User login
Dermatofibrosarcoma Protuberans More Common In Black Patients, Analysis Finds
TOPLINE:
that also found that larger tumor size and older age were associated with survival outcomes.
METHODOLOGY:
- Researchers used the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) registry from 2000 through 2018 to provide a comprehensive report on the incidence of DFSP, a rare, low-grade cutaneous soft tissue sarcoma, and factors associated with metastatic progression, overall survival (OS), and cancer-specific survival.
- A total of 7748 patients (mean age, 43.5 years; 53.3% women; 52% non-Hispanic White) were diagnosed with histologically confirmed DFSP of the skin and connective tissue and were included in the study.
- DFSP incidence was reported as cases per million person-years and age-adjusted to the 2000 US Standard Population, and factors influencing metastasis were assessed.
TAKEAWAY:
- The overall DFSP incidence rate was 6.25 cases per million person-years, with a higher incidence in Black individuals than in White individuals (8.74 vs 4.53).
- The 5-year OS rate was 95.8%. Older age (≥ 60 years; hazard ratio [HR], 6.66), male gender assigned at birth (HR, 1.79), and larger tumor size (≥ 3 cm; HR, 2.02) were associated with poorer OS (P < .001 for all).
- The 1-year and 5-year DFSP-specific survival rates were 99.9% and 99.2%, respectively. Older age (HR, 3.47; P < .001) and larger tumor size (≥ 3 cm; HR, 5.34; P = .002) were associated with significantly worse cancer-specific survival.
- Large tumor size (odds ratio [OR], 2.24) and DFSP located on the head and neck (OR, 4.88), or genitalia (OR, 3.16) were significantly associated with increased metastasis risk. Higher socioeconomic status was linked to a lower risk for metastasis.
IN PRACTICE:
“Our findings highlight the increased incidence rates of DFSP among Black patients. We demonstrate the interplay between patient demographics and clinical factors in influencing DFSP metastasis, OS, and cancer-specific survival,” the authors wrote. The results, they added, “may be useful for further evaluation of proposed causes, which will ultimately lead to further understanding and prevention of this disease.”
SOURCE:
The study was led by Jalal Maghfour, MD, Department of Dermatology, Henry Ford Health, Detroit, and was published online on June 20 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
Details on specific cases in the SEER registry are limited. For 1752 patients, tumor size was not included, increasing the risk for misclassification bias. Because specific pathology reports were not available, the analysis did not address histologic grade.
DISCLOSURES:
The study did not receive any funding support. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
that also found that larger tumor size and older age were associated with survival outcomes.
METHODOLOGY:
- Researchers used the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) registry from 2000 through 2018 to provide a comprehensive report on the incidence of DFSP, a rare, low-grade cutaneous soft tissue sarcoma, and factors associated with metastatic progression, overall survival (OS), and cancer-specific survival.
- A total of 7748 patients (mean age, 43.5 years; 53.3% women; 52% non-Hispanic White) were diagnosed with histologically confirmed DFSP of the skin and connective tissue and were included in the study.
- DFSP incidence was reported as cases per million person-years and age-adjusted to the 2000 US Standard Population, and factors influencing metastasis were assessed.
TAKEAWAY:
- The overall DFSP incidence rate was 6.25 cases per million person-years, with a higher incidence in Black individuals than in White individuals (8.74 vs 4.53).
- The 5-year OS rate was 95.8%. Older age (≥ 60 years; hazard ratio [HR], 6.66), male gender assigned at birth (HR, 1.79), and larger tumor size (≥ 3 cm; HR, 2.02) were associated with poorer OS (P < .001 for all).
- The 1-year and 5-year DFSP-specific survival rates were 99.9% and 99.2%, respectively. Older age (HR, 3.47; P < .001) and larger tumor size (≥ 3 cm; HR, 5.34; P = .002) were associated with significantly worse cancer-specific survival.
- Large tumor size (odds ratio [OR], 2.24) and DFSP located on the head and neck (OR, 4.88), or genitalia (OR, 3.16) were significantly associated with increased metastasis risk. Higher socioeconomic status was linked to a lower risk for metastasis.
IN PRACTICE:
“Our findings highlight the increased incidence rates of DFSP among Black patients. We demonstrate the interplay between patient demographics and clinical factors in influencing DFSP metastasis, OS, and cancer-specific survival,” the authors wrote. The results, they added, “may be useful for further evaluation of proposed causes, which will ultimately lead to further understanding and prevention of this disease.”
SOURCE:
The study was led by Jalal Maghfour, MD, Department of Dermatology, Henry Ford Health, Detroit, and was published online on June 20 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
Details on specific cases in the SEER registry are limited. For 1752 patients, tumor size was not included, increasing the risk for misclassification bias. Because specific pathology reports were not available, the analysis did not address histologic grade.
DISCLOSURES:
The study did not receive any funding support. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
that also found that larger tumor size and older age were associated with survival outcomes.
METHODOLOGY:
- Researchers used the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) registry from 2000 through 2018 to provide a comprehensive report on the incidence of DFSP, a rare, low-grade cutaneous soft tissue sarcoma, and factors associated with metastatic progression, overall survival (OS), and cancer-specific survival.
- A total of 7748 patients (mean age, 43.5 years; 53.3% women; 52% non-Hispanic White) were diagnosed with histologically confirmed DFSP of the skin and connective tissue and were included in the study.
- DFSP incidence was reported as cases per million person-years and age-adjusted to the 2000 US Standard Population, and factors influencing metastasis were assessed.
TAKEAWAY:
- The overall DFSP incidence rate was 6.25 cases per million person-years, with a higher incidence in Black individuals than in White individuals (8.74 vs 4.53).
- The 5-year OS rate was 95.8%. Older age (≥ 60 years; hazard ratio [HR], 6.66), male gender assigned at birth (HR, 1.79), and larger tumor size (≥ 3 cm; HR, 2.02) were associated with poorer OS (P < .001 for all).
- The 1-year and 5-year DFSP-specific survival rates were 99.9% and 99.2%, respectively. Older age (HR, 3.47; P < .001) and larger tumor size (≥ 3 cm; HR, 5.34; P = .002) were associated with significantly worse cancer-specific survival.
- Large tumor size (odds ratio [OR], 2.24) and DFSP located on the head and neck (OR, 4.88), or genitalia (OR, 3.16) were significantly associated with increased metastasis risk. Higher socioeconomic status was linked to a lower risk for metastasis.
IN PRACTICE:
“Our findings highlight the increased incidence rates of DFSP among Black patients. We demonstrate the interplay between patient demographics and clinical factors in influencing DFSP metastasis, OS, and cancer-specific survival,” the authors wrote. The results, they added, “may be useful for further evaluation of proposed causes, which will ultimately lead to further understanding and prevention of this disease.”
SOURCE:
The study was led by Jalal Maghfour, MD, Department of Dermatology, Henry Ford Health, Detroit, and was published online on June 20 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
Details on specific cases in the SEER registry are limited. For 1752 patients, tumor size was not included, increasing the risk for misclassification bias. Because specific pathology reports were not available, the analysis did not address histologic grade.
DISCLOSURES:
The study did not receive any funding support. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
See the Medical World Through Neurodivergent Doctors’ Eyes
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Some 15%-20% of the world’s population are neurodivergent, with conditions such as autism, dyslexia, Tourette syndrome, attention-deficit/hyperactivity disorder (ADHD), and others. With different strengths and challenges around learning, engaging socially, or completing certain tasks, neurodivergent people can face barriers in the workforce.
Meanwhile, studies suggest that neurodivergent people may be overrepresented in STEM fields such as medicine. The medical field may self-select for traits associated with neurodivergent conditions, researchers say, including a hyperfocus on intense interests, pattern recognition, increased curiosity and empathy, and thinking quickly under pressure.
But . They struggle with stigma, a culture of nondisclosure, and lack of accommodations, which can lead to burnout and poor mental health.
“The medical system and the mental health system are some of the spaces that are holding on tightly to some of the outdated understandings of things like autism and ADHD,” says Megan Anna Neff, PsyD, a psychologist with autism and ADHD based in Portland, Oregon.
Situations can get dire: A 2023 survey of more than 200 autistic doctors from several countries found that 77% had considered suicide and 24% had attempted it.
But here’s the crux of it: Many neurodivergent doctors believe their unique ways of thinking and outside-the-box creativity are skills and strengths that can benefit the field. And they say making medicine more inclusive — and better understanding how a neurodivergent physician’s brain works — would allow them to thrive.
Blending In and Breaking Down
The exact number of neurodivergent physicians in the workforce remains unknown. Existing studies are small and focus mainly on autism. But researchers believe the percentage could be higher than we think, because neurodiversity can be underidentified.
Although autism can sometimes be diagnosed as early as 18 months, it’s not uncommon to receive a diagnosis well into adulthood. “Like many late-identified autistic adults, I got my autism diagnosis in the context of autistic burnout,” says Melissa Houser, MD, a primary care physician who received a diagnosis in 2021. Dr. Houser, who uses the pronouns she/they, explains that her experience is common, “a consequence of chronically having your life’s demands exceed your capacity.”
Dr. Houser, who also has ADHD and dyslexia, among other neurodivergent conditions, says that before her diagnosis, she worked in a traditional practice setting. Eventually, she began to notice intense dysregulation and fatigue. “I began to have a lot more difficulties with communication and my motor planning and sequencing,” Dr. Houser says. “I was sleep-deprived, and my needs were not being met. I was in a situation where I had a complete lack of autonomy over my practice.”
Deep in burnout, Dr. Houser says she lost her ability to “mask,” a term used to describe how some neurodivergent people work to “blend in” with societal expectations. This led to further communication breakdowns with her supervisor. Finally, Dr. Houser saw a psychiatrist.
Shortly after her diagnosis, Dr. Houser quit her job and founded All Brains Belong, a nonprofit that provides neurodiversity-affirming medical care, education, and advocacy. Research has found that people with autism are at increased risk for physical health conditions, including immune conditions, gastrointestinal disorders, metabolic conditions, and increased mortality in hospital settings. Understanding these connections can “mean the difference between life and death” for neurodivergent patients, Dr. Houser says.
Yet, in a 2015 study that assessed providers’ ability to recognize autism, a high proportion were not aware that they had patients with autism spectrum disorder, and most reported lacking both the skills and the tools to care for them.
Different as a Doctor and a Patient
Bernadette Grosjean, MD, a retired associate professor of psychiatry at David Geffen School of Medicine at UCLA and a distinguished Fellow of the American Psychiatric Association, also found insight into lifelong experiences as both a doctor and a patient with her autism diagnosis, which came when she was 61.
“Looking back, I was a smart kid but kind of clumsy and different in other ways,” Dr. Grosjean says. According to a 2021 survey by Cambridge University, autistic individuals are significantly more likely to identify as LGBTQ+, and Dr. Grosjean, who is gay, says that not being fully accepted by family or friends played a role in her struggles with mental health issues.
