Distribution based on contribution: The merit-based ACO shared savings distribution model
Our nation is in the midst of an inexorable shift in health care delivery from "pay for volume" to "pay for value." It is well documented that our current largely fee-for-service system is unsustainable and a dramatic incentive shift must occur. Every provider needs to be committed to providing the highest quality at the lowest cost. This is the fundamental goal of the pay-for-value system.
If quality and patient satisfaction criteria are met and providers working together in an accountable care organization or similar entity create savings for a defined patient population, then the ACO usually gets a portion of the savings, commonly 50%. Unlike capitated arrangements, shared savings arrangements can avoid or limit downside financial risk and therefore can serve as stepping-stones toward fuller accountability and incentives. They are quite appropriate for start-up and smaller ACOs.
The ACO gets the savings, if there are any. But what the ACO does with them is crucial to the success and sustainability of the organization. "ACOs must offer a realistic and achievable opportunity for providers to share in the savings created from delivering higher-value care. The incentive system must reward providers for delivering efficient care as opposed to the current volume-driven system" (The ACO Toolkit; the Dartmouth Institute, p. 9, Jan. 2011).
If providers or hospital stakeholders feel that their efforts to drive value are not being fairly recognized, they will no longer participate meaningfully, the goals of value-based medicine will be thwarted, and savings will not occur in the long-run. Before signing a participation contract, physicians should scrutinize how each ACO plans to distribute the savings it receives.
The Centers for Medicare and Medicaid Services administers the Medicare Shared Savings Program (MSSP). The fact that CMS’s regulations concerning MSSP are not prescriptive about a given savings distribution formula gives ACOs flexibility in this area. But the regulations are specific about the ultimate purpose of distributions: "As part of its application, an ACO must describe the following: (1) how it plans to use shared savings payments, including the criteria it plans to employ for distributing shared savings among its ACO participants and ACO providers/suppliers, ... and (3) how the proposed plan will achieve the general aims of better care for individuals, better health for populations, and lower growth in expenditures" (42 CFR 425.204(d), 76 Fed. Reg. 6798 [Nov. 2, 2011]).
Fatal flaw?
Some ACOs, however, have lost sight of the fact that failure to have a fair shared savings distribution formula (linking relative distributions to relative contributions) will be fatal to its sustainability. Some view them as "profits" to go to the owners or shareholders. Some simply lock in a fixed allocation similar to fee-for-service payment ratios, without regard to who generated the savings. Some employers of physicians have contracted to compensate only on a work production basis with zero performance incentive payments at all. Other ACOs are putting off the issue because it is sensitive culturally. As health care moves more and more to value-based compensation, the distribution of savings must be viewed primarily as the providers’ professional remuneration and not corporate "profit." Payments for administrative services and debt service must, of course, come out of the savings distribution to "keep the pump primed," but they should be carefully managed. The bulk must be distributed in proportion to contribution toward quality and cost-effective care.
One physician stated, "No physician is going to join an ACO when someone else is telling them what they are worth unless they know that the savings distribution formula is impeccably fair." To those putting off design of a fair merit-based compensation system until there is more physician buy-in, we respectfully submit that you cannot get buy-in without one.
A need for honed metrics
Yes, this concept is pretty basic when you think about it. But though it may be easy to understand, it can be complex to implement, especially when multiple specialists and facilities are involved in an ACO’s care coordination. One not only needs to determine the relative potential and actual value contribution for each provider, but also the clinically valid metrics by which to measure them. Under fee for service, metrics for success were usually transactional and objective (in other words, volume of procedure times rate). An ACO’s success metrics may be neither. Success may come from things not happening (that is, fewer ED visits, avoidable admissions, and reduced readmissions). At the same time, the distribution model needs to be clear, practical, and capable of being understood by all.
But there can be a replicable framework for any ACO to use to create a fair and sustainable shared savings distribution model. There are necessary subjective judgments – at this time, many metrics are imprecise or nonexistent – and the sophistication of the distribution process must parallel the sophistication of the ACO’s infrastructure. But, if the right people are involved and apply the ACO’s guiding principles on savings allocation, participants will be appropriately incentivized. The precision of distribution application will grow over time. Don’t let the perfect be the enemy of the good.
The six guiding principles for shared savings distribution
Though application will vary widely because of differing circumstances and types of initiatives, chances for success will increase if every activity can be judged by whether it is consistent with a set of guiding principles viewed as fair by the ACO members. You may want to consider a savings distribution formula with the following principles:
• Eyes on the prize: Triple Aim. It offers incentives for the delivery of high-quality and cost-effective care to achieve the Triple Aim – better care for individuals, better health for populations, and lower per capita costs.
• Broad provider input. It is the result of input from a diverse spectrum of knowledgeable providers who understand what drives patient population value.
• Fairness. It is fair to all in that it links relative distribution to relative contribution to the organization’s total savings and quality performance, and adheres to measurable clinically valid metrics.
• Transparency. It is clear, transparent, practical to implement and replicable.
• Constant evolution. It adapts and improves as the capabilities and experience as the ACO grows.
• Maximized incentive to drive value by all participants. After prudently meeting overhead costs, it allows gradual transition as well as commercially reasonable return on capital investment or debt service. It makes the most of ongoing incentive programs for all to deliver value by distributing as much of the savings surplus as possible to those who generate them.
Weighting: How to assign relative percentage among providers
As mentioned, it is important that design of a fair distribution formula be the product of collaboration among informed and committed clinicians who understand patient population management. Like virtually all organization compensation formulas, the determination of relative contributions of the different providers in a given ACO, or care initiative within the ACO, will involve a certain amount of inherent subjectivity but will be guided by weighted criteria applied in good faith.
• Step 1: Break down each initiative into its value-adding elements and assign provider responsibility for each. The ACO will have a number of different care management initiatives. Some, like outpatient diabetes management, may be completely the responsibility of one provider specialty, (that is, primary care). Others may involve coordination across multiple settings for patients with multiple conditions involving multiple specialties. Each initiative was chosen for a reason – to drive value. In setting relative potential distribution percentages, envision the perfect implementation of each initiative. Next, look at what tasks or best practices are needed to drive success, and then who is assigned responsibility for each.
• Step 2: Assign relative percentages to each specialty relative to its potential to realize savings. For a pure primary care prevention initiative, they would get 100% in all categories. For multispecialty initiatives, the percentage is tied to the proportion of those savings predicted to flow from that provider class.
N.B.: Historically, cost centers are not necessarily the cost savers. A mature ACO will be able to allocate savings to each initiative and the relative savings distribution within each. But for a start-up ACO, because it is so apparently logical and fits the traditional fee-for-service mindset, it is tempting to look at claims differences in the various service categories, such as inpatient, outpatient, primary care, specialists, drugs, and ancillaries, and attribute savings to the provider historically billing for same (that is, hospitals get "credit" for reduced hospital costs). However, a successful wellness, prevention, or lifestyle counseling program in a medical home may be the reason those patients never go to the hospital. The radiologist embedded in the medical home diagnostic team may have helped make an informed image analysis confirming a negative result and avoided those admissions. But, do use those service categories to set cost targets.
• Step 3: Individual attribution. We now know every provider group’s potential savings, but how do we determine the actual distribution based on actual results? Select metrics that are accurately associated with the desired individual and collective conduct of that provider class. They should cover both quality and efficiency. In the value-based reimbursement world, even if the performance is superb, if it is not measured appropriately, it will not be rewarded.
Once the proper metrics are selected, each provider’s performance is measured.
Keep it simple and open
Pick a few of the very best quality and efficiency metrics and have them and the data collection process thoroughly vetted by the providers. Following the guiding principles, the distribution model will be a success if: (1) everyone understands that this is the best practical approach, (2) the process has been open, and (3) everyone is acting in good faith to have as fair a shared savings distribution process as the current sophistication level of the ACO’s infrastructure allows. It cannot be viewed as coming from a "black box." For a young ACO, it will be crude, at best, in the beginning.
Conclusion
Even at this dawning of the movement to value-based reimbursement in health care, a framework for a fair merit-based shared savings distribution is available to all ACOs. As ACOs gain actual performance data, their health information technology capabilities improve, and refined quality and efficiency metrics emerge, the process will evolve from an open and good-faith application of the guiding principles with limited tools, to more and more refined determinations of the sources of the ACO’s quality and savings results. The path will get easier over time, but the destination is always clear – distribution in proportion to contribution.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author ([email protected] or 919-821-6612).
Our nation is in the midst of an inexorable shift in health care delivery from "pay for volume" to "pay for value." It is well documented that our current largely fee-for-service system is unsustainable and a dramatic incentive shift must occur. Every provider needs to be committed to providing the highest quality at the lowest cost. This is the fundamental goal of the pay-for-value system.
If quality and patient satisfaction criteria are met and providers working together in an accountable care organization or similar entity create savings for a defined patient population, then the ACO usually gets a portion of the savings, commonly 50%. Unlike capitated arrangements, shared savings arrangements can avoid or limit downside financial risk and therefore can serve as stepping-stones toward fuller accountability and incentives. They are quite appropriate for start-up and smaller ACOs.
The ACO gets the savings, if there are any. But what the ACO does with them is crucial to the success and sustainability of the organization. "ACOs must offer a realistic and achievable opportunity for providers to share in the savings created from delivering higher-value care. The incentive system must reward providers for delivering efficient care as opposed to the current volume-driven system" (The ACO Toolkit; the Dartmouth Institute, p. 9, Jan. 2011).
If providers or hospital stakeholders feel that their efforts to drive value are not being fairly recognized, they will no longer participate meaningfully, the goals of value-based medicine will be thwarted, and savings will not occur in the long-run. Before signing a participation contract, physicians should scrutinize how each ACO plans to distribute the savings it receives.
The Centers for Medicare and Medicaid Services administers the Medicare Shared Savings Program (MSSP). The fact that CMS’s regulations concerning MSSP are not prescriptive about a given savings distribution formula gives ACOs flexibility in this area. But the regulations are specific about the ultimate purpose of distributions: "As part of its application, an ACO must describe the following: (1) how it plans to use shared savings payments, including the criteria it plans to employ for distributing shared savings among its ACO participants and ACO providers/suppliers, ... and (3) how the proposed plan will achieve the general aims of better care for individuals, better health for populations, and lower growth in expenditures" (42 CFR 425.204(d), 76 Fed. Reg. 6798 [Nov. 2, 2011]).
Fatal flaw?
Some ACOs, however, have lost sight of the fact that failure to have a fair shared savings distribution formula (linking relative distributions to relative contributions) will be fatal to its sustainability. Some view them as "profits" to go to the owners or shareholders. Some simply lock in a fixed allocation similar to fee-for-service payment ratios, without regard to who generated the savings. Some employers of physicians have contracted to compensate only on a work production basis with zero performance incentive payments at all. Other ACOs are putting off the issue because it is sensitive culturally. As health care moves more and more to value-based compensation, the distribution of savings must be viewed primarily as the providers’ professional remuneration and not corporate "profit." Payments for administrative services and debt service must, of course, come out of the savings distribution to "keep the pump primed," but they should be carefully managed. The bulk must be distributed in proportion to contribution toward quality and cost-effective care.
One physician stated, "No physician is going to join an ACO when someone else is telling them what they are worth unless they know that the savings distribution formula is impeccably fair." To those putting off design of a fair merit-based compensation system until there is more physician buy-in, we respectfully submit that you cannot get buy-in without one.
A need for honed metrics
Yes, this concept is pretty basic when you think about it. But though it may be easy to understand, it can be complex to implement, especially when multiple specialists and facilities are involved in an ACO’s care coordination. One not only needs to determine the relative potential and actual value contribution for each provider, but also the clinically valid metrics by which to measure them. Under fee for service, metrics for success were usually transactional and objective (in other words, volume of procedure times rate). An ACO’s success metrics may be neither. Success may come from things not happening (that is, fewer ED visits, avoidable admissions, and reduced readmissions). At the same time, the distribution model needs to be clear, practical, and capable of being understood by all.
But there can be a replicable framework for any ACO to use to create a fair and sustainable shared savings distribution model. There are necessary subjective judgments – at this time, many metrics are imprecise or nonexistent – and the sophistication of the distribution process must parallel the sophistication of the ACO’s infrastructure. But, if the right people are involved and apply the ACO’s guiding principles on savings allocation, participants will be appropriately incentivized. The precision of distribution application will grow over time. Don’t let the perfect be the enemy of the good.
The six guiding principles for shared savings distribution
Though application will vary widely because of differing circumstances and types of initiatives, chances for success will increase if every activity can be judged by whether it is consistent with a set of guiding principles viewed as fair by the ACO members. You may want to consider a savings distribution formula with the following principles:
• Eyes on the prize: Triple Aim. It offers incentives for the delivery of high-quality and cost-effective care to achieve the Triple Aim – better care for individuals, better health for populations, and lower per capita costs.
• Broad provider input. It is the result of input from a diverse spectrum of knowledgeable providers who understand what drives patient population value.
• Fairness. It is fair to all in that it links relative distribution to relative contribution to the organization’s total savings and quality performance, and adheres to measurable clinically valid metrics.
• Transparency. It is clear, transparent, practical to implement and replicable.
• Constant evolution. It adapts and improves as the capabilities and experience as the ACO grows.
• Maximized incentive to drive value by all participants. After prudently meeting overhead costs, it allows gradual transition as well as commercially reasonable return on capital investment or debt service. It makes the most of ongoing incentive programs for all to deliver value by distributing as much of the savings surplus as possible to those who generate them.
Weighting: How to assign relative percentage among providers
As mentioned, it is important that design of a fair distribution formula be the product of collaboration among informed and committed clinicians who understand patient population management. Like virtually all organization compensation formulas, the determination of relative contributions of the different providers in a given ACO, or care initiative within the ACO, will involve a certain amount of inherent subjectivity but will be guided by weighted criteria applied in good faith.
• Step 1: Break down each initiative into its value-adding elements and assign provider responsibility for each. The ACO will have a number of different care management initiatives. Some, like outpatient diabetes management, may be completely the responsibility of one provider specialty, (that is, primary care). Others may involve coordination across multiple settings for patients with multiple conditions involving multiple specialties. Each initiative was chosen for a reason – to drive value. In setting relative potential distribution percentages, envision the perfect implementation of each initiative. Next, look at what tasks or best practices are needed to drive success, and then who is assigned responsibility for each.
• Step 2: Assign relative percentages to each specialty relative to its potential to realize savings. For a pure primary care prevention initiative, they would get 100% in all categories. For multispecialty initiatives, the percentage is tied to the proportion of those savings predicted to flow from that provider class.
N.B.: Historically, cost centers are not necessarily the cost savers. A mature ACO will be able to allocate savings to each initiative and the relative savings distribution within each. But for a start-up ACO, because it is so apparently logical and fits the traditional fee-for-service mindset, it is tempting to look at claims differences in the various service categories, such as inpatient, outpatient, primary care, specialists, drugs, and ancillaries, and attribute savings to the provider historically billing for same (that is, hospitals get "credit" for reduced hospital costs). However, a successful wellness, prevention, or lifestyle counseling program in a medical home may be the reason those patients never go to the hospital. The radiologist embedded in the medical home diagnostic team may have helped make an informed image analysis confirming a negative result and avoided those admissions. But, do use those service categories to set cost targets.
• Step 3: Individual attribution. We now know every provider group’s potential savings, but how do we determine the actual distribution based on actual results? Select metrics that are accurately associated with the desired individual and collective conduct of that provider class. They should cover both quality and efficiency. In the value-based reimbursement world, even if the performance is superb, if it is not measured appropriately, it will not be rewarded.
Once the proper metrics are selected, each provider’s performance is measured.
Keep it simple and open
Pick a few of the very best quality and efficiency metrics and have them and the data collection process thoroughly vetted by the providers. Following the guiding principles, the distribution model will be a success if: (1) everyone understands that this is the best practical approach, (2) the process has been open, and (3) everyone is acting in good faith to have as fair a shared savings distribution process as the current sophistication level of the ACO’s infrastructure allows. It cannot be viewed as coming from a "black box." For a young ACO, it will be crude, at best, in the beginning.
Conclusion
Even at this dawning of the movement to value-based reimbursement in health care, a framework for a fair merit-based shared savings distribution is available to all ACOs. As ACOs gain actual performance data, their health information technology capabilities improve, and refined quality and efficiency metrics emerge, the process will evolve from an open and good-faith application of the guiding principles with limited tools, to more and more refined determinations of the sources of the ACO’s quality and savings results. The path will get easier over time, but the destination is always clear – distribution in proportion to contribution.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author ([email protected] or 919-821-6612).
Our nation is in the midst of an inexorable shift in health care delivery from "pay for volume" to "pay for value." It is well documented that our current largely fee-for-service system is unsustainable and a dramatic incentive shift must occur. Every provider needs to be committed to providing the highest quality at the lowest cost. This is the fundamental goal of the pay-for-value system.
If quality and patient satisfaction criteria are met and providers working together in an accountable care organization or similar entity create savings for a defined patient population, then the ACO usually gets a portion of the savings, commonly 50%. Unlike capitated arrangements, shared savings arrangements can avoid or limit downside financial risk and therefore can serve as stepping-stones toward fuller accountability and incentives. They are quite appropriate for start-up and smaller ACOs.
The ACO gets the savings, if there are any. But what the ACO does with them is crucial to the success and sustainability of the organization. "ACOs must offer a realistic and achievable opportunity for providers to share in the savings created from delivering higher-value care. The incentive system must reward providers for delivering efficient care as opposed to the current volume-driven system" (The ACO Toolkit; the Dartmouth Institute, p. 9, Jan. 2011).
If providers or hospital stakeholders feel that their efforts to drive value are not being fairly recognized, they will no longer participate meaningfully, the goals of value-based medicine will be thwarted, and savings will not occur in the long-run. Before signing a participation contract, physicians should scrutinize how each ACO plans to distribute the savings it receives.
The Centers for Medicare and Medicaid Services administers the Medicare Shared Savings Program (MSSP). The fact that CMS’s regulations concerning MSSP are not prescriptive about a given savings distribution formula gives ACOs flexibility in this area. But the regulations are specific about the ultimate purpose of distributions: "As part of its application, an ACO must describe the following: (1) how it plans to use shared savings payments, including the criteria it plans to employ for distributing shared savings among its ACO participants and ACO providers/suppliers, ... and (3) how the proposed plan will achieve the general aims of better care for individuals, better health for populations, and lower growth in expenditures" (42 CFR 425.204(d), 76 Fed. Reg. 6798 [Nov. 2, 2011]).
Fatal flaw?