Throughout her mental health treatment, Dr. Grosjean felt as though her providers “were expecting from me things that I didn’t know how to do or fix. I didn’t know how to be a ‘good’ patient,” she recalls.
As a psychiatrist, Dr. Grosjean started to notice that many of the women she treated for borderline personality disorder, which is categorized by unstable relationships and emotions, were autistic. “I then started asking lots of questions about myself — the fact that I’ve always been very sensitive or that I’ve been accused of being both hypersensitive and not having emotions, and I understood a lot.”
When Dr. Grosjean came across Autistic Doctors International, a group of over 800 autistic doctors worldwide, she says, “I found my tribe.” She now serves as the US lead for psychiatry for the group, which is focused on support, advocacy, research, and education around neurodiversity.
Psychiatric comorbidities can accompany neurodivergent conditions. But a growing body of research, including a 2022 study published in the European Archives of Psychiatry and Clinical Neuroscience, indicates that autism and ADHD are frequently misdiagnosed as depression or anxiety.
Dr. Neff was unaware of her conditions until one of her children was diagnosed with autism in 2021. She started to research it. “As I was learning about autism and girls, I was like, ‘Oh, my gosh, this is me,’ ” Dr. Neff recalls. Within a few weeks, she had her own diagnosis.
In hindsight, Dr. Neff has more clarity regarding her struggles in the traditional medical space. She had found it difficult to fit patients into short appointment windows and keep their notes concise. Although she loved hospital work, the environment had been overwhelming and led to burnout.
‘A Deficit-Based Lens’
Dr. Houser believes that too often, autism is viewed through a “deficit-based lens.” Stressors like sensory overload, changes in routine, or unexpected events can exacerbate behavioral challenges for neurodivergent people in the workplace. The DSM-5 criteria for autism, she points out, are largely based on autistic “stress behaviors.”
The result, Dr. Houser says, is that neurodivergent doctors are judged by their response to stressors that put them at a disadvantage rather than their capabilities under more positive circumstances. “The more dysregulated someone is,” she says, “the more likely they are to manifest those observable behaviors.”
Dr. Neff notes that medicine is a very “sensory overwhelming work environment.” Working in ob.gyn. and primary care clinics, she remembers often coming home with a headache and a low-grade fever. “I had no idea why, but I now realize it’s because I was so sensory sick.”
Fearing for her job, Dr. Neff intentionally waited until she was in private practice to disclose her neurodiversity. “I don’t think it would have been received well if I was in a hospital system,” she says. “There’s a lot of invalidation that can come when someone chooses to self-disclose, and their colleagues don’t have a framework in mind to understand.” In one instance, after revealing her diagnosis, she remembers a well-known researcher telling her she wasn’t autistic.
Dr. Grosjean has also had former colleagues invalidate her diagnosis, something she says “keeps people quiet.”
Understanding the Neurodivergent Brain
The general lack of education on how neurodivergent brains work, physicians with these conditions say, means they are not often recognized for how they can function with certain accommodations and how they could contribute in unique ways if their workplace challenges were reduced.
“What we know about autistic brains is that we are systems-thinking pattern matchers,” says Dr. Houser, who formed an interdisciplinary task force to explore medical conditions that are more common in autistic people. Through that comprehensive approach, she has worked to find best practices to treat the constellation of conditions that can arise among these patients. “My autistic brain allowed me to do that,” Dr. Houser says.
Catriona McVey, a medical student in the United Kingdom and creator of the blog Attention Deficit Doctor, points out that “ADHD brains are interest-driven; they can be very focused when you’re doing something enjoyable or new due to increased dopaminergic stimulation.” Ms. McVey speaks from personal experience. “I’ve hyperfocused before on an essay that interested me for over 10 hours,” she recalls, “so I imagine if I was interested in surgery, I could easily hyperfocus on a long operation.”
Empathy is another key part of medical practice. Contrary to stereotypes of neurodivergent people lacking empathy, current research suggests this isn’t true. A concept known as the “double empathy problem,” a term coined by British researcher Damian Milton in 2012, challenges the misconception that autistic people do not have empathy, explains Dr. Grosjean.
Mr. Milton theorized that there are two types of empathy: emotional, when you feel someone else’s pain, and cognitive, which involves critical thinking to understand someone’s emotions or thoughts. “Autistic people have, in general, a lot of emotional empathy,” Dr. Grosjean says, “but the cognitive empathy they don’t have as well.”
Dr. Neff has experienced this in her practice. “I will often feel what my clients are feeling as they’re feeling it,” she says, adding that she has always had an innate ability to analyze and connect with clients. She’s good at observing the interplay of health conditions, incorporating biology, psychology, and social conceptualizations of issues, with nuance. She feels that recognizing behavioral patterns or psychological triggers in her patients helps her see them holistically and provide better care. “That was a skill even before I realized I was autistic, but I always thought it was just intuitive to everyone,” she says.
Support Can Lead to Success
The Americans with Disabilities Act requires employers to provide reasonable accommodations to neurodivergent employees. However, getting those accommodations involves disclosure, which many physicians have reasons to avoid.
It also means more work. Requesting and putting adjustments in place can take a lot of time and energy to organize. Ms. McVey says they can be “long-winded, multistep tasks” that are not very compatible with ADHD. “Some doctors report that service pressures and funding are used as excuses to refuse adjustments,” she adds.
Ms. McVey lists several workplace accommodations that could be helpful, including flexible working hours, a quiet space to complete paperwork, dictation software, and extra time for medical students to complete written exams.
Neurodivergent physicians have also called for increased diversity of senior leadership and utilizing “cognitive apprenticeship models,” where employees explain their thought processes and receive timely feedback.
But far too often, there is little intervention until a doctor reaches a crisis point. “I look forward to the day when we don’t have to wait until people are profoundly depleted to discover how their brains work,” says Dr. Houser.
Beyond logistical and structural changes in the medical field, Dr. Grosjean speaks of the simple need to listen to colleagues with an open mind and believe them when they express their feelings and experiences. “Everyone has a role to play in challenging stigma, misconceptions, and stereotypes,” Ms. McVey agrees. Ask yourself the old question, she suggests: “If not me, then who? If not now, then when?”
A version of this article first appeared on Medscape.com.
Plantar Hyperpigmentation
The Comparison
Plantar hyperpigmentation (also known as plantar melanosis [increased melanin], volar pigmented macules, benign racial melanosis, acral pigmentation, acral ethnic melanosis, or mottled hyperpigmentation of the plantar surface) is a benign finding in many individuals and is especially prevalent in those with darker skin tones. Acral refers to manifestation on the hands and feet, volar on the palms and soles, and plantar on the soles only. Here, we focus on plantar hyperpigmentation. We use the terms ethnic and racial interchangeably.
It is critically important to differentiate benign hyperpigmentation, which is common in patients with skin of color, from melanoma. Although rare, Black patients in the United States experience high morbidity and mortality from acral melanoma, which often is diagnosed late in the disease course.1
There are many causes of hyperpigmentation on the plantar surfaces, including benign ethnic melanosis, nevi, melanoma, infections such as syphilis and tinea nigra, conditions such as Peutz-Jeghers syndrome and Laugier-Hunziker syndrome, and postinflammatory hyperpigmentation secondary to atopic dermatitis and psoriasis. We focus on the most common causes, ethnic melanosis and nevi, as well as melanoma, which is the deadliest cause.
Epidemiology
In a 1980 study (N=251), Black Americans had a high incidence of plantar hyperpigmentation, with 52% of affected patients having dark brown skin and 31% having light brown skin.2
The epidemiology of melanoma varies by race/ethnicity. Melanoma in Black individuals is relatively rare, with an annual incidence of approximately 1 in 100,000 individuals.3 However, when individuals with skin of color develop melanoma, they are more likely than their White counterparts to have acral melanoma (acral lentiginous melanoma), one of the deadliest types.1 In a case series of Black patients with melanoma (N=48) from 2 tertiary care centers in Texas, 30 of 40 primary cutaneous melanomas (75%) were located on acral skin.4 Overall, 13 patients developed stage IV disease and 12 died due to disease progression. All patients who developed distant metastases or died of melanoma had acral melanoma.4 Individuals of Asian descent also have a high incidence of acral melanoma, as shown in research from Japan.5-9
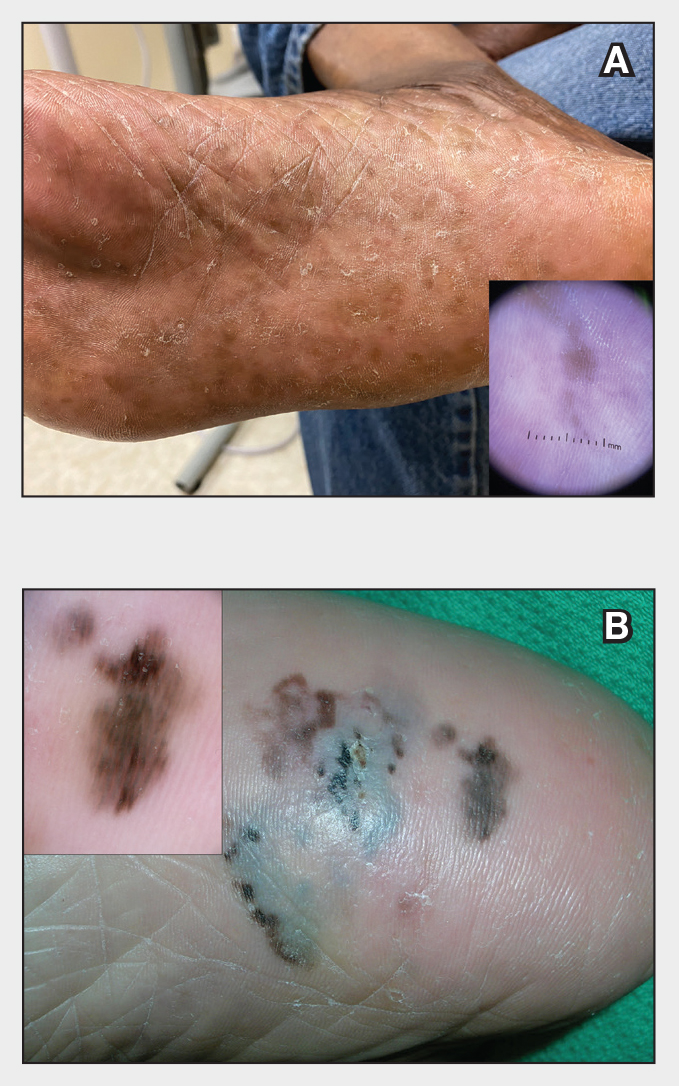
Key clinical features in individuals with darker skin tones
Dermoscopy is an evidence-based clinical examination method for earlier diagnosis of cutaneous melanoma, including on acral skin.10,11 Benign nevi on the volar skin as well as the palms and soles tend to have one of these 3 dermoscopic patterns: parallel furrow, lattice, or irregular fibrillar. The pattern that is most predictive of volar melanoma is the parallel ridge pattern (PRP) (Figures A and B [insets]), which showed a high specificity (99.0%) and very high negative predictive value (97.7%) for malignant melanoma in a Japanese population.7 The PRP data from this study cannot be applied reliably to Black individuals, especially because benign ethnic melanosis and other benign conditions can demonstrate PRP.12 Reliance on the PRP as a diagnostic clue could result in unneccessary biopsies in as many as 50% of Black patients with benign plantar hyperpigmentation.2 Furthermore, biopsies of the plantar surface can be painful and cause pain while walking.
It has been suggested that PRP seen on dermoscopy in benign hyperpigmentation such as ethnic melanosis and nevi may preserve the acrosyringia (eccrine gland openings on the ridge), whereas PRP in melanoma may obliterate the acrosyringia.13 This observation is based on case reports only and needs further study. However, if validated, it could be a useful diagnostic clue.
Worth noting
In a retrospective cohort study of skin cancer in Black individuals (n=165) at a New York City–based cancer center from 2000 to 2020, 68% of patients were diagnosed with melanomas—80% were the acral subtype and 75% displayed a PRP. However, the surrounding uninvolved background skin, which was visible in most cases, also demonstrated a PRP.14 Because of the high morbidity and mortality rates of acral melanoma, clinicians should biopsy or immediately refer patients with concerning plantar hyperpigmentation to a dermatologist.
Health disparity highlight
The mortality rate for acral melanoma in Black patients is disproportionately high for the following reasons15,16:
- Patients and health care providers do not expect to see melanoma in Black patients (it truly is rare!), so screening and education on sun protection are limited.
- Benign ethnic melanosis makes it more difficult to distinguish between early acral melanoma and benign skin changes.
- Black patients and other US patient populations with skin of color may be less likely to have health insurance, which contributes to inequities in access to health care. As of 2022, the uninsured rates for nonelderly American Indian and Alaska Native, Hispanic, Native Hawaiian and Other Pacific Islander, Black, and White individuals were 19.1%, 18.0%, 12.7%, 10.0%, and 6.6%, respectively.17
Multi-institutional registries could improve understanding of acral melanoma in Black patients.4 More studies are needed to help differentiate between the dermoscopic finding of PRP in benign ethnic melanosis vs malignant melanoma.
- Huang K, Fan J, Misra S. Acral lentiginous melanoma: incidence and survival in the United States, 2006-2015: an analysis of the SEER registry. J Surg Res. 2020;251:329-339. doi:10.1016/j.jss.2020.02.010
- Coleman WP, Gately LE, Krementz AB, et al. Nevi, lentigines, and melanomas in blacks. Arch Dermatol. 1980;116:548-551.
- Centers for Disease Control and Prevention. Melanoma Incidence and Mortality, United States: 2012-2016. USCS Data Brief, no. 9. Centers for Disease Control and Prevention, US Department of Health and Human Services; 2019. https://www.cdc.gov/cancer/uscs/about/data-briefs/no9-melanoma-incidence-mortality-UnitedStates-2012-2016.htm
- Wix SN, Brown AB, Heberton M, et al. Clinical features and outcomes of black patients with melanoma. JAMA Dermatol. 2024;160:328-333. doi:10.1001/jamadermatol.2023.5789
- Saida T, Koga H. Dermoscopic patterns of acral melanocytic nevi: their variations, changes, and significance. Arch Dermatol. 2007;143:1423-1426. doi:10.1001/archderm.143.11.1423
- Saida T, Koga H, Uhara H. Key points in dermoscopic differentiation between early acral melanoma and acral nevus. J Dermatol. 2011;38:25-34. doi:10.1111/j.1346-8138.2010.01174.x
- Saida T, Miyazaki A, Oguchi S. Significance of dermoscopic patterns in detecting malignant melanoma on acral volar skin: results of a multicenter study in Japan. Arch Dermatol. 2004;140:1233-1238. doi:10.1001/archderm.140.10.1233
- Saida T, Koga H, Uhara H. Dermoscopy for acral melanocytic lesions: revision of the 3-step algorithm and refined definition of the regular and irregular fibrillar pattern. Dermatol Pract Concept. 2022;12:e2022123. doi:10.5826/dpc.1203a123
- Heath CR, Usatine RP. Melanoma. Cutis. 2022;109:284-285.doi:10.12788/cutis.0513.
- Dinnes J, Deeks JJ, Chuchu N, et al; Cochrane Skin Cancer Diagnostic Test Accuracy Group. Visual inspection and dermoscopy, alone or in combination, for diagnosing keratinocyte skin cancers in adults. Cochrane Database Syst Rev. 2018; 12:CD011901. doi:10.1002/14651858.CD011901.pub2
- Vestergaard ME, Macaskill P, Holt PE, et al. Dermoscopy compared with naked-eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting. Br J Dermatol. 2008;159:669-676. doi:10.1111/j.1365-2133.2008.08713.x
- Phan A, Dalle S, Marcilly MC, et al. Benign dermoscopic parallel ridge pattern variants. Arch Dermatol. 2011;147:634. doi:10.1001/archdermatol.2011.47
- Fracaroli TS, Lavorato FG, Maceira JP, et al. Parallel ridge pattern on dermoscopy: observation in non-melanoma cases. An Bras Dermatol. 2013;88:646-648. doi:10.1590/abd1806-4841.20132058
- Manci RN, Dauscher M, Marchetti MA, et al. Features of skin cancer in black individuals: a single-institution retrospective cohort study. Dermatol Pract Concept. 2022;12:e2022075. doi:10.5826/dpc.1202a75
- Dawes SM, Tsai S, Gittleman H, et al. Racial disparities in melanoma survival. J Am Acad Dermatol. 2016;75:983-991. doi:10.1016/j.jaad.2016.06.006
- Ingrassia JP, Stein JA, Levine A, et al. Diagnosis and management of acral pigmented lesions. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2023;49:926-931. doi:10.1097/DSS.0000000000003891
- Hill L, Artiga S, Damico A. Health coverage by race and ethnicity, 2010-2022. Kaiser Family Foundation. Published January 11, 2024. Accessed May 9, 2024. https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-coverage-by-race-and-ethnicity
The Comparison
Plantar hyperpigmentation (also known as plantar melanosis [increased melanin], volar pigmented macules, benign racial melanosis, acral pigmentation, acral ethnic melanosis, or mottled hyperpigmentation of the plantar surface) is a benign finding in many individuals and is especially prevalent in those with darker skin tones. Acral refers to manifestation on the hands and feet, volar on the palms and soles, and plantar on the soles only. Here, we focus on plantar hyperpigmentation. We use the terms ethnic and racial interchangeably.
It is critically important to differentiate benign hyperpigmentation, which is common in patients with skin of color, from melanoma. Although rare, Black patients in the United States experience high morbidity and mortality from acral melanoma, which often is diagnosed late in the disease course.1
There are many causes of hyperpigmentation on the plantar surfaces, including benign ethnic melanosis, nevi, melanoma, infections such as syphilis and tinea nigra, conditions such as Peutz-Jeghers syndrome and Laugier-Hunziker syndrome, and postinflammatory hyperpigmentation secondary to atopic dermatitis and psoriasis. We focus on the most common causes, ethnic melanosis and nevi, as well as melanoma, which is the deadliest cause.
Epidemiology
In a 1980 study (N=251), Black Americans had a high incidence of plantar hyperpigmentation, with 52% of affected patients having dark brown skin and 31% having light brown skin.2
The epidemiology of melanoma varies by race/ethnicity. Melanoma in Black individuals is relatively rare, with an annual incidence of approximately 1 in 100,000 individuals.3 However, when individuals with skin of color develop melanoma, they are more likely than their White counterparts to have acral melanoma (acral lentiginous melanoma), one of the deadliest types.1 In a case series of Black patients with melanoma (N=48) from 2 tertiary care centers in Texas, 30 of 40 primary cutaneous melanomas (75%) were located on acral skin.4 Overall, 13 patients developed stage IV disease and 12 died due to disease progression. All patients who developed distant metastases or died of melanoma had acral melanoma.4 Individuals of Asian descent also have a high incidence of acral melanoma, as shown in research from Japan.5-9
Key clinical features in individuals with darker skin tones
Dermoscopy is an evidence-based clinical examination method for earlier diagnosis of cutaneous melanoma, including on acral skin.10,11 Benign nevi on the volar skin as well as the palms and soles tend to have one of these 3 dermoscopic patterns: parallel furrow, lattice, or irregular fibrillar. The pattern that is most predictive of volar melanoma is the parallel ridge pattern (PRP) (Figures A and B [insets]), which showed a high specificity (99.0%) and very high negative predictive value (97.7%) for malignant melanoma in a Japanese population.7 The PRP data from this study cannot be applied reliably to Black individuals, especially because benign ethnic melanosis and other benign conditions can demonstrate PRP.12 Reliance on the PRP as a diagnostic clue could result in unneccessary biopsies in as many as 50% of Black patients with benign plantar hyperpigmentation.2 Furthermore, biopsies of the plantar surface can be painful and cause pain while walking.
It has been suggested that PRP seen on dermoscopy in benign hyperpigmentation such as ethnic melanosis and nevi may preserve the acrosyringia (eccrine gland openings on the ridge), whereas PRP in melanoma may obliterate the acrosyringia.13 This observation is based on case reports only and needs further study. However, if validated, it could be a useful diagnostic clue.
Worth noting
In a retrospective cohort study of skin cancer in Black individuals (n=165) at a New York City–based cancer center from 2000 to 2020, 68% of patients were diagnosed with melanomas—80% were the acral subtype and 75% displayed a PRP. However, the surrounding uninvolved background skin, which was visible in most cases, also demonstrated a PRP.14 Because of the high morbidity and mortality rates of acral melanoma, clinicians should biopsy or immediately refer patients with concerning plantar hyperpigmentation to a dermatologist.
Health disparity highlight
The mortality rate for acral melanoma in Black patients is disproportionately high for the following reasons15,16:
- Patients and health care providers do not expect to see melanoma in Black patients (it truly is rare!), so screening and education on sun protection are limited.
- Benign ethnic melanosis makes it more difficult to distinguish between early acral melanoma and benign skin changes.
- Black patients and other US patient populations with skin of color may be less likely to have health insurance, which contributes to inequities in access to health care. As of 2022, the uninsured rates for nonelderly American Indian and Alaska Native, Hispanic, Native Hawaiian and Other Pacific Islander, Black, and White individuals were 19.1%, 18.0%, 12.7%, 10.0%, and 6.6%, respectively.17
Multi-institutional registries could improve understanding of acral melanoma in Black patients.4 More studies are needed to help differentiate between the dermoscopic finding of PRP in benign ethnic melanosis vs malignant melanoma.