Some ACOs, however, have lost sight of the fact that failure to have a fair shared savings distribution formula (linking relative distributions to relative contributions) will be fatal to its sustainability. Some view them as "profits" to go to the owners or shareholders. Some simply lock in a fixed allocation similar to fee-for-service payment ratios, without regard to who generated the savings. Some employers of physicians have contracted to compensate only on a work production basis with zero performance incentive payments at all. Other ACOs are putting off the issue because it is sensitive culturally. As health care moves more and more to value-based compensation, the distribution of savings must be viewed primarily as the providers’ professional remuneration and not corporate "profit." Payments for administrative services and debt service must, of course, come out of the savings distribution to "keep the pump primed," but they should be carefully managed. The bulk must be distributed in proportion to contribution toward quality and cost-effective care.
One physician stated, "No physician is going to join an ACO when someone else is telling them what they are worth unless they know that the savings distribution formula is impeccably fair." To those putting off design of a fair merit-based compensation system until there is more physician buy-in, we respectfully submit that you cannot get buy-in without one.
A need for honed metrics
Yes, this concept is pretty basic when you think about it. But though it may be easy to understand, it can be complex to implement, especially when multiple specialists and facilities are involved in an ACO’s care coordination. One not only needs to determine the relative potential and actual value contribution for each provider, but also the clinically valid metrics by which to measure them. Under fee for service, metrics for success were usually transactional and objective (in other words, volume of procedure times rate). An ACO’s success metrics may be neither. Success may come from things not happening (that is, fewer ED visits, avoidable admissions, and reduced readmissions). At the same time, the distribution model needs to be clear, practical, and capable of being understood by all.
But there can be a replicable framework for any ACO to use to create a fair and sustainable shared savings distribution model. There are necessary subjective judgments – at this time, many metrics are imprecise or nonexistent – and the sophistication of the distribution process must parallel the sophistication of the ACO’s infrastructure. But, if the right people are involved and apply the ACO’s guiding principles on savings allocation, participants will be appropriately incentivized. The precision of distribution application will grow over time. Don’t let the perfect be the enemy of the good.
The six guiding principles for shared savings distribution
Though application will vary widely because of differing circumstances and types of initiatives, chances for success will increase if every activity can be judged by whether it is consistent with a set of guiding principles viewed as fair by the ACO members. You may want to consider a savings distribution formula with the following principles:
• Eyes on the prize: Triple Aim. It offers incentives for the delivery of high-quality and cost-effective care to achieve the Triple Aim – better care for individuals, better health for populations, and lower per capita costs.
• Broad provider input. It is the result of input from a diverse spectrum of knowledgeable providers who understand what drives patient population value.
• Fairness. It is fair to all in that it links relative distribution to relative contribution to the organization’s total savings and quality performance, and adheres to measurable clinically valid metrics.
• Transparency. It is clear, transparent, practical to implement and replicable.
• Constant evolution. It adapts and improves as the capabilities and experience as the ACO grows.
• Maximized incentive to drive value by all participants. After prudently meeting overhead costs, it allows gradual transition as well as commercially reasonable return on capital investment or debt service. It makes the most of ongoing incentive programs for all to deliver value by distributing as much of the savings surplus as possible to those who generate them.
Weighting: How to assign relative percentage among providers
As mentioned, it is important that design of a fair distribution formula be the product of collaboration among informed and committed clinicians who understand patient population management. Like virtually all organization compensation formulas, the determination of relative contributions of the different providers in a given ACO, or care initiative within the ACO, will involve a certain amount of inherent subjectivity but will be guided by weighted criteria applied in good faith.
• Step 1: Break down each initiative into its value-adding elements and assign provider responsibility for each. The ACO will have a number of different care management initiatives. Some, like outpatient diabetes management, may be completely the responsibility of one provider specialty, (that is, primary care). Others may involve coordination across multiple settings for patients with multiple conditions involving multiple specialties. Each initiative was chosen for a reason – to drive value. In setting relative potential distribution percentages, envision the perfect implementation of each initiative. Next, look at what tasks or best practices are needed to drive success, and then who is assigned responsibility for each.
• Step 2: Assign relative percentages to each specialty relative to its potential to realize savings. For a pure primary care prevention initiative, they would get 100% in all categories. For multispecialty initiatives, the percentage is tied to the proportion of those savings predicted to flow from that provider class.
N.B.: Historically, cost centers are not necessarily the cost savers. A mature ACO will be able to allocate savings to each initiative and the relative savings distribution within each. But for a start-up ACO, because it is so apparently logical and fits the traditional fee-for-service mindset, it is tempting to look at claims differences in the various service categories, such as inpatient, outpatient, primary care, specialists, drugs, and ancillaries, and attribute savings to the provider historically billing for same (that is, hospitals get "credit" for reduced hospital costs). However, a successful wellness, prevention, or lifestyle counseling program in a medical home may be the reason those patients never go to the hospital. The radiologist embedded in the medical home diagnostic team may have helped make an informed image analysis confirming a negative result and avoided those admissions. But, do use those service categories to set cost targets.
• Step 3: Individual attribution. We now know every provider group’s potential savings, but how do we determine the actual distribution based on actual results? Select metrics that are accurately associated with the desired individual and collective conduct of that provider class. They should cover both quality and efficiency. In the value-based reimbursement world, even if the performance is superb, if it is not measured appropriately, it will not be rewarded.
Once the proper metrics are selected, each provider’s performance is measured.
Keep it simple and open
Pick a few of the very best quality and efficiency metrics and have them and the data collection process thoroughly vetted by the providers. Following the guiding principles, the distribution model will be a success if: (1) everyone understands that this is the best practical approach, (2) the process has been open, and (3) everyone is acting in good faith to have as fair a shared savings distribution process as the current sophistication level of the ACO’s infrastructure allows. It cannot be viewed as coming from a "black box." For a young ACO, it will be crude, at best, in the beginning.
Conclusion
Even at this dawning of the movement to value-based reimbursement in health care, a framework for a fair merit-based shared savings distribution is available to all ACOs. As ACOs gain actual performance data, their health information technology capabilities improve, and refined quality and efficiency metrics emerge, the process will evolve from an open and good-faith application of the guiding principles with limited tools, to more and more refined determinations of the sources of the ACO’s quality and savings results. The path will get easier over time, but the destination is always clear – distribution in proportion to contribution.
Mr. Bobbitt is a senior partner and head of the Health Law Group at the Smith Anderson law firm in Raleigh, N.C. He has many years’ experience assisting physicians form integrated delivery systems. He has spoken and written nationally to primary care physicians on the strategies and practicalities of forming or joining ACOs. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author ([email protected] or 919-821-6612).

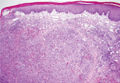
Angiolymphoid Hyperplasia With Eosinophilia
You have a big eyebrow!
One of my favorite Seinfeld episodes involves Elaine breaking up with a man who likes to mess with the minds of anyone who has the nerve to call it off with him. When Elaine tells him that they’re through, he says to her, "You know, you have a big head."
The rest of the show is devoted to Elaine trying to convince herself that she does not have a big head. In one scene, a cabbie tells the petite Elaine sitting in his back seat, "Please slide down, will you? You’re blocking the window!" And Elaine stands in Central Park in the show’s final scene, a bird flies right into her head as an old man says, "Well, I never saw that before. Looked like the bird just couldn’t get out of the way."
Jerry Seinfeld, who may have OCD-oid tendencies himself, often referred to dermatology in his sketches and showed insight into our patients and our clinical lives. How many people do we see who can’t stop thinking about some part of their appearance, often one we would never guess could be the focus of their attention: a small mole or freckle, a tiny wrinkle, a slight asymmetry in their features? Quite often, these patients become fixated on the feature not because they are "vain" or "narcissistic," and not because they have "body dysmorphic disorder," but just because someone else (and not necessarily somebody they were breaking up with who wanted to get even) pointed it out. From then on, they couldn’t stop thinking about it.
It may have been a doctor. ("That mole, has it been changing?") It may have been a friend. ("You know, the groove on the left side of your nose is deeper than the one on the right.") It may have been a hairdresser – it often is a hairdresser, who can see what you can’t. ("How long has that spot been up here?" Or, "Goodness! I can see right through to your scalp. Are you going bald?!")
Or it could be one of my favorite villains, the magnifying mirror, bane of presbyopic middle-age women. Overcoming presbyopia comes at the price of seeing every nevus as Pike’s Peak and every pore as the Grand Canyon.
In these cases, and many others like them, once the spots or defects are pointed out, people find it all but impossible to stop thinking about them and noticing them every time they look at themselves. If a bird flew by, it would probably slam right into them because it couldn’t get out of the way.
Removing what the patients are fixated on may be unnecessary, risky, or impossible. Advice to "just stop looking" may make sense, but can be unsatisfying or unacceptable.
I had a Seinfeld-esque moment the other day. Inga, thirtyish, came by to discuss acne, and then said, "Can you feel this growth at the end of my eyebrow?" My student and I palpated a small nodule under the outer aspect of her right eyebrow.
"It feels like a cyst," I said. "Probably been there a long time."
"Are you sure?" she asked. "Doesn’t it distort my face?"
We stepped back to a conversational distance. I couldn’t see anything, and neither could the student. "We can’t even see it from here," I told Inga. "What makes you think it distorts your face?"
"I was walking down the street with my mother and sister last week," she said, "and my mother said, "Inga, what is that on your eyebrow? Your whole face looks out of whack! And my sister said, ‘You’d better get that checked out.’"
My student and I stared at her. She was serious.