The Comparison
Plantar hyperpigmentation (also known as plantar melanosis [increased melanin], volar pigmented macules, benign racial melanosis, acral pigmentation, acral ethnic melanosis, or mottled hyperpigmentation of the plantar surface) is a benign finding in many individuals and is especially prevalent in those with darker skin tones. Acral refers to manifestation on the hands and feet, volar on the palms and soles, and plantar on the soles only. Here, we focus on plantar hyperpigmentation. We use the terms ethnic and racial interchangeably.
It is critically important to differentiate benign hyperpigmentation, which is common in patients with skin of color, from melanoma. Although rare, Black patients in the United States experience high morbidity and mortality from acral melanoma, which often is diagnosed late in the disease course.1
There are many causes of hyperpigmentation on the plantar surfaces, including benign ethnic melanosis, nevi, melanoma, infections such as syphilis and tinea nigra, conditions such as Peutz-Jeghers syndrome and Laugier-Hunziker syndrome, and postinflammatory hyperpigmentation secondary to atopic dermatitis and psoriasis. We focus on the most common causes, ethnic melanosis and nevi, as well as melanoma, which is the deadliest cause.
Epidemiology
In a 1980 study (N=251), Black Americans had a high incidence of plantar hyperpigmentation, with 52% of affected patients having dark brown skin and 31% having light brown skin.2
The epidemiology of melanoma varies by race/ethnicity. Melanoma in Black individuals is relatively rare, with an annual incidence of approximately 1 in 100,000 individuals.3 However, when individuals with skin of color develop melanoma, they are more likely than their White counterparts to have acral melanoma (acral lentiginous melanoma), one of the deadliest types.1 In a case series of Black patients with melanoma (N=48) from 2 tertiary care centers in Texas, 30 of 40 primary cutaneous melanomas (75%) were located on acral skin.4 Overall, 13 patients developed stage IV disease and 12 died due to disease progression. All patients who developed distant metastases or died of melanoma had acral melanoma.4 Individuals of Asian descent also have a high incidence of acral melanoma, as shown in research from Japan.5-9
Key clinical features in individuals with darker skin tones
Dermoscopy is an evidence-based clinical examination method for earlier diagnosis of cutaneous melanoma, including on acral skin.10,11 Benign nevi on the volar skin as well as the palms and soles tend to have one of these 3 dermoscopic patterns: parallel furrow, lattice, or irregular fibrillar. The pattern that is most predictive of volar melanoma is the parallel ridge pattern (PRP) (Figures A and B [insets]), which showed a high specificity (99.0%) and very high negative predictive value (97.7%) for malignant melanoma in a Japanese population.7 The PRP data from this study cannot be applied reliably to Black individuals, especially because benign ethnic melanosis and other benign conditions can demonstrate PRP.12 Reliance on the PRP as a diagnostic clue could result in unneccessary biopsies in as many as 50% of Black patients with benign plantar hyperpigmentation.2 Furthermore, biopsies of the plantar surface can be painful and cause pain while walking.
It has been suggested that PRP seen on dermoscopy in benign hyperpigmentation such as ethnic melanosis and nevi may preserve the acrosyringia (eccrine gland openings on the ridge), whereas PRP in melanoma may obliterate the acrosyringia.13 This observation is based on case reports only and needs further study. However, if validated, it could be a useful diagnostic clue.
Worth noting
In a retrospective cohort study of skin cancer in Black individuals (n=165) at a New York City–based cancer center from 2000 to 2020, 68% of patients were diagnosed with melanomas—80% were the acral subtype and 75% displayed a PRP. However, the surrounding uninvolved background skin, which was visible in most cases, also demonstrated a PRP.14 Because of the high morbidity and mortality rates of acral melanoma, clinicians should biopsy or immediately refer patients with concerning plantar hyperpigmentation to a dermatologist.
Health disparity highlight
The mortality rate for acral melanoma in Black patients is disproportionately high for the following reasons15,16:
- Patients and health care providers do not expect to see melanoma in Black patients (it truly is rare!), so screening and education on sun protection are limited.
- Benign ethnic melanosis makes it more difficult to distinguish between early acral melanoma and benign skin changes.
- Black patients and other US patient populations with skin of color may be less likely to have health insurance, which contributes to inequities in access to health care. As of 2022, the uninsured rates for nonelderly American Indian and Alaska Native, Hispanic, Native Hawaiian and Other Pacific Islander, Black, and White individuals were 19.1%, 18.0%, 12.7%, 10.0%, and 6.6%, respectively.17
Multi-institutional registries could improve understanding of acral melanoma in Black patients.4 More studies are needed to help differentiate between the dermoscopic finding of PRP in benign ethnic melanosis vs malignant melanoma.
- Huang K, Fan J, Misra S. Acral lentiginous melanoma: incidence and survival in the United States, 2006-2015: an analysis of the SEER registry. J Surg Res. 2020;251:329-339. doi:10.1016/j.jss.2020.02.010
- Coleman WP, Gately LE, Krementz AB, et al. Nevi, lentigines, and melanomas in blacks. Arch Dermatol. 1980;116:548-551.
- Centers for Disease Control and Prevention. Melanoma Incidence and Mortality, United States: 2012-2016. USCS Data Brief, no. 9. Centers for Disease Control and Prevention, US Department of Health and Human Services; 2019. https://www.cdc.gov/cancer/uscs/about/data-briefs/no9-melanoma-incidence-mortality-UnitedStates-2012-2016.htm
- Wix SN, Brown AB, Heberton M, et al. Clinical features and outcomes of black patients with melanoma. JAMA Dermatol. 2024;160:328-333. doi:10.1001/jamadermatol.2023.5789
- Saida T, Koga H. Dermoscopic patterns of acral melanocytic nevi: their variations, changes, and significance. Arch Dermatol. 2007;143:1423-1426. doi:10.1001/archderm.143.11.1423
- Saida T, Koga H, Uhara H. Key points in dermoscopic differentiation between early acral melanoma and acral nevus. J Dermatol. 2011;38:25-34. doi:10.1111/j.1346-8138.2010.01174.x
- Saida T, Miyazaki A, Oguchi S. Significance of dermoscopic patterns in detecting malignant melanoma on acral volar skin: results of a multicenter study in Japan. Arch Dermatol. 2004;140:1233-1238. doi:10.1001/archderm.140.10.1233
- Saida T, Koga H, Uhara H. Dermoscopy for acral melanocytic lesions: revision of the 3-step algorithm and refined definition of the regular and irregular fibrillar pattern. Dermatol Pract Concept. 2022;12:e2022123. doi:10.5826/dpc.1203a123
- Heath CR, Usatine RP. Melanoma. Cutis. 2022;109:284-285.doi:10.12788/cutis.0513.
- Dinnes J, Deeks JJ, Chuchu N, et al; Cochrane Skin Cancer Diagnostic Test Accuracy Group. Visual inspection and dermoscopy, alone or in combination, for diagnosing keratinocyte skin cancers in adults. Cochrane Database Syst Rev. 2018; 12:CD011901. doi:10.1002/14651858.CD011901.pub2
- Vestergaard ME, Macaskill P, Holt PE, et al. Dermoscopy compared with naked-eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting. Br J Dermatol. 2008;159:669-676. doi:10.1111/j.1365-2133.2008.08713.x
- Phan A, Dalle S, Marcilly MC, et al. Benign dermoscopic parallel ridge pattern variants. Arch Dermatol. 2011;147:634. doi:10.1001/archdermatol.2011.47
- Fracaroli TS, Lavorato FG, Maceira JP, et al. Parallel ridge pattern on dermoscopy: observation in non-melanoma cases. An Bras Dermatol. 2013;88:646-648. doi:10.1590/abd1806-4841.20132058
- Manci RN, Dauscher M, Marchetti MA, et al. Features of skin cancer in black individuals: a single-institution retrospective cohort study. Dermatol Pract Concept. 2022;12:e2022075. doi:10.5826/dpc.1202a75
- Dawes SM, Tsai S, Gittleman H, et al. Racial disparities in melanoma survival. J Am Acad Dermatol. 2016;75:983-991. doi:10.1016/j.jaad.2016.06.006
- Ingrassia JP, Stein JA, Levine A, et al. Diagnosis and management of acral pigmented lesions. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2023;49:926-931. doi:10.1097/DSS.0000000000003891
- Hill L, Artiga S, Damico A. Health coverage by race and ethnicity, 2010-2022. Kaiser Family Foundation. Published January 11, 2024. Accessed May 9, 2024. https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-coverage-by-race-and-ethnicity
- Huang K, Fan J, Misra S. Acral lentiginous melanoma: incidence and survival in the United States, 2006-2015: an analysis of the SEER registry. J Surg Res. 2020;251:329-339. doi:10.1016/j.jss.2020.02.010
- Coleman WP, Gately LE, Krementz AB, et al. Nevi, lentigines, and melanomas in blacks. Arch Dermatol. 1980;116:548-551.
- Centers for Disease Control and Prevention. Melanoma Incidence and Mortality, United States: 2012-2016. USCS Data Brief, no. 9. Centers for Disease Control and Prevention, US Department of Health and Human Services; 2019. https://www.cdc.gov/cancer/uscs/about/data-briefs/no9-melanoma-incidence-mortality-UnitedStates-2012-2016.htm
- Wix SN, Brown AB, Heberton M, et al. Clinical features and outcomes of black patients with melanoma. JAMA Dermatol. 2024;160:328-333. doi:10.1001/jamadermatol.2023.5789
- Saida T, Koga H. Dermoscopic patterns of acral melanocytic nevi: their variations, changes, and significance. Arch Dermatol. 2007;143:1423-1426. doi:10.1001/archderm.143.11.1423
- Saida T, Koga H, Uhara H. Key points in dermoscopic differentiation between early acral melanoma and acral nevus. J Dermatol. 2011;38:25-34. doi:10.1111/j.1346-8138.2010.01174.x
- Saida T, Miyazaki A, Oguchi S. Significance of dermoscopic patterns in detecting malignant melanoma on acral volar skin: results of a multicenter study in Japan. Arch Dermatol. 2004;140:1233-1238. doi:10.1001/archderm.140.10.1233
- Saida T, Koga H, Uhara H. Dermoscopy for acral melanocytic lesions: revision of the 3-step algorithm and refined definition of the regular and irregular fibrillar pattern. Dermatol Pract Concept. 2022;12:e2022123. doi:10.5826/dpc.1203a123
- Heath CR, Usatine RP. Melanoma. Cutis. 2022;109:284-285.doi:10.12788/cutis.0513.
- Dinnes J, Deeks JJ, Chuchu N, et al; Cochrane Skin Cancer Diagnostic Test Accuracy Group. Visual inspection and dermoscopy, alone or in combination, for diagnosing keratinocyte skin cancers in adults. Cochrane Database Syst Rev. 2018; 12:CD011901. doi:10.1002/14651858.CD011901.pub2
- Vestergaard ME, Macaskill P, Holt PE, et al. Dermoscopy compared with naked-eye examination for the diagnosis of primary melanoma: a meta-analysis of studies performed in a clinical setting. Br J Dermatol. 2008;159:669-676. doi:10.1111/j.1365-2133.2008.08713.x
- Phan A, Dalle S, Marcilly MC, et al. Benign dermoscopic parallel ridge pattern variants. Arch Dermatol. 2011;147:634. doi:10.1001/archdermatol.2011.47
- Fracaroli TS, Lavorato FG, Maceira JP, et al. Parallel ridge pattern on dermoscopy: observation in non-melanoma cases. An Bras Dermatol. 2013;88:646-648. doi:10.1590/abd1806-4841.20132058
- Manci RN, Dauscher M, Marchetti MA, et al. Features of skin cancer in black individuals: a single-institution retrospective cohort study. Dermatol Pract Concept. 2022;12:e2022075. doi:10.5826/dpc.1202a75
- Dawes SM, Tsai S, Gittleman H, et al. Racial disparities in melanoma survival. J Am Acad Dermatol. 2016;75:983-991. doi:10.1016/j.jaad.2016.06.006
- Ingrassia JP, Stein JA, Levine A, et al. Diagnosis and management of acral pigmented lesions. Dermatol Surg Off Publ Am Soc Dermatol Surg Al. 2023;49:926-931. doi:10.1097/DSS.0000000000003891
- Hill L, Artiga S, Damico A. Health coverage by race and ethnicity, 2010-2022. Kaiser Family Foundation. Published January 11, 2024. Accessed May 9, 2024. https://www.kff.org/racial-equity-and-health-policy/issue-brief/health-coverage-by-race-and-ethnicity

Central Centrifugal Cicatricial Alopecia in Males: Analysis of Time to Diagnosis and Disease Severity
To the Editor:
Central centrifugal cicatricial alopecia (CCCA) is a chronic progressive type of scarring alopecia that primarily affects women of African descent.1 The disorder rarely is reported in men, which may be due to misdiagnosis or delayed diagnosis. Early diagnosis and treatment are the cornerstones to slow or halt disease progression and prevent permanent damage to hair follicles. This study aimed to investigate the time to diagnosis and disease severity among males with CCCA.
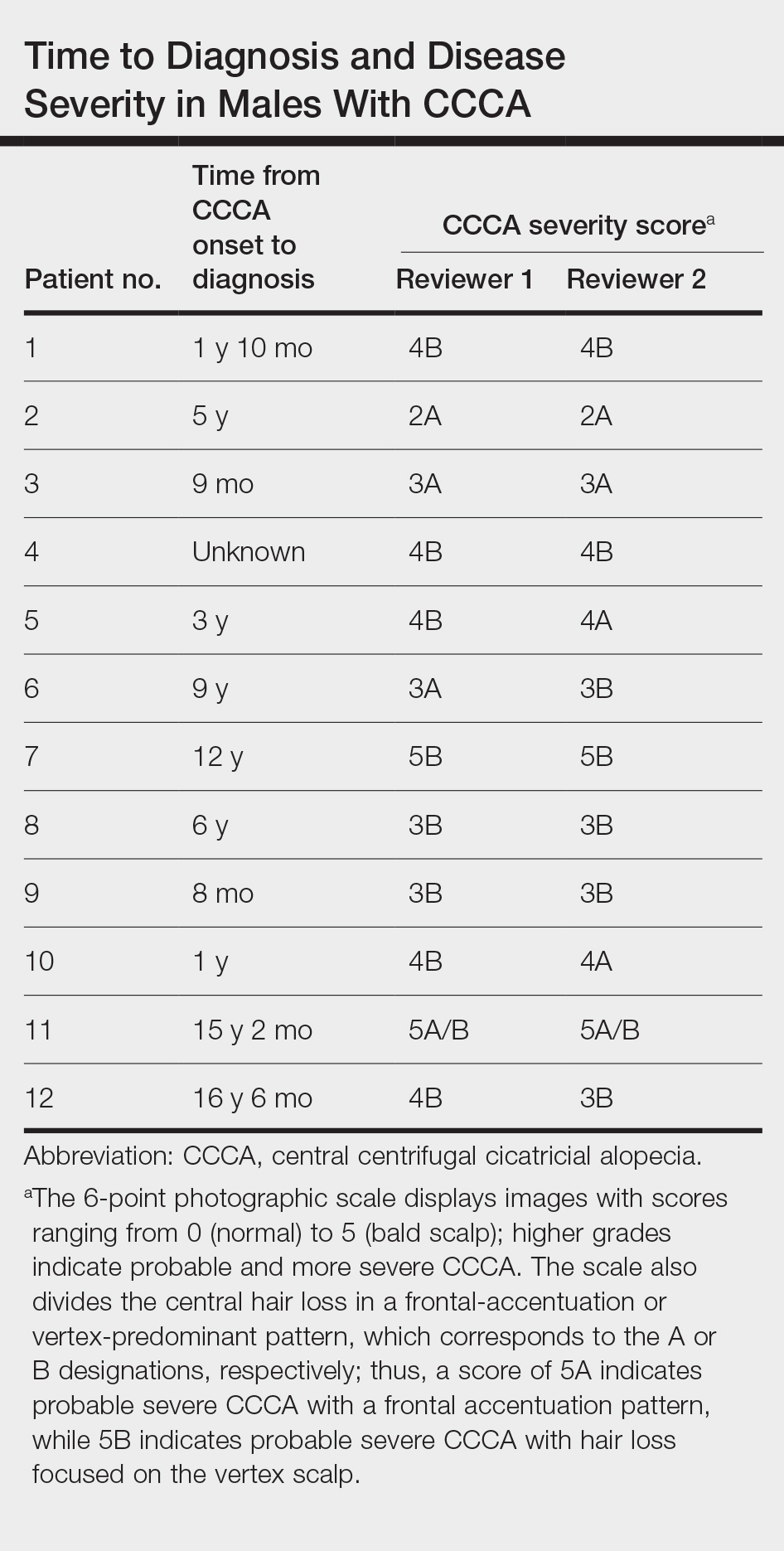
We conducted a retrospective chart review of male patients older than 18 years seen in outpatient clinics at an academic dermatology department (Philadelphia, Pennsylvania) between January 2012 and December 2022. An electronic query using the International Classification of Diseases, Ninth and Tenth Revisions, code L66.9 (cicatricial alopecia, unspecified) was performed. Patients were included if they had a clinical diagnosis of CCCA, histologic evidence of CCCA, and scalp photographs from the initial dermatology visit. Patients with folliculitis decalvans, scalp biopsy features that limited characterization, or no scalp biopsy were excluded from the study. Onset of CCCA was defined as the patient-reported start time of hair loss and/or scalp symptoms. To determine alopecia severity, the degree of central scalp hair loss was independently assessed by 2 dermatologists (S.C.T., T.O.) using the central scalp alopecia photographic scale in African American women.2,3 This 6-point photographic scale displays images with grades ranging from 0 (normal) to 5 (bald scalp); higher grades indicate probable and more severe CCCA. The scale also divides the central hair loss in a frontal-accentuation or vertex-predominant pattern, which corresponds to the A or B designations, respectively; thus, a score of 5A indicates probable severe CCCA with a frontal accentuation pattern, while 5B indicates probable severe CCCA with hair loss focused on the vertex scalp. This study was approved by the University of Pennsylvania institutional review board (approval #850730).
Of 108 male patients, 12 met the eligibility criteria. Nearly all patients (91.7% [11/12]) had a CCCA severity grade of 3 or higher at the initial dermatology visit, indicating extensive hair loss (Table). The clinical appearance of severity grades 2 through 5 is demonstrated in the Figure. Among patients with a known disease duration prior to diagnosis, 72.7% (8/11) were diagnosed more than 1 year after onset of CCCA, and 45.4% (5/11) were diagnosed more than 5 years after onset. On average (SD), it took 6.4 (5.9) years for patients to receive a diagnosis of CCCA after the onset of scalp symptoms and/or hair loss.
Randomized controlled trials evaluating treatment of CCCA are lacking, and anecdotal evidence posits a better treatment response in early CCCA; however, our results suggest that most male patients present with advanced CCCA and receive a diagnosis years after disease onset. Similar research in alopecia areata has shown that 72.4% (105/145) of patients received their diagnosis within a year after onset of symptoms, and the mean time from onset of symptoms to diagnosis was 1 year.4 In contrast, male patients with CCCA experience considerable diagnostic delays. This disparity indicates the need for clinicians to increase recognition of CCCA in men and quickly refer them to a dermatologist for prompt treatment.

Androgenetic alopecia (AGA) commonly is at the top of the differential diagnosis for hair loss on the vertex of the scalp in males, but clinicians should maintain a high index of suspicion for CCCA, especially when scalp symptoms or atypical features of AGA are present.5 Androgenetic alopecia typically is asymptomatic, whereas the symptoms of CCCA may include itching, tenderness, and/or burning.6,7 Trichoscopy is useful to evaluate for scarring, and a scalp biopsy may reveal other features to lower AGA on the differential. Educating patients, barbers, and hairstylists about the importance of early intervention also may encourage earlier visits before the scarring process is advanced. Further exploration into factors impacting diagnosis and CCCA severity may uncover implications for prognosis and treatment.
This study was limited by a small sample size, retrospective design, and single-center analysis. Some patients had comorbid hair loss conditions, which could affect disease severity. Moreover, the central scalp alopecia photographic scale2 was not validated in men or designed for assessment of the nonclassical hair loss distributions noted in some of our patients. Nonetheless, we hope these data will support clinicians in efforts to advocate for early diagnosis and treatment in patients with CCCA to ultimately help improve outcomes.
- Ogunleye TA, McMichael A, Olsen EA. Central centrifugal cicatricial alopecia: what has been achieved, current clues for future research. Dermatol Clin. 2014;32:173-181. doi:10.1016/j.det.2013.12.005
- Olsen EA, Callender V, McMichael A, et al. Central hair loss in African American women: incidence and potential risk factors. J Am Acad Dermatol. 2011;64:245-252. doi:10.1016/j.jaad.2009.11.693
- Olsen EA, Callendar V, Sperling L, et al. Central scalp alopecia photographic scale in African American women. Dermatol Ther. 2008;21:264-267. doi:10.1111/j.1529-8019.2008.00208.x
- Andersen YMF, Nymand L, DeLozier AM, et al. Patient characteristics and disease burden of alopecia areata in the Danish Skin Cohort. BMJ Open. 2022;12:E053137. doi:10.1136/bmjopen-2021-053137
- Davis EC, Reid SD, Callender VD, et al. Differentiating central centrifugal cicatricial alopecia and androgenetic alopecia in African American men. J Clin Aesthetic Dermatol. 2012;5:37-40.