"Look," I said. "There is something there, but it’s definitely OK, and removing it would be unnecessary and leave a big scar. We honestly have no idea why your mother and sister would say that your face is lopsided when we can’t see anything even when we look for it."
Inga seemed mollified. We had to leave her, as we must leave all patients, to the vagaries of their own family dynamics. I can only hope that Inga doesn’t one day have some cabbie tell her to please lean to the left to keep the taxi from rolling over.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years.
One of my favorite Seinfeld episodes involves Elaine breaking up with a man who likes to mess with the minds of anyone who has the nerve to call it off with him. When Elaine tells him that they’re through, he says to her, "You know, you have a big head."
The rest of the show is devoted to Elaine trying to convince herself that she does not have a big head. In one scene, a cabbie tells the petite Elaine sitting in his back seat, "Please slide down, will you? You’re blocking the window!" And Elaine stands in Central Park in the show’s final scene, a bird flies right into her head as an old man says, "Well, I never saw that before. Looked like the bird just couldn’t get out of the way."
Jerry Seinfeld, who may have OCD-oid tendencies himself, often referred to dermatology in his sketches and showed insight into our patients and our clinical lives. How many people do we see who can’t stop thinking about some part of their appearance, often one we would never guess could be the focus of their attention: a small mole or freckle, a tiny wrinkle, a slight asymmetry in their features? Quite often, these patients become fixated on the feature not because they are "vain" or "narcissistic," and not because they have "body dysmorphic disorder," but just because someone else (and not necessarily somebody they were breaking up with who wanted to get even) pointed it out. From then on, they couldn’t stop thinking about it.
It may have been a doctor. ("That mole, has it been changing?") It may have been a friend. ("You know, the groove on the left side of your nose is deeper than the one on the right.") It may have been a hairdresser – it often is a hairdresser, who can see what you can’t. ("How long has that spot been up here?" Or, "Goodness! I can see right through to your scalp. Are you going bald?!")
Or it could be one of my favorite villains, the magnifying mirror, bane of presbyopic middle-age women. Overcoming presbyopia comes at the price of seeing every nevus as Pike’s Peak and every pore as the Grand Canyon.
In these cases, and many others like them, once the spots or defects are pointed out, people find it all but impossible to stop thinking about them and noticing them every time they look at themselves. If a bird flew by, it would probably slam right into them because it couldn’t get out of the way.
Removing what the patients are fixated on may be unnecessary, risky, or impossible. Advice to "just stop looking" may make sense, but can be unsatisfying or unacceptable.
I had a Seinfeld-esque moment the other day. Inga, thirtyish, came by to discuss acne, and then said, "Can you feel this growth at the end of my eyebrow?" My student and I palpated a small nodule under the outer aspect of her right eyebrow.
"It feels like a cyst," I said. "Probably been there a long time."
"Are you sure?" she asked. "Doesn’t it distort my face?"
We stepped back to a conversational distance. I couldn’t see anything, and neither could the student. "We can’t even see it from here," I told Inga. "What makes you think it distorts your face?"
"I was walking down the street with my mother and sister last week," she said, "and my mother said, "Inga, what is that on your eyebrow? Your whole face looks out of whack! And my sister said, ‘You’d better get that checked out.’"
My student and I stared at her. She was serious.
"Look," I said. "There is something there, but it’s definitely OK, and removing it would be unnecessary and leave a big scar. We honestly have no idea why your mother and sister would say that your face is lopsided when we can’t see anything even when we look for it."
Inga seemed mollified. We had to leave her, as we must leave all patients, to the vagaries of their own family dynamics. I can only hope that Inga doesn’t one day have some cabbie tell her to please lean to the left to keep the taxi from rolling over.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years.
One of my favorite Seinfeld episodes involves Elaine breaking up with a man who likes to mess with the minds of anyone who has the nerve to call it off with him. When Elaine tells him that they’re through, he says to her, "You know, you have a big head."
The rest of the show is devoted to Elaine trying to convince herself that she does not have a big head. In one scene, a cabbie tells the petite Elaine sitting in his back seat, "Please slide down, will you? You’re blocking the window!" And Elaine stands in Central Park in the show’s final scene, a bird flies right into her head as an old man says, "Well, I never saw that before. Looked like the bird just couldn’t get out of the way."
Jerry Seinfeld, who may have OCD-oid tendencies himself, often referred to dermatology in his sketches and showed insight into our patients and our clinical lives. How many people do we see who can’t stop thinking about some part of their appearance, often one we would never guess could be the focus of their attention: a small mole or freckle, a tiny wrinkle, a slight asymmetry in their features? Quite often, these patients become fixated on the feature not because they are "vain" or "narcissistic," and not because they have "body dysmorphic disorder," but just because someone else (and not necessarily somebody they were breaking up with who wanted to get even) pointed it out. From then on, they couldn’t stop thinking about it.
It may have been a doctor. ("That mole, has it been changing?") It may have been a friend. ("You know, the groove on the left side of your nose is deeper than the one on the right.") It may have been a hairdresser – it often is a hairdresser, who can see what you can’t. ("How long has that spot been up here?" Or, "Goodness! I can see right through to your scalp. Are you going bald?!")
Or it could be one of my favorite villains, the magnifying mirror, bane of presbyopic middle-age women. Overcoming presbyopia comes at the price of seeing every nevus as Pike’s Peak and every pore as the Grand Canyon.
In these cases, and many others like them, once the spots or defects are pointed out, people find it all but impossible to stop thinking about them and noticing them every time they look at themselves. If a bird flew by, it would probably slam right into them because it couldn’t get out of the way.
Removing what the patients are fixated on may be unnecessary, risky, or impossible. Advice to "just stop looking" may make sense, but can be unsatisfying or unacceptable.
I had a Seinfeld-esque moment the other day. Inga, thirtyish, came by to discuss acne, and then said, "Can you feel this growth at the end of my eyebrow?" My student and I palpated a small nodule under the outer aspect of her right eyebrow.
"It feels like a cyst," I said. "Probably been there a long time."
"Are you sure?" she asked. "Doesn’t it distort my face?"
We stepped back to a conversational distance. I couldn’t see anything, and neither could the student. "We can’t even see it from here," I told Inga. "What makes you think it distorts your face?"
"I was walking down the street with my mother and sister last week," she said, "and my mother said, "Inga, what is that on your eyebrow? Your whole face looks out of whack! And my sister said, ‘You’d better get that checked out.’"
My student and I stared at her. She was serious.
"Look," I said. "There is something there, but it’s definitely OK, and removing it would be unnecessary and leave a big scar. We honestly have no idea why your mother and sister would say that your face is lopsided when we can’t see anything even when we look for it."
Inga seemed mollified. We had to leave her, as we must leave all patients, to the vagaries of their own family dynamics. I can only hope that Inga doesn’t one day have some cabbie tell her to please lean to the left to keep the taxi from rolling over.
Dr. Rockoff practices dermatology in Brookline, Mass. He is on the clinical faculty at Tufts University School of Medicine, Boston, and has taught senior medical students and other trainees for 30 years.

Minimizing cancer’s impact on bone with denosumab: current and future perspectives
Bone metastasis is a serious complication of advanced cancer. It is most commonly observed in patients with metastatic breast and prostate cancers, but also occurs in most other metastatic solid cancers. Without treatment, patients may experience complications including intractable bone pain, hypercalcemia, fracture, spinal cord compression and/or a requirement for surgical or radiotherapeutic intervention. In 2010, denosumab, a fully human monoclonal antibody that inhibits RANK ligand (RANKL) and subsequent osteoclast-mediated bone destruction, was approved by the Food and Drug Administration for the prevention of skeletal-related events (SREs) in patients with bone metastases from solid tumors. This article reviews the role of denosumab in preventing SREs due to bone metastases, treating bone loss due to hormone-ablative cancer therapies, and describes denosumab’s safety profile and potential future indications under investigation.
Click on the PDF icon at the top of this introduction to read the full article.
Bone metastasis is a serious complication of advanced cancer. It is most commonly observed in patients with metastatic breast and prostate cancers, but also occurs in most other metastatic solid cancers. Without treatment, patients may experience complications including intractable bone pain, hypercalcemia, fracture, spinal cord compression and/or a requirement for surgical or radiotherapeutic intervention. In 2010, denosumab, a fully human monoclonal antibody that inhibits RANK ligand (RANKL) and subsequent osteoclast-mediated bone destruction, was approved by the Food and Drug Administration for the prevention of skeletal-related events (SREs) in patients with bone metastases from solid tumors. This article reviews the role of denosumab in preventing SREs due to bone metastases, treating bone loss due to hormone-ablative cancer therapies, and describes denosumab’s safety profile and potential future indications under investigation.
Click on the PDF icon at the top of this introduction to read the full article.
Bone metastasis is a serious complication of advanced cancer. It is most commonly observed in patients with metastatic breast and prostate cancers, but also occurs in most other metastatic solid cancers. Without treatment, patients may experience complications including intractable bone pain, hypercalcemia, fracture, spinal cord compression and/or a requirement for surgical or radiotherapeutic intervention. In 2010, denosumab, a fully human monoclonal antibody that inhibits RANK ligand (RANKL) and subsequent osteoclast-mediated bone destruction, was approved by the Food and Drug Administration for the prevention of skeletal-related events (SREs) in patients with bone metastases from solid tumors. This article reviews the role of denosumab in preventing SREs due to bone metastases, treating bone loss due to hormone-ablative cancer therapies, and describes denosumab’s safety profile and potential future indications under investigation.
Click on the PDF icon at the top of this introduction to read the full article.