- Jackson TK, Sow Y, Ayoade KO, et al. Central centrifugal cicatricial alopecia in males. J Am Acad Dermatol. 2023;89:1136-1140. doi:10.1016/j.jaad.2023.07.1011
- Lawson CN, Bakayoko A, Callender VD. Central centrifugal cicatricial alopecia: challenges and treatments. Dermatol Clin. 2021;39:389-405. doi:10.1016/j.det.2021.03.004
To the Editor:
Central centrifugal cicatricial alopecia (CCCA) is a chronic progressive type of scarring alopecia that primarily affects women of African descent.1 The disorder rarely is reported in men, which may be due to misdiagnosis or delayed diagnosis. Early diagnosis and treatment are the cornerstones to slow or halt disease progression and prevent permanent damage to hair follicles. This study aimed to investigate the time to diagnosis and disease severity among males with CCCA.
We conducted a retrospective chart review of male patients older than 18 years seen in outpatient clinics at an academic dermatology department (Philadelphia, Pennsylvania) between January 2012 and December 2022. An electronic query using the International Classification of Diseases, Ninth and Tenth Revisions, code L66.9 (cicatricial alopecia, unspecified) was performed. Patients were included if they had a clinical diagnosis of CCCA, histologic evidence of CCCA, and scalp photographs from the initial dermatology visit. Patients with folliculitis decalvans, scalp biopsy features that limited characterization, or no scalp biopsy were excluded from the study. Onset of CCCA was defined as the patient-reported start time of hair loss and/or scalp symptoms. To determine alopecia severity, the degree of central scalp hair loss was independently assessed by 2 dermatologists (S.C.T., T.O.) using the central scalp alopecia photographic scale in African American women.2,3 This 6-point photographic scale displays images with grades ranging from 0 (normal) to 5 (bald scalp); higher grades indicate probable and more severe CCCA. The scale also divides the central hair loss in a frontal-accentuation or vertex-predominant pattern, which corresponds to the A or B designations, respectively; thus, a score of 5A indicates probable severe CCCA with a frontal accentuation pattern, while 5B indicates probable severe CCCA with hair loss focused on the vertex scalp. This study was approved by the University of Pennsylvania institutional review board (approval #850730).
Of 108 male patients, 12 met the eligibility criteria. Nearly all patients (91.7% [11/12]) had a CCCA severity grade of 3 or higher at the initial dermatology visit, indicating extensive hair loss (Table). The clinical appearance of severity grades 2 through 5 is demonstrated in the Figure. Among patients with a known disease duration prior to diagnosis, 72.7% (8/11) were diagnosed more than 1 year after onset of CCCA, and 45.4% (5/11) were diagnosed more than 5 years after onset. On average (SD), it took 6.4 (5.9) years for patients to receive a diagnosis of CCCA after the onset of scalp symptoms and/or hair loss.
Randomized controlled trials evaluating treatment of CCCA are lacking, and anecdotal evidence posits a better treatment response in early CCCA; however, our results suggest that most male patients present with advanced CCCA and receive a diagnosis years after disease onset. Similar research in alopecia areata has shown that 72.4% (105/145) of patients received their diagnosis within a year after onset of symptoms, and the mean time from onset of symptoms to diagnosis was 1 year.4 In contrast, male patients with CCCA experience considerable diagnostic delays. This disparity indicates the need for clinicians to increase recognition of CCCA in men and quickly refer them to a dermatologist for prompt treatment.
Androgenetic alopecia (AGA) commonly is at the top of the differential diagnosis for hair loss on the vertex of the scalp in males, but clinicians should maintain a high index of suspicion for CCCA, especially when scalp symptoms or atypical features of AGA are present.5 Androgenetic alopecia typically is asymptomatic, whereas the symptoms of CCCA may include itching, tenderness, and/or burning.6,7 Trichoscopy is useful to evaluate for scarring, and a scalp biopsy may reveal other features to lower AGA on the differential. Educating patients, barbers, and hairstylists about the importance of early intervention also may encourage earlier visits before the scarring process is advanced. Further exploration into factors impacting diagnosis and CCCA severity may uncover implications for prognosis and treatment.
This study was limited by a small sample size, retrospective design, and single-center analysis. Some patients had comorbid hair loss conditions, which could affect disease severity. Moreover, the central scalp alopecia photographic scale2 was not validated in men or designed for assessment of the nonclassical hair loss distributions noted in some of our patients. Nonetheless, we hope these data will support clinicians in efforts to advocate for early diagnosis and treatment in patients with CCCA to ultimately help improve outcomes.
To the Editor:
Central centrifugal cicatricial alopecia (CCCA) is a chronic progressive type of scarring alopecia that primarily affects women of African descent.1 The disorder rarely is reported in men, which may be due to misdiagnosis or delayed diagnosis. Early diagnosis and treatment are the cornerstones to slow or halt disease progression and prevent permanent damage to hair follicles. This study aimed to investigate the time to diagnosis and disease severity among males with CCCA.
We conducted a retrospective chart review of male patients older than 18 years seen in outpatient clinics at an academic dermatology department (Philadelphia, Pennsylvania) between January 2012 and December 2022. An electronic query using the International Classification of Diseases, Ninth and Tenth Revisions, code L66.9 (cicatricial alopecia, unspecified) was performed. Patients were included if they had a clinical diagnosis of CCCA, histologic evidence of CCCA, and scalp photographs from the initial dermatology visit. Patients with folliculitis decalvans, scalp biopsy features that limited characterization, or no scalp biopsy were excluded from the study. Onset of CCCA was defined as the patient-reported start time of hair loss and/or scalp symptoms. To determine alopecia severity, the degree of central scalp hair loss was independently assessed by 2 dermatologists (S.C.T., T.O.) using the central scalp alopecia photographic scale in African American women.2,3 This 6-point photographic scale displays images with grades ranging from 0 (normal) to 5 (bald scalp); higher grades indicate probable and more severe CCCA. The scale also divides the central hair loss in a frontal-accentuation or vertex-predominant pattern, which corresponds to the A or B designations, respectively; thus, a score of 5A indicates probable severe CCCA with a frontal accentuation pattern, while 5B indicates probable severe CCCA with hair loss focused on the vertex scalp. This study was approved by the University of Pennsylvania institutional review board (approval #850730).
Of 108 male patients, 12 met the eligibility criteria. Nearly all patients (91.7% [11/12]) had a CCCA severity grade of 3 or higher at the initial dermatology visit, indicating extensive hair loss (Table). The clinical appearance of severity grades 2 through 5 is demonstrated in the Figure. Among patients with a known disease duration prior to diagnosis, 72.7% (8/11) were diagnosed more than 1 year after onset of CCCA, and 45.4% (5/11) were diagnosed more than 5 years after onset. On average (SD), it took 6.4 (5.9) years for patients to receive a diagnosis of CCCA after the onset of scalp symptoms and/or hair loss.
Randomized controlled trials evaluating treatment of CCCA are lacking, and anecdotal evidence posits a better treatment response in early CCCA; however, our results suggest that most male patients present with advanced CCCA and receive a diagnosis years after disease onset. Similar research in alopecia areata has shown that 72.4% (105/145) of patients received their diagnosis within a year after onset of symptoms, and the mean time from onset of symptoms to diagnosis was 1 year.4 In contrast, male patients with CCCA experience considerable diagnostic delays. This disparity indicates the need for clinicians to increase recognition of CCCA in men and quickly refer them to a dermatologist for prompt treatment.
Androgenetic alopecia (AGA) commonly is at the top of the differential diagnosis for hair loss on the vertex of the scalp in males, but clinicians should maintain a high index of suspicion for CCCA, especially when scalp symptoms or atypical features of AGA are present.5 Androgenetic alopecia typically is asymptomatic, whereas the symptoms of CCCA may include itching, tenderness, and/or burning.6,7 Trichoscopy is useful to evaluate for scarring, and a scalp biopsy may reveal other features to lower AGA on the differential. Educating patients, barbers, and hairstylists about the importance of early intervention also may encourage earlier visits before the scarring process is advanced. Further exploration into factors impacting diagnosis and CCCA severity may uncover implications for prognosis and treatment.
This study was limited by a small sample size, retrospective design, and single-center analysis. Some patients had comorbid hair loss conditions, which could affect disease severity. Moreover, the central scalp alopecia photographic scale2 was not validated in men or designed for assessment of the nonclassical hair loss distributions noted in some of our patients. Nonetheless, we hope these data will support clinicians in efforts to advocate for early diagnosis and treatment in patients with CCCA to ultimately help improve outcomes.
- Ogunleye TA, McMichael A, Olsen EA. Central centrifugal cicatricial alopecia: what has been achieved, current clues for future research. Dermatol Clin. 2014;32:173-181. doi:10.1016/j.det.2013.12.005
- Olsen EA, Callender V, McMichael A, et al. Central hair loss in African American women: incidence and potential risk factors. J Am Acad Dermatol. 2011;64:245-252. doi:10.1016/j.jaad.2009.11.693
- Olsen EA, Callendar V, Sperling L, et al. Central scalp alopecia photographic scale in African American women. Dermatol Ther. 2008;21:264-267. doi:10.1111/j.1529-8019.2008.00208.x
- Andersen YMF, Nymand L, DeLozier AM, et al. Patient characteristics and disease burden of alopecia areata in the Danish Skin Cohort. BMJ Open. 2022;12:E053137. doi:10.1136/bmjopen-2021-053137
- Davis EC, Reid SD, Callender VD, et al. Differentiating central centrifugal cicatricial alopecia and androgenetic alopecia in African American men. J Clin Aesthetic Dermatol. 2012;5:37-40.
- Jackson TK, Sow Y, Ayoade KO, et al. Central centrifugal cicatricial alopecia in males. J Am Acad Dermatol. 2023;89:1136-1140. doi:10.1016/j.jaad.2023.07.1011
- Lawson CN, Bakayoko A, Callender VD. Central centrifugal cicatricial alopecia: challenges and treatments. Dermatol Clin. 2021;39:389-405. doi:10.1016/j.det.2021.03.004
- Ogunleye TA, McMichael A, Olsen EA. Central centrifugal cicatricial alopecia: what has been achieved, current clues for future research. Dermatol Clin. 2014;32:173-181. doi:10.1016/j.det.2013.12.005
- Olsen EA, Callender V, McMichael A, et al. Central hair loss in African American women: incidence and potential risk factors. J Am Acad Dermatol. 2011;64:245-252. doi:10.1016/j.jaad.2009.11.693
- Olsen EA, Callendar V, Sperling L, et al. Central scalp alopecia photographic scale in African American women. Dermatol Ther. 2008;21:264-267. doi:10.1111/j.1529-8019.2008.00208.x
- Andersen YMF, Nymand L, DeLozier AM, et al. Patient characteristics and disease burden of alopecia areata in the Danish Skin Cohort. BMJ Open. 2022;12:E053137. doi:10.1136/bmjopen-2021-053137
- Davis EC, Reid SD, Callender VD, et al. Differentiating central centrifugal cicatricial alopecia and androgenetic alopecia in African American men. J Clin Aesthetic Dermatol. 2012;5:37-40.
- Jackson TK, Sow Y, Ayoade KO, et al. Central centrifugal cicatricial alopecia in males. J Am Acad Dermatol. 2023;89:1136-1140. doi:10.1016/j.jaad.2023.07.1011
- Lawson CN, Bakayoko A, Callender VD. Central centrifugal cicatricial alopecia: challenges and treatments. Dermatol Clin. 2021;39:389-405. doi:10.1016/j.det.2021.03.004
Practice Points
- Most males with central centrifugal cicatricial alopecia (CCCA) experience considerable diagnostic delays and typically present to dermatology with late-stage disease.
- Dermatologists should consider CCCA in the differential diagnosis for adult Black males with alopecia.
- More research is needed to explore advanced CCCA in males, including factors limiting timely diagnosis and the impact on quality of life in this population.

The Impact of the Recent Supreme Court Ruling on the Dermatology Recruitment Pipeline
The ruling by the Supreme Court of the United States (SCOTUS) in 20231,2 on the use of race-based criteria in college admissions was met with a range of reactions across the country. Given the implications of this decision on the future makeup of higher education, the downstream effects on medical school admissions, and the possible further impact on graduate medical education programs, we sought to explore the potential impact of the landmark decision from the perspective of dermatology residency program directors and offer insights on this pivotal judgment.
Background on the SCOTUS Ruling
In June 2023, SCOTUS issued its formal decision on 2 court cases brought by the organization Students for Fair Admissions (SFFA) against the University of North Carolina at Chapel Hill1 and Harvard University (Cambridge, Massachusetts)2 that addressed college admissions practices dealing with the use of race as a selection criterion in the application process. The cases alleged that these universities had overly emphasized race in the admissions process and thus were in violation of the Civil Rights Act of 1964 as well as the 14th Amendment.1,2
The SCOTUS justices voted 6 to 3 in favor of the argument presented by the SFFA, determining that the use of race in the college admissions process essentially constituted a form of racial discrimination. The ruling was in contrast to a prior decision in 2003 that centered on law school admissions at the University of Michigan (Ann Arbor, Michigan) in which SCOTUS previously had determined that race could be used as one factor amongst other criteria in the higher education selection process.3 In the 2023 decision siding with SFFA, SCOTUS did acknowledge that it was still acceptable for selection processes to consider “an applicant’s discussion of how race affected his or her life, be it through discrimination, inspiration, or otherwise.”2
Effect on Undergraduate Admissions
Prior to the 2023 ruling, several states had already passed independent laws against the use of affirmative action or race-based selection criteria in the admissions process at public colleges and universities.4 As a result, these institutions would already be conforming to the principles set forth in the SCOTUS ruling and major changes to their undergraduate admissions policies would not be expected; however, a considerable number of colleges and universities—particularly those considered highly selective with applicant acceptance rates that are well below the national average—reported the use of race as a factor in their admissions processes in standardized reporting surveys.5 For these institutions, it is no longer considered acceptable (based on the SCOTUS decision) to use race as a singular factor in admissions or to implement race-conscious decision-making—in which individuals are considered differently based solely on their race—as part of the undergraduate selection process.
In light of these rulings, many institutions have explicitly committed to upholding principles of diversity in their recruitment processes, acknowledging the multifaceted nature of diversity beyond strictly racial terms—including but not limited to socioeconomic diversity, religious diversity, or gender diversity—which is in compliance with the interpretation ruling by the US Department of Education and the US Department of Justice.6 Additionally, select institutions have taken approaches to explicitly include questions on ways in which applicants have overcome obstacles or challenges, allowing an opportunity for individuals who have had such experiences related to race an opportunity to incorporate these elements into their applications. Finally, some institutions have taken a more limited approach, eliminating ways in which race is explicitly addressed in the application and focusing on race-neutral elements of the application in their approach to selection.7
Because the first college admission cycle since the 2023 SCOTUS ruling is still underway, we have yet to witness the full impact of this decision on the current undergraduate admissions landscape.
Effect on Medical School Admissions and Rotations
Although SCOTUS specifically examined the undergraduate admissions process, the ruling on race-conscious admissions also had a profound impact on graduate school admissions including medical school admission processes.1,2,8,9 This is because the language of the majority opinion refers to “university programs” in its ruling, which also has been broadly interpreted to include graduate school programs. As with undergraduate admissions, it has been interpreted by national medical education organizations and institutions that medical schools also cannot consider an applicant’s race or ethnicity as a specific factor in the admissions process.1,2,8,9
Lived individual experiences, including essays that speak to an applicant’s lived experiences and career aspirations related to race, still can be taken into account. In particular, holistic review still can be utilized to evaluate medical school candidates and may play a more integral role in the medical school admissions process now than in the past.8,10,11 After the ruling, Justice Sonia Sotomayor noted that “today’s decision leaves intact holistic college admissions and recruitment efforts that seek to enroll diverse classes without using racial classifications.”1
The ruling asserted that universities may define their mission as they see fit. As a result, the ruling did not affect medical school missions or strategic plans, including those that may aim to diversify the health care workforce.8,10,11 The ruling also did not affect the ability to utilize pathway programs to encourage a career in medicine or recruitment relationships with diverse undergraduate or community-based organizations. Student interest groups also can be involved in the relationship-building or recruitment activities for medical schools.8,10,11 Guidance from the US Department of Education and US Department of Justice noted that institutions may consider race in identifying prospective applicants through recruitment and outreach, “provided that their outreach and recruitment programs do not provide targeted groups of prospective students preference in the admissions process, and provided that all students—whether part of a specifically targeted group or not—enjoy the same opportunity to apply and compete for admission.”12
In regard to pathways programs, slots cannot be reserved and preference cannot be given to applicants who participated in these programs if race was a factor in selecting participants.8 Similarly, medical school away electives related to diversity cannot be reserved for those of a specific race or ethnicity; however, these electives can utilize commitment to stated aims and missions of the rotation, such as a commitment to diversity within medicine, as a basis to selecting candidates.8
The ruling did not address how race or ethnicity is factored into financial aid or scholarship determination. There has been concern in higher education that the legal framework utilized in the SCOTUS decision could affect financial aid and scholarship decisions; therefore, many institutions are proceeding with caution in their approach.8
Effect on Residency Selection
Because the SCOTUS ruling references colleges and universities, not health care employers, it should not affect the residency selection process; however, there is variability in how health care institutions are interpreting the impact of the ruling on residency selection, with some taking a more prescriptive and cautious view on the matter. Additionally, with that said, residency selection is considered an employment practice covered by Title VII of the Civil Rights Act of 1964,13 which already prohibits the consideration of race in hiring decisions.7 Under Title VII, it is unlawful for employers to discriminate against someone because of race, color, religion, sex, or national origin, and it is “unlawful to use policies or practices that seem neutral but have the effect of discriminating against people because of their race, color, religion, sex … or national origin.” Title VII also states that employers cannot “make employment decisions based on stereotypes or assumptions about a person’s abilities, traits, or performance because of their race, color, religion, sex … or national origin.”13
Importantly, Title VII does not imply that employers need to abandon their diversity, equity, or inclusion initiatives, and it does not imply that employers must revoke their mission to improve diversity in the workforce. Title VII does not state that racial information cannot be available. It would be permissible to use racial data to assess recruitment trends, identify inequities, and create programs to eliminate barriers and decrease bias14; for example, if a program identified that, based on their current review system, students who are underrepresented in medicine were disproportionately screened out of the applicant pool or interview group, they may wish to revisit their review process to identify and eliminate possible biases. Programs also may wish to adopt educational programs for reviewers (eg, implicit bias training) or educational content on the potential for bias in commonly used review criteria, such as the US Medical Licensing Examination, clerkship grades, and the Medical Student Performance Evaluation.15 Reviewers can and should consider applications in an individualized and holistic manner in which experiences, traits, skills, and academic metrics are assessed together for compatibility with the values and mission of the training program.16
Future Directions for Dermatology
Beyond the SCOTUS ruling, there have been other shifts in the dermatology residency application process that have affected candidate review. Dermatology programs recently have adopted the use of preference signaling in residency applications. Preliminary data from the Association of American Medical Colleges for the 2024 application cycle indicated that of the 81 programs analyzed, there was a nearly 0% chance of an applicant receiving an interview invitation from a program that they did not signal. The median signal-to-interview conversion rate for the 81 dermatology programs analyzed was 55% for gold signals and 15% for silver signals.17 It can be inferred from these data that programs are using preference signaling as important criteria for consideration of interview invitation. Programs may choose to focus most of their attention on the applicant pool who has signaled them. Because the number and type of signals available is equal among all applicants, we hope that this provides an equitable way for all applicants to garner holistic review from programs that interested them. In addition, there has been a 30% decrease in average applications submitted per dermatology applicant.18 With a substantial decline in applications to dermatology, we hope that reviewers are able to spend more time devoted to comprehensive holistic review.
Although signals are equitable for applicants, their distribution among programs may not be; for example, in a given year, a program might find that all their gold signals came from non–underrepresented in medicine students. We encourage programs to carefully review applicant data to ensure their recruitment process is not inadvertently discriminatory and is in alignment with their goals and mission.
- Students for Fair Admissions, Inc. v University of North Carolina, 567 F. Supp. 3d 580 (M.D.N.C. 2021).
- Students for Fair Admissions, Inc. v President and Fellows of Harvard College, 600 US ___ (2023).
- Grutter v Bollinger, 539 US 306 (2003).