Improving access with a collaborative approach to cancer genetic counseling services: a pilot study
Background Limited access to cancer genetic counselors (GC) may result in the lack of patient identification and/or failure to show due to travel distance and complicated treatment schedules.
Objective We hypothesized that access would improve when a GC collaborated with distant nongenetics health care providers to provide services locally.
Methods Patients at a collaborative site were offered a risk assessment survey that was reviewed remotely by a licensed, boardcertified GC. Patients were triaged such that the onsite registered nurse (RN) provided basic risk assessment and offered genetic testing for straight-forward hereditary breast and ovarian cases. Ongoing training and support was provided by the GC. Followup and complex cases were scheduled with the GC during a monthly outreach visit to the collaborative site.
Results During the 1-year study period, the total number of patients who accessed genetic counseling services from the target region was 4 times greater than the previous year. Ten of 17 patients who were triaged for genetic counseling and testing underwent genetic risk assessment services as a result of this identification and triage protocol.
Conclusion This defines a workable approach for patient identification and triage for hereditary cancer risk assessment and genetic counseling in a community setting. This collaborative approach may be applicable to centers that do not have access to a board-certified GC, especially important in light of the 2012 Commission on Cancer Standards that require cancer risk assessment, genetic counseling and testing services on site or by referral.
Click on the PDF icon at the top of this introduction to read the full article.
Background Limited access to cancer genetic counselors (GC) may result in the lack of patient identification and/or failure to show due to travel distance and complicated treatment schedules.
Objective We hypothesized that access would improve when a GC collaborated with distant nongenetics health care providers to provide services locally.
Methods Patients at a collaborative site were offered a risk assessment survey that was reviewed remotely by a licensed, boardcertified GC. Patients were triaged such that the onsite registered nurse (RN) provided basic risk assessment and offered genetic testing for straight-forward hereditary breast and ovarian cases. Ongoing training and support was provided by the GC. Followup and complex cases were scheduled with the GC during a monthly outreach visit to the collaborative site.
Results During the 1-year study period, the total number of patients who accessed genetic counseling services from the target region was 4 times greater than the previous year. Ten of 17 patients who were triaged for genetic counseling and testing underwent genetic risk assessment services as a result of this identification and triage protocol.
Conclusion This defines a workable approach for patient identification and triage for hereditary cancer risk assessment and genetic counseling in a community setting. This collaborative approach may be applicable to centers that do not have access to a board-certified GC, especially important in light of the 2012 Commission on Cancer Standards that require cancer risk assessment, genetic counseling and testing services on site or by referral.
Click on the PDF icon at the top of this introduction to read the full article.
Background Limited access to cancer genetic counselors (GC) may result in the lack of patient identification and/or failure to show due to travel distance and complicated treatment schedules.
Objective We hypothesized that access would improve when a GC collaborated with distant nongenetics health care providers to provide services locally.
Methods Patients at a collaborative site were offered a risk assessment survey that was reviewed remotely by a licensed, boardcertified GC. Patients were triaged such that the onsite registered nurse (RN) provided basic risk assessment and offered genetic testing for straight-forward hereditary breast and ovarian cases. Ongoing training and support was provided by the GC. Followup and complex cases were scheduled with the GC during a monthly outreach visit to the collaborative site.
Results During the 1-year study period, the total number of patients who accessed genetic counseling services from the target region was 4 times greater than the previous year. Ten of 17 patients who were triaged for genetic counseling and testing underwent genetic risk assessment services as a result of this identification and triage protocol.
Conclusion This defines a workable approach for patient identification and triage for hereditary cancer risk assessment and genetic counseling in a community setting. This collaborative approach may be applicable to centers that do not have access to a board-certified GC, especially important in light of the 2012 Commission on Cancer Standards that require cancer risk assessment, genetic counseling and testing services on site or by referral.
Click on the PDF icon at the top of this introduction to read the full article.
Locally advanced pancreatic cancer in a socio-economically challenged population
Background Locally advanced pancreatic cancer (LAPC) is associated with poor outcome, and clinical trials are imperative to address this. However, barriers to trial enrollment often exist, particularly in socio-economically challenged populations.
Objective To evaluate the outcome of socio-economically challenged patients who had LAPC, multiple comorbidities, and who were not enrolled on clinical trials, but who were treated with the best standard-of-care.
Methods We retrospectively reviewed the charts of 32 patients diagnosed as having LAPC who were referred to an urban cancer center between 2005 and 2010, analyzing the treatment and outcomes of 19 who underwent treatment at our center.
Results In all 26.3% of the analyzed patients had commercial insurance, 31.6% did not identify English as their preferred language, and 84.2% had 3 or more comorbidities. The median overall survival was 19.1 months, with estimated 1- and 2-year survivals of 60.8% and 36.5%, respectively. The median survival for patients receiving chemotherapy followed by chemoradiation was 26.6 months. Toxicities were controllable. Translation services were required by 26% and social services interventions by 84%. Survival analysis based on insurance coverage did not show a significant association with levels of reimbursement.
Limitations Retrospective study, small sample size, differences in chemotherapy types.
Conclusions These patients, representative of a diverse and socio-economically challenged community, were able to receive standard-of-care therapies with acceptable toxicity and to achieve survivals comparable with clinical trials. This was achieved with intense supportive services.
Click on the PDF icon at the top of this introduction to read the full article.
Background Locally advanced pancreatic cancer (LAPC) is associated with poor outcome, and clinical trials are imperative to address this. However, barriers to trial enrollment often exist, particularly in socio-economically challenged populations.
Objective To evaluate the outcome of socio-economically challenged patients who had LAPC, multiple comorbidities, and who were not enrolled on clinical trials, but who were treated with the best standard-of-care.
Methods We retrospectively reviewed the charts of 32 patients diagnosed as having LAPC who were referred to an urban cancer center between 2005 and 2010, analyzing the treatment and outcomes of 19 who underwent treatment at our center.
Results In all 26.3% of the analyzed patients had commercial insurance, 31.6% did not identify English as their preferred language, and 84.2% had 3 or more comorbidities. The median overall survival was 19.1 months, with estimated 1- and 2-year survivals of 60.8% and 36.5%, respectively. The median survival for patients receiving chemotherapy followed by chemoradiation was 26.6 months. Toxicities were controllable. Translation services were required by 26% and social services interventions by 84%. Survival analysis based on insurance coverage did not show a significant association with levels of reimbursement.
Limitations Retrospective study, small sample size, differences in chemotherapy types.
Conclusions These patients, representative of a diverse and socio-economically challenged community, were able to receive standard-of-care therapies with acceptable toxicity and to achieve survivals comparable with clinical trials. This was achieved with intense supportive services.
Click on the PDF icon at the top of this introduction to read the full article.
Background Locally advanced pancreatic cancer (LAPC) is associated with poor outcome, and clinical trials are imperative to address this. However, barriers to trial enrollment often exist, particularly in socio-economically challenged populations.
Objective To evaluate the outcome of socio-economically challenged patients who had LAPC, multiple comorbidities, and who were not enrolled on clinical trials, but who were treated with the best standard-of-care.
Methods We retrospectively reviewed the charts of 32 patients diagnosed as having LAPC who were referred to an urban cancer center between 2005 and 2010, analyzing the treatment and outcomes of 19 who underwent treatment at our center.
Results In all 26.3% of the analyzed patients had commercial insurance, 31.6% did not identify English as their preferred language, and 84.2% had 3 or more comorbidities. The median overall survival was 19.1 months, with estimated 1- and 2-year survivals of 60.8% and 36.5%, respectively. The median survival for patients receiving chemotherapy followed by chemoradiation was 26.6 months. Toxicities were controllable. Translation services were required by 26% and social services interventions by 84%. Survival analysis based on insurance coverage did not show a significant association with levels of reimbursement.
Limitations Retrospective study, small sample size, differences in chemotherapy types.
Conclusions These patients, representative of a diverse and socio-economically challenged community, were able to receive standard-of-care therapies with acceptable toxicity and to achieve survivals comparable with clinical trials. This was achieved with intense supportive services.
Click on the PDF icon at the top of this introduction to read the full article.
Plasma product now available in US

Credit: Cristina Granados
A pooled plasma product that was approved by the Food and Drug Administration in January is now available for use in the US.
The product, called Octaplas, is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma is collected from US donors who have been screened and tested for diseases transmitted by blood.
Octaplas is indicated for the replacement of multiple coagulation
factors in patients with acquired deficiencies due to liver disease or
undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura.
Octaplas is contraindicated in patients with IgA deficiency, severe deficiency of protein S, a history of hypersensitivity to fresh-frozen plasma or plasma-derived products including any plasma protein, or a history of hypersensitivity reaction to Octaplas.
Transfusion reactions can occur with ABO blood group mismatches. High infusion rates can induce hypervolemia with consequent pulmonary edema or cardiac failure.
Excessive bleeding due to hyperfibrinolysis can occur due to low levels of alpha2-antiplasmin. Thrombosis can occur due to low levels of protein S, and citrate toxicity can occur with volumes exceeding 1 mL of Octaplas per kg per minute.
Because Octaplas is made from human plasma, it may carry the risk of transmitting infectious agents; for instance, the variant Creutzfeldt-Jakob disease agent.
Administering Octaplas
Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of the product is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12 to 15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
To order Octaplas, call your local Blood Center or National Hospital Specialties at 800-344-6087. To request product information, call 201-604-1130.
For prescribing information, visit www.octaplasus.com. Octaplas is manufactured by Octapharma USA. ![]()
Credit: Cristina Granados
A pooled plasma product that was approved by the Food and Drug Administration in January is now available for use in the US.
The product, called Octaplas, is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma is collected from US donors who have been screened and tested for diseases transmitted by blood.
Octaplas is indicated for the replacement of multiple coagulation
factors in patients with acquired deficiencies due to liver disease or
undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura.
Octaplas is contraindicated in patients with IgA deficiency, severe deficiency of protein S, a history of hypersensitivity to fresh-frozen plasma or plasma-derived products including any plasma protein, or a history of hypersensitivity reaction to Octaplas.
Transfusion reactions can occur with ABO blood group mismatches. High infusion rates can induce hypervolemia with consequent pulmonary edema or cardiac failure.
Excessive bleeding due to hyperfibrinolysis can occur due to low levels of alpha2-antiplasmin. Thrombosis can occur due to low levels of protein S, and citrate toxicity can occur with volumes exceeding 1 mL of Octaplas per kg per minute.
Because Octaplas is made from human plasma, it may carry the risk of transmitting infectious agents; for instance, the variant Creutzfeldt-Jakob disease agent.
Administering Octaplas
Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of the product is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12 to 15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
To order Octaplas, call your local Blood Center or National Hospital Specialties at 800-344-6087. To request product information, call 201-604-1130.
For prescribing information, visit www.octaplasus.com. Octaplas is manufactured by Octapharma USA. ![]()
Credit: Cristina Granados
A pooled plasma product that was approved by the Food and Drug Administration in January is now available for use in the US.
The product, called Octaplas, is a sterile, frozen solution of human plasma from several donors that has been treated with a solvent detergent process to minimize the risk of serious virus transmission.
The plasma is collected from US donors who have been screened and tested for diseases transmitted by blood.
Octaplas is indicated for the replacement of multiple coagulation
factors in patients with acquired deficiencies due to liver disease or
undergoing cardiac surgery or liver transplant. Octaplas can also be
used for plasma exchange in patients with thrombotic thrombocytopenic purpura.
Octaplas is contraindicated in patients with IgA deficiency, severe deficiency of protein S, a history of hypersensitivity to fresh-frozen plasma or plasma-derived products including any plasma protein, or a history of hypersensitivity reaction to Octaplas.
Transfusion reactions can occur with ABO blood group mismatches. High infusion rates can induce hypervolemia with consequent pulmonary edema or cardiac failure.
Excessive bleeding due to hyperfibrinolysis can occur due to low levels of alpha2-antiplasmin. Thrombosis can occur due to low levels of protein S, and citrate toxicity can occur with volumes exceeding 1 mL of Octaplas per kg per minute.
Because Octaplas is made from human plasma, it may carry the risk of transmitting infectious agents; for instance, the variant Creutzfeldt-Jakob disease agent.
Administering Octaplas
Octaplas should be matched to the recipient’s blood group to help avoid transfusion reactions. Each lot of the product is tested for composition of key clotting factors and is only released if the levels are within acceptable ranges.
The product is administered by intravenous infusion after thawing, using an infusion set with a filter. An aseptic technique must be used throughout the infusion.
The dosage depends upon the clinical situation and the underlying disorder. But 12 to 15 mL/kg of body weight is a generally accepted starting dose, and it should increase the patient’s plasma coagulation factor levels by about 25%.
It is important to monitor patient response, both clinically and with measurement of prothrombin time, partial thromboplastin time, and/or specific coagulation factor assays.
To order Octaplas, call your local Blood Center or National Hospital Specialties at 800-344-6087. To request product information, call 201-604-1130.
For prescribing information, visit www.octaplasus.com. Octaplas is manufactured by Octapharma USA. ![]()
New drug stacks up well against warfarin

Image by Kevin MacKenzie
AMSTERDAM—The oral anticoagulant edoxaban compares favorably with warfarin as treatment for recurrent venous thromboembolism (VTE), according to results of the Hokusai-VTE trial.
Edoxaban given after initial low molecular weight heparin (LMWH) proved equally as effective as warfarin given after LMWH.
And patients treated with edoxaban were less likely to experience clinically relevant bleeding than patients who received warfarin.
Results of the trial also offer new insight into a previously under-represented subgroup of patients with pulmonary embolism (PE), suggesting that treatment for this group might need to be different than for other VTE patients, said lead investigator Harry R. Büller, MD, of the Academic Medical Center in Amsterdam.
Dr Büller presented these findings at the 2013 European Society of Cardiology Congress, which is taking place August 31 through September 4. The study was also published in NEJM on September 1.
“What makes this study unique is new insight that there are subgroups in which we might need to revisit what we currently think about the treatment of VTE,” Dr Büller said.
The Hokusai-VTE trial included a broad spectrum of VTE patients, including a large subgroup (30%) of patients with PE and right ventricular dysfunction, and another subgroup (20%) at high risk for bleeding due to renal impairment and low body weight.
In total, 4921 patients with deep vein thrombosis and 3319 with PE received initial subcutaneous LMWH therapy and were then randomized to receive edoxaban or warfarin daily for 3 to 12 months.
Patients at a higher risk for bleeding—ie, those with creatinine clearance of 30 to 50 mL/min or body weight below 60 kg—received 30 mg of edoxaban. The rest of the patients in the edoxaban arm received 60 mg. Warfarin patients were dosed according to standard of care.
Overall, edoxaban proved as effective as warfarin. Recurrent symptomatic VTE occurred in 3.2% and 3.5% of patients, respectively (P<0.001 for noninferiority).
However, in the subgroup of patients with PE and evidence of right ventricular dysfunction, efficacy was superior with edoxaban—3.3% and 6.2%, respectively.
Edoxaban proved superior when it came to the primary safety outcome as well. Clinically relevant bleeding occurred in 8.5% of edoxaban-treated patients and 10.3% of warfarin-treated patients (P=0.004 for superiority).
In the edoxaban arm, there were 2 fatal bleeds and 13 non-fatal bleeds in a critical site. With warfarin, there were 10 fatal bleeds and 25 non-fatal bleeds in a critical site.
“By halving the daily dose of edoxaban to 30 mg [among patients at high risk of bleeding], efficacy was maintained, with significantly less bleeding than observed in the warfarin group,” Dr Büller said.
In this high-risk subgroup, clinically relevant bleeding occurred in 7.9% of those treated with edoxaban, compared to 12.8% of those treated with warfarin. And recurrent symptomatic VTE occurred in 3.0% and 4.2%, respectively.
Previous trials of oral anticoagulants have not identified these specific subgroups, Dr Büller said.
“Our findings are likely to be generalizable in a global setting,” he added. “We included patients with both provoked and unprovoked venous thromboembolism, and treatment durations varied from 3 to 12 months at the discretion of the treating physician.”
This study was supported by Daiichi Sankyo, the company developing edoxaban. ![]()
Image by Kevin MacKenzie
AMSTERDAM—The oral anticoagulant edoxaban compares favorably with warfarin as treatment for recurrent venous thromboembolism (VTE), according to results of the Hokusai-VTE trial.
Edoxaban given after initial low molecular weight heparin (LMWH) proved equally as effective as warfarin given after LMWH.
And patients treated with edoxaban were less likely to experience clinically relevant bleeding than patients who received warfarin.
Results of the trial also offer new insight into a previously under-represented subgroup of patients with pulmonary embolism (PE), suggesting that treatment for this group might need to be different than for other VTE patients, said lead investigator Harry R. Büller, MD, of the Academic Medical Center in Amsterdam.
Dr Büller presented these findings at the 2013 European Society of Cardiology Congress, which is taking place August 31 through September 4. The study was also published in NEJM on September 1.
“What makes this study unique is new insight that there are subgroups in which we might need to revisit what we currently think about the treatment of VTE,” Dr Büller said.
The Hokusai-VTE trial included a broad spectrum of VTE patients, including a large subgroup (30%) of patients with PE and right ventricular dysfunction, and another subgroup (20%) at high risk for bleeding due to renal impairment and low body weight.
In total, 4921 patients with deep vein thrombosis and 3319 with PE received initial subcutaneous LMWH therapy and were then randomized to receive edoxaban or warfarin daily for 3 to 12 months.
Patients at a higher risk for bleeding—ie, those with creatinine clearance of 30 to 50 mL/min or body weight below 60 kg—received 30 mg of edoxaban. The rest of the patients in the edoxaban arm received 60 mg. Warfarin patients were dosed according to standard of care.
Overall, edoxaban proved as effective as warfarin. Recurrent symptomatic VTE occurred in 3.2% and 3.5% of patients, respectively (P<0.001 for noninferiority).
However, in the subgroup of patients with PE and evidence of right ventricular dysfunction, efficacy was superior with edoxaban—3.3% and 6.2%, respectively.
Edoxaban proved superior when it came to the primary safety outcome as well. Clinically relevant bleeding occurred in 8.5% of edoxaban-treated patients and 10.3% of warfarin-treated patients (P=0.004 for superiority).
In the edoxaban arm, there were 2 fatal bleeds and 13 non-fatal bleeds in a critical site. With warfarin, there were 10 fatal bleeds and 25 non-fatal bleeds in a critical site.
“By halving the daily dose of edoxaban to 30 mg [among patients at high risk of bleeding], efficacy was maintained, with significantly less bleeding than observed in the warfarin group,” Dr Büller said.
In this high-risk subgroup, clinically relevant bleeding occurred in 7.9% of those treated with edoxaban, compared to 12.8% of those treated with warfarin. And recurrent symptomatic VTE occurred in 3.0% and 4.2%, respectively.
Previous trials of oral anticoagulants have not identified these specific subgroups, Dr Büller said.
“Our findings are likely to be generalizable in a global setting,” he added. “We included patients with both provoked and unprovoked venous thromboembolism, and treatment durations varied from 3 to 12 months at the discretion of the treating physician.”
This study was supported by Daiichi Sankyo, the company developing edoxaban. ![]()
Image by Kevin MacKenzie
AMSTERDAM—The oral anticoagulant edoxaban compares favorably with warfarin as treatment for recurrent venous thromboembolism (VTE), according to results of the Hokusai-VTE trial.
Edoxaban given after initial low molecular weight heparin (LMWH) proved equally as effective as warfarin given after LMWH.
And patients treated with edoxaban were less likely to experience clinically relevant bleeding than patients who received warfarin.
Results of the trial also offer new insight into a previously under-represented subgroup of patients with pulmonary embolism (PE), suggesting that treatment for this group might need to be different than for other VTE patients, said lead investigator Harry R. Büller, MD, of the Academic Medical Center in Amsterdam.
Dr Büller presented these findings at the 2013 European Society of Cardiology Congress, which is taking place August 31 through September 4. The study was also published in NEJM on September 1.
“What makes this study unique is new insight that there are subgroups in which we might need to revisit what we currently think about the treatment of VTE,” Dr Büller said.
The Hokusai-VTE trial included a broad spectrum of VTE patients, including a large subgroup (30%) of patients with PE and right ventricular dysfunction, and another subgroup (20%) at high risk for bleeding due to renal impairment and low body weight.
In total, 4921 patients with deep vein thrombosis and 3319 with PE received initial subcutaneous LMWH therapy and were then randomized to receive edoxaban or warfarin daily for 3 to 12 months.
Patients at a higher risk for bleeding—ie, those with creatinine clearance of 30 to 50 mL/min or body weight below 60 kg—received 30 mg of edoxaban. The rest of the patients in the edoxaban arm received 60 mg. Warfarin patients were dosed according to standard of care.
Overall, edoxaban proved as effective as warfarin. Recurrent symptomatic VTE occurred in 3.2% and 3.5% of patients, respectively (P<0.001 for noninferiority).
However, in the subgroup of patients with PE and evidence of right ventricular dysfunction, efficacy was superior with edoxaban—3.3% and 6.2%, respectively.
Edoxaban proved superior when it came to the primary safety outcome as well. Clinically relevant bleeding occurred in 8.5% of edoxaban-treated patients and 10.3% of warfarin-treated patients (P=0.004 for superiority).
In the edoxaban arm, there were 2 fatal bleeds and 13 non-fatal bleeds in a critical site. With warfarin, there were 10 fatal bleeds and 25 non-fatal bleeds in a critical site.
“By halving the daily dose of edoxaban to 30 mg [among patients at high risk of bleeding], efficacy was maintained, with significantly less bleeding than observed in the warfarin group,” Dr Büller said.
In this high-risk subgroup, clinically relevant bleeding occurred in 7.9% of those treated with edoxaban, compared to 12.8% of those treated with warfarin. And recurrent symptomatic VTE occurred in 3.0% and 4.2%, respectively.
Previous trials of oral anticoagulants have not identified these specific subgroups, Dr Büller said.
“Our findings are likely to be generalizable in a global setting,” he added. “We included patients with both provoked and unprovoked venous thromboembolism, and treatment durations varied from 3 to 12 months at the discretion of the treating physician.”
This study was supported by Daiichi Sankyo, the company developing edoxaban. ![]()
Building patient-centered care through values assessment integration with advance care planning
Oncologists frequently have to make diagnoses that portend bad outcomes and difficulties in management, among them, for stage IV lung or pancreatic cancer. Many recent studies have shown the importance of appropriate implementation of palliative care and the need for discussing with the patient the goals of treatment early in diagnosis.1-3
Click on the PDF icon at the top of this introduction to read the full article.
Oncologists frequently have to make diagnoses that portend bad outcomes and difficulties in management, among them, for stage IV lung or pancreatic cancer. Many recent studies have shown the importance of appropriate implementation of palliative care and the need for discussing with the patient the goals of treatment early in diagnosis.1-3
Click on the PDF icon at the top of this introduction to read the full article.
Oncologists frequently have to make diagnoses that portend bad outcomes and difficulties in management, among them, for stage IV lung or pancreatic cancer. Many recent studies have shown the importance of appropriate implementation of palliative care and the need for discussing with the patient the goals of treatment early in diagnosis.1-3
Click on the PDF icon at the top of this introduction to read the full article.
Three Factors Tied to Femoral Artery Aneurysm Outcomes
SAN FRANCISCO - Predictors of acute aneurysm - related complications were aneurysm size of 4 cm or greater, thrombus, and age younger than 60 years, in a study of patients with isolated degenerative femoral artery aneurysms.
"Acute complications have not occurred in patients with FAAs less than 3.5 cm, suggesting that this should be adopted as a new threshold for elective repair," Dr. Gustavo S. Oderich said at the Society for Vascular Surgery Annual Meeting.
Femoral artery aneurysms (FAAs) are rare, affecting 5/100,000 individuals, said Dr. Oderich, a vascular surgeon who practices at the Mayo Clinic, Rochester, Minn. Current indications for repair are symptoms, size greater than 2.5 cm, growth, and thrombus.
Most reports of FAAs predate modern imaging. These studies "are limited by the small number of patients, mixed etiology, and short follow-up," Dr. Oderich said. "The purpose of the current study was to review the clinical presentation, management strategies, and outcomes of degenerative FAAs in a larger cohort of patients."

For the study, led by Dr. Peter F. Lawrence of the University of California, Los Angeles, researchers retrospectively studied patients treated for degenerative FAAs between 2002 and 2012 at eight medical centers in the United States. Iatrogenic, anastomotic, and mycotic aneurysms were excluded from the analysis. Endpoints of interest were morbidity and mortality with operative repair; acute aneurysm - related complications including rupture, thrombosis, and embolization; and patient survival.
Dr. Oderich reported on 236 FAAs that occurred in 182 patients. The mean size was 32 cm. Most (81%) were located on the common femoral artery, 14% were located on the superficial femoral artery, and 5% were located on the profunda femoris artery. The majority of patients (88%) had synchronous aneurysms in other locations. The most common locations outside of the femoral artery were the aortic (62%) artery, common iliac arteries (60%), popliteal arteries (47%), and bilateral FAAs (25%).
The mean age of patients was 73 and 94% of patients were male. At presentation 63% of patients were asymptomatic. The most common signs and symptoms were palpable mass (29%), claudication (22%), and local pain (10%).
When the researchers compared symptomatic versus asymptomatic aneurysms, symptomatic aneurysms were larger, had more intraluminal thrombus, and more often affected the profunda femoral artery .Only 12 patients (5%) had acute events, most of them rupture or thrombosis, with a size of 3.5-7 cm in range.
Independent predictors associated with acute aneurysm - related complications were a diameter of 4 cm or greater (P = less than .001), an intraluminal thrombus (P = less than .001), and age younger than 60 (P = .004). Freedom from repair among patients with asymptomatic FAAs was 21% at 5 years, "largely reflecting our practice of indicating the operation for aneurysms greater than 2.5 cm," Dr. Oderich said. The most common indications for repair were pain (34%), intramural thrombus (27%), and size of 2.5 cm or greater (23%).
He reported that 138 patients underwent open repair and 3 patients underwent endovascular treatment of 177 FAAs. The most frequent form of reconstruction was an interposition graft (80%) or bypass (20%). Among the 141 patients who had operative treatment, the 30-day mortality was 1.5%, the morbidity rate was 20%, and the mean length of stay was 7 days. During a mean follow-up of 49 months, there were 35 nonaneurysm-related deaths (27%) and 1 graft-related complication. Patient survival at 5 years was 61%.
"Repair of smaller FAAs may be indicated in patients with intramural thrombus or progressive enlargement," Dr. Oderich concluded. "Current repair of all symptomatic FAAs should remain unchanged. Operative repair was associated with low mortality, morbidity, and durable results."
Decision making when faced with a patient with a degenerative femoral artery aneurysm has always been based on small series. Especially when deciding what size asymptomatic aneurysm is too big to continue to watch, the available data are weak.
The authors pooled a large number of cases from eight institutions to assemble a dataset of 236 FAAs, 25% of which were apparently observed without repair. (Disclaimer: One of my partners contributed data to this series.) They noted that no asymptomatic aneurysm less than 3.5 cm developed an acute complication, and concluded that the threshold for repair of these lesions should rise to at least 3.5 cm in diameter.
Although this report is retrospective and almost certainly contains selection bias, this conclusion seems valid to me at a gut level. I also agree that any symptoms or the presence of significant mural thrombus should prompt repair. Until we are able to capitalize on the capacity of electronic medical records to determine the clinical outcome of patients on the basis of diagnosis rather than what surgical procedure they have had, this is probably the best data we are likely to see regarding the management of FAA.
Dr. Larry W. Kraiss is professor and chief of vascular surgery at the University of Utah, Salt Lake City, and is an associate medical editor of Vascular Specialist.
Decision making when faced with a patient with a degenerative femoral artery aneurysm has always been based on small series. Especially when deciding what size asymptomatic aneurysm is too big to continue to watch, the available data are weak.
The authors pooled a large number of cases from eight institutions to assemble a dataset of 236 FAAs, 25% of which were apparently observed without repair. (Disclaimer: One of my partners contributed data to this series.) They noted that no asymptomatic aneurysm less than 3.5 cm developed an acute complication, and concluded that the threshold for repair of these lesions should rise to at least 3.5 cm in diameter.
Although this report is retrospective and almost certainly contains selection bias, this conclusion seems valid to me at a gut level. I also agree that any symptoms or the presence of significant mural thrombus should prompt repair. Until we are able to capitalize on the capacity of electronic medical records to determine the clinical outcome of patients on the basis of diagnosis rather than what surgical procedure they have had, this is probably the best data we are likely to see regarding the management of FAA.
Dr. Larry W. Kraiss is professor and chief of vascular surgery at the University of Utah, Salt Lake City, and is an associate medical editor of Vascular Specialist.
Decision making when faced with a patient with a degenerative femoral artery aneurysm has always been based on small series. Especially when deciding what size asymptomatic aneurysm is too big to continue to watch, the available data are weak.
The authors pooled a large number of cases from eight institutions to assemble a dataset of 236 FAAs, 25% of which were apparently observed without repair. (Disclaimer: One of my partners contributed data to this series.) They noted that no asymptomatic aneurysm less than 3.5 cm developed an acute complication, and concluded that the threshold for repair of these lesions should rise to at least 3.5 cm in diameter.
Although this report is retrospective and almost certainly contains selection bias, this conclusion seems valid to me at a gut level. I also agree that any symptoms or the presence of significant mural thrombus should prompt repair. Until we are able to capitalize on the capacity of electronic medical records to determine the clinical outcome of patients on the basis of diagnosis rather than what surgical procedure they have had, this is probably the best data we are likely to see regarding the management of FAA.
Dr. Larry W. Kraiss is professor and chief of vascular surgery at the University of Utah, Salt Lake City, and is an associate medical editor of Vascular Specialist.
SAN FRANCISCO - Predictors of acute aneurysm - related complications were aneurysm size of 4 cm or greater, thrombus, and age younger than 60 years, in a study of patients with isolated degenerative femoral artery aneurysms.
"Acute complications have not occurred in patients with FAAs less than 3.5 cm, suggesting that this should be adopted as a new threshold for elective repair," Dr. Gustavo S. Oderich said at the Society for Vascular Surgery Annual Meeting.
Femoral artery aneurysms (FAAs) are rare, affecting 5/100,000 individuals, said Dr. Oderich, a vascular surgeon who practices at the Mayo Clinic, Rochester, Minn. Current indications for repair are symptoms, size greater than 2.5 cm, growth, and thrombus.
Most reports of FAAs predate modern imaging. These studies "are limited by the small number of patients, mixed etiology, and short follow-up," Dr. Oderich said. "The purpose of the current study was to review the clinical presentation, management strategies, and outcomes of degenerative FAAs in a larger cohort of patients."
For the study, led by Dr. Peter F. Lawrence of the University of California, Los Angeles, researchers retrospectively studied patients treated for degenerative FAAs between 2002 and 2012 at eight medical centers in the United States. Iatrogenic, anastomotic, and mycotic aneurysms were excluded from the analysis. Endpoints of interest were morbidity and mortality with operative repair; acute aneurysm - related complications including rupture, thrombosis, and embolization; and patient survival.
Dr. Oderich reported on 236 FAAs that occurred in 182 patients. The mean size was 32 cm. Most (81%) were located on the common femoral artery, 14% were located on the superficial femoral artery, and 5% were located on the profunda femoris artery. The majority of patients (88%) had synchronous aneurysms in other locations. The most common locations outside of the femoral artery were the aortic (62%) artery, common iliac arteries (60%), popliteal arteries (47%), and bilateral FAAs (25%).
The mean age of patients was 73 and 94% of patients were male. At presentation 63% of patients were asymptomatic. The most common signs and symptoms were palpable mass (29%), claudication (22%), and local pain (10%).
When the researchers compared symptomatic versus asymptomatic aneurysms, symptomatic aneurysms were larger, had more intraluminal thrombus, and more often affected the profunda femoral artery .Only 12 patients (5%) had acute events, most of them rupture or thrombosis, with a size of 3.5-7 cm in range.
Independent predictors associated with acute aneurysm - related complications were a diameter of 4 cm or greater (P = less than .001), an intraluminal thrombus (P = less than .001), and age younger than 60 (P = .004). Freedom from repair among patients with asymptomatic FAAs was 21% at 5 years, "largely reflecting our practice of indicating the operation for aneurysms greater than 2.5 cm," Dr. Oderich said. The most common indications for repair were pain (34%), intramural thrombus (27%), and size of 2.5 cm or greater (23%).
He reported that 138 patients underwent open repair and 3 patients underwent endovascular treatment of 177 FAAs. The most frequent form of reconstruction was an interposition graft (80%) or bypass (20%). Among the 141 patients who had operative treatment, the 30-day mortality was 1.5%, the morbidity rate was 20%, and the mean length of stay was 7 days. During a mean follow-up of 49 months, there were 35 nonaneurysm-related deaths (27%) and 1 graft-related complication. Patient survival at 5 years was 61%.
"Repair of smaller FAAs may be indicated in patients with intramural thrombus or progressive enlargement," Dr. Oderich concluded. "Current repair of all symptomatic FAAs should remain unchanged. Operative repair was associated with low mortality, morbidity, and durable results."
SAN FRANCISCO - Predictors of acute aneurysm - related complications were aneurysm size of 4 cm or greater, thrombus, and age younger than 60 years, in a study of patients with isolated degenerative femoral artery aneurysms.
"Acute complications have not occurred in patients with FAAs less than 3.5 cm, suggesting that this should be adopted as a new threshold for elective repair," Dr. Gustavo S. Oderich said at the Society for Vascular Surgery Annual Meeting.
Femoral artery aneurysms (FAAs) are rare, affecting 5/100,000 individuals, said Dr. Oderich, a vascular surgeon who practices at the Mayo Clinic, Rochester, Minn. Current indications for repair are symptoms, size greater than 2.5 cm, growth, and thrombus.
Most reports of FAAs predate modern imaging. These studies "are limited by the small number of patients, mixed etiology, and short follow-up," Dr. Oderich said. "The purpose of the current study was to review the clinical presentation, management strategies, and outcomes of degenerative FAAs in a larger cohort of patients."
For the study, led by Dr. Peter F. Lawrence of the University of California, Los Angeles, researchers retrospectively studied patients treated for degenerative FAAs between 2002 and 2012 at eight medical centers in the United States. Iatrogenic, anastomotic, and mycotic aneurysms were excluded from the analysis. Endpoints of interest were morbidity and mortality with operative repair; acute aneurysm - related complications including rupture, thrombosis, and embolization; and patient survival.
Dr. Oderich reported on 236 FAAs that occurred in 182 patients. The mean size was 32 cm. Most (81%) were located on the common femoral artery, 14% were located on the superficial femoral artery, and 5% were located on the profunda femoris artery. The majority of patients (88%) had synchronous aneurysms in other locations. The most common locations outside of the femoral artery were the aortic (62%) artery, common iliac arteries (60%), popliteal arteries (47%), and bilateral FAAs (25%).
The mean age of patients was 73 and 94% of patients were male. At presentation 63% of patients were asymptomatic. The most common signs and symptoms were palpable mass (29%), claudication (22%), and local pain (10%).
When the researchers compared symptomatic versus asymptomatic aneurysms, symptomatic aneurysms were larger, had more intraluminal thrombus, and more often affected the profunda femoral artery .Only 12 patients (5%) had acute events, most of them rupture or thrombosis, with a size of 3.5-7 cm in range.
Independent predictors associated with acute aneurysm - related complications were a diameter of 4 cm or greater (P = less than .001), an intraluminal thrombus (P = less than .001), and age younger than 60 (P = .004). Freedom from repair among patients with asymptomatic FAAs was 21% at 5 years, "largely reflecting our practice of indicating the operation for aneurysms greater than 2.5 cm," Dr. Oderich said. The most common indications for repair were pain (34%), intramural thrombus (27%), and size of 2.5 cm or greater (23%).
He reported that 138 patients underwent open repair and 3 patients underwent endovascular treatment of 177 FAAs. The most frequent form of reconstruction was an interposition graft (80%) or bypass (20%). Among the 141 patients who had operative treatment, the 30-day mortality was 1.5%, the morbidity rate was 20%, and the mean length of stay was 7 days. During a mean follow-up of 49 months, there were 35 nonaneurysm-related deaths (27%) and 1 graft-related complication. Patient survival at 5 years was 61%.
"Repair of smaller FAAs may be indicated in patients with intramural thrombus or progressive enlargement," Dr. Oderich concluded. "Current repair of all symptomatic FAAs should remain unchanged. Operative repair was associated with low mortality, morbidity, and durable results."
AT THE SVS ANNUAL MEETING
Major finding: Among patients treated for isolated degenerative femoral artery aneurysms, independent predictors associated with acute aneurysm–related complications were a diameter of 4 cm or greater (P = less than .001), an intraluminal thrombus (P = less than .001), and age younger than 60 (P = .004).
Data source: A retrospective study of 182 patients in the United States who were treated for 236 femoral artery aneurysms that occurred between 2002 and 2012.
Disclosures: Dr. Oderich disclosed that he has served as a consultant to W.L. Gore and Cook Medical.