- Saul S. 9 states have banned affirmative action. here’s what that looks like. The New York Times. October 31, 2022. https://www.nytimes.com/2022/10/31/us/politics/affirmative-action-ban-states.html
- Desilver D. Private, selective colleges are most likely to use race, ethnicity as a factor in admissions decisions. Pew Research Center. July 14, 2023. Accessed May 29, 2024. https://www.pewresearch.org/short-reads/2023/07/14/private-selective-colleges-are-most-likely-to-use-race-ethnicity-as-a-factor-in-admissions-decisions/
- US Department of Education. Justice and education departments release resources to advance diversity and opportunity in higher education. August 14, 2023. Accessed May 17, 2024. https://www.ed.gov/news/press-releases/advance-diversity-and-opportunity-higher-education-justice-and-education-departments-release-resources-advance-diversity-and-opportunity-higher-education
- Amponsah MN, Hamid RD. Harvard overhauls college application in wake of affirmative action decision. The Harvard Crimson. August 3, 2023. Accessed May 17, 2024. https://www.thecrimson.com/article/2023/8/3/harvard-admission-essay-change/
- Association of American Medical Colleges. Frequently asked questions: what does the Harvard and UNC decision mean for medical education? August 24, 2023. Accessed May 17, 2024. https://www.aamc.org/media/68771/download?attachment%3Fattachment
- American Medical Association. Affirmative action ends: how Supreme Court ruling impacts medical schools & the health care workforce. July 7, 2023. Accessed May 17, 2024. https://www.ama-assn.org/medical-students/medical-school-life/affirmative-action-ends-how-supreme-court-ruling-impacts
- Association of American Medical Colleges. How can medical schools boost racial diversity in the wake of the recent Supreme Court ruling? July 27, 2023. Accessed May 17, 2024. https://www.aamc.org/news/how-can-medical-schools-boost-racial-diversity-wake-recent-supreme-court-ruling
- Association of American Medical Colleges. Diversity in medical school admissions. Updated March 18, 2024. Accessed May 17, 2024. https://www.aamc.org/about-us/mission-areas/medical-education/diversity-medical-school-admissions
- United States Department of Justice. Questions and answers regarding the Supreme Court’s decision in Students For Fair Admissions, Inc. v. Harvard College and University of North Carolina. August 14, 2023. Accessed May 29, 2024. https://www.justice.gov/d9/2023-08/post-sffa_resource_faq_final_508.pdf
- US Department of Justice. Title VII of the Civil Rights Act of 1964. Accessed May 17, 2024. https://www.justice.gov/crt/laws-we-enforce
- Zheng L. How to effectively—and legally—use racial data for DEI. Harvard Business Review. July 24, 2023. Accessed May 17, 2024. https://hbr.org/2023/07/how-to-effectively-and-legally-use-racial-data-for-dei
- Crites K, Johnson J, Scott N, et al. Increasing diversity in residency training programs. Cureus. 2022;14:E25962. doi:10.7759/cureus.25962
- Association of American Medical Colleges. Holistic principles in resident selection: an introduction. Accessed May 17, 2024. https://www.aamc.org/media/44586/download?attachment
- Association of American Medical Colleges. Exploring the relationship between program signaling & interview invitations across specialties 2024 ERAS® preliminary analysis. December 29, 2023. Accessed May 17, 2024. https://www.aamc.org/media/74811/download?attachment
- Association of American Medical Colleges. Preliminary program signaling data and their impact on residency selection. October 24, 2023. Accessed May 17, 2024. https://www.aamc.org/services/eras-institutions/program-signaling-data#:~:text=Preliminary%20Program%20Signaling%20Data%20and%20Their%20Impact%20on%20Residency%20Selection,-Oct.&text=Program%20signals%20are%20a%20mechanism,whom%20to%20invite%20for%20interview
The ruling by the Supreme Court of the United States (SCOTUS) in 20231,2 on the use of race-based criteria in college admissions was met with a range of reactions across the country. Given the implications of this decision on the future makeup of higher education, the downstream effects on medical school admissions, and the possible further impact on graduate medical education programs, we sought to explore the potential impact of the landmark decision from the perspective of dermatology residency program directors and offer insights on this pivotal judgment.
Background on the SCOTUS Ruling
In June 2023, SCOTUS issued its formal decision on 2 court cases brought by the organization Students for Fair Admissions (SFFA) against the University of North Carolina at Chapel Hill1 and Harvard University (Cambridge, Massachusetts)2 that addressed college admissions practices dealing with the use of race as a selection criterion in the application process. The cases alleged that these universities had overly emphasized race in the admissions process and thus were in violation of the Civil Rights Act of 1964 as well as the 14th Amendment.1,2
The SCOTUS justices voted 6 to 3 in favor of the argument presented by the SFFA, determining that the use of race in the college admissions process essentially constituted a form of racial discrimination. The ruling was in contrast to a prior decision in 2003 that centered on law school admissions at the University of Michigan (Ann Arbor, Michigan) in which SCOTUS previously had determined that race could be used as one factor amongst other criteria in the higher education selection process.3 In the 2023 decision siding with SFFA, SCOTUS did acknowledge that it was still acceptable for selection processes to consider “an applicant’s discussion of how race affected his or her life, be it through discrimination, inspiration, or otherwise.”2
Effect on Undergraduate Admissions
Prior to the 2023 ruling, several states had already passed independent laws against the use of affirmative action or race-based selection criteria in the admissions process at public colleges and universities.4 As a result, these institutions would already be conforming to the principles set forth in the SCOTUS ruling and major changes to their undergraduate admissions policies would not be expected; however, a considerable number of colleges and universities—particularly those considered highly selective with applicant acceptance rates that are well below the national average—reported the use of race as a factor in their admissions processes in standardized reporting surveys.5 For these institutions, it is no longer considered acceptable (based on the SCOTUS decision) to use race as a singular factor in admissions or to implement race-conscious decision-making—in which individuals are considered differently based solely on their race—as part of the undergraduate selection process.
In light of these rulings, many institutions have explicitly committed to upholding principles of diversity in their recruitment processes, acknowledging the multifaceted nature of diversity beyond strictly racial terms—including but not limited to socioeconomic diversity, religious diversity, or gender diversity—which is in compliance with the interpretation ruling by the US Department of Education and the US Department of Justice.6 Additionally, select institutions have taken approaches to explicitly include questions on ways in which applicants have overcome obstacles or challenges, allowing an opportunity for individuals who have had such experiences related to race an opportunity to incorporate these elements into their applications. Finally, some institutions have taken a more limited approach, eliminating ways in which race is explicitly addressed in the application and focusing on race-neutral elements of the application in their approach to selection.7
Because the first college admission cycle since the 2023 SCOTUS ruling is still underway, we have yet to witness the full impact of this decision on the current undergraduate admissions landscape.
Effect on Medical School Admissions and Rotations
Although SCOTUS specifically examined the undergraduate admissions process, the ruling on race-conscious admissions also had a profound impact on graduate school admissions including medical school admission processes.1,2,8,9 This is because the language of the majority opinion refers to “university programs” in its ruling, which also has been broadly interpreted to include graduate school programs. As with undergraduate admissions, it has been interpreted by national medical education organizations and institutions that medical schools also cannot consider an applicant’s race or ethnicity as a specific factor in the admissions process.1,2,8,9
Lived individual experiences, including essays that speak to an applicant’s lived experiences and career aspirations related to race, still can be taken into account. In particular, holistic review still can be utilized to evaluate medical school candidates and may play a more integral role in the medical school admissions process now than in the past.8,10,11 After the ruling, Justice Sonia Sotomayor noted that “today’s decision leaves intact holistic college admissions and recruitment efforts that seek to enroll diverse classes without using racial classifications.”1
The ruling asserted that universities may define their mission as they see fit. As a result, the ruling did not affect medical school missions or strategic plans, including those that may aim to diversify the health care workforce.8,10,11 The ruling also did not affect the ability to utilize pathway programs to encourage a career in medicine or recruitment relationships with diverse undergraduate or community-based organizations. Student interest groups also can be involved in the relationship-building or recruitment activities for medical schools.8,10,11 Guidance from the US Department of Education and US Department of Justice noted that institutions may consider race in identifying prospective applicants through recruitment and outreach, “provided that their outreach and recruitment programs do not provide targeted groups of prospective students preference in the admissions process, and provided that all students—whether part of a specifically targeted group or not—enjoy the same opportunity to apply and compete for admission.”12
In regard to pathways programs, slots cannot be reserved and preference cannot be given to applicants who participated in these programs if race was a factor in selecting participants.8 Similarly, medical school away electives related to diversity cannot be reserved for those of a specific race or ethnicity; however, these electives can utilize commitment to stated aims and missions of the rotation, such as a commitment to diversity within medicine, as a basis to selecting candidates.8
The ruling did not address how race or ethnicity is factored into financial aid or scholarship determination. There has been concern in higher education that the legal framework utilized in the SCOTUS decision could affect financial aid and scholarship decisions; therefore, many institutions are proceeding with caution in their approach.8
Effect on Residency Selection
Because the SCOTUS ruling references colleges and universities, not health care employers, it should not affect the residency selection process; however, there is variability in how health care institutions are interpreting the impact of the ruling on residency selection, with some taking a more prescriptive and cautious view on the matter. Additionally, with that said, residency selection is considered an employment practice covered by Title VII of the Civil Rights Act of 1964,13 which already prohibits the consideration of race in hiring decisions.7 Under Title VII, it is unlawful for employers to discriminate against someone because of race, color, religion, sex, or national origin, and it is “unlawful to use policies or practices that seem neutral but have the effect of discriminating against people because of their race, color, religion, sex … or national origin.” Title VII also states that employers cannot “make employment decisions based on stereotypes or assumptions about a person’s abilities, traits, or performance because of their race, color, religion, sex … or national origin.”13
Importantly, Title VII does not imply that employers need to abandon their diversity, equity, or inclusion initiatives, and it does not imply that employers must revoke their mission to improve diversity in the workforce. Title VII does not state that racial information cannot be available. It would be permissible to use racial data to assess recruitment trends, identify inequities, and create programs to eliminate barriers and decrease bias14; for example, if a program identified that, based on their current review system, students who are underrepresented in medicine were disproportionately screened out of the applicant pool or interview group, they may wish to revisit their review process to identify and eliminate possible biases. Programs also may wish to adopt educational programs for reviewers (eg, implicit bias training) or educational content on the potential for bias in commonly used review criteria, such as the US Medical Licensing Examination, clerkship grades, and the Medical Student Performance Evaluation.15 Reviewers can and should consider applications in an individualized and holistic manner in which experiences, traits, skills, and academic metrics are assessed together for compatibility with the values and mission of the training program.16
Future Directions for Dermatology
Beyond the SCOTUS ruling, there have been other shifts in the dermatology residency application process that have affected candidate review. Dermatology programs recently have adopted the use of preference signaling in residency applications. Preliminary data from the Association of American Medical Colleges for the 2024 application cycle indicated that of the 81 programs analyzed, there was a nearly 0% chance of an applicant receiving an interview invitation from a program that they did not signal. The median signal-to-interview conversion rate for the 81 dermatology programs analyzed was 55% for gold signals and 15% for silver signals.17 It can be inferred from these data that programs are using preference signaling as important criteria for consideration of interview invitation. Programs may choose to focus most of their attention on the applicant pool who has signaled them. Because the number and type of signals available is equal among all applicants, we hope that this provides an equitable way for all applicants to garner holistic review from programs that interested them. In addition, there has been a 30% decrease in average applications submitted per dermatology applicant.18 With a substantial decline in applications to dermatology, we hope that reviewers are able to spend more time devoted to comprehensive holistic review.
Although signals are equitable for applicants, their distribution among programs may not be; for example, in a given year, a program might find that all their gold signals came from non–underrepresented in medicine students. We encourage programs to carefully review applicant data to ensure their recruitment process is not inadvertently discriminatory and is in alignment with their goals and mission.
The ruling by the Supreme Court of the United States (SCOTUS) in 20231,2 on the use of race-based criteria in college admissions was met with a range of reactions across the country. Given the implications of this decision on the future makeup of higher education, the downstream effects on medical school admissions, and the possible further impact on graduate medical education programs, we sought to explore the potential impact of the landmark decision from the perspective of dermatology residency program directors and offer insights on this pivotal judgment.
Background on the SCOTUS Ruling
In June 2023, SCOTUS issued its formal decision on 2 court cases brought by the organization Students for Fair Admissions (SFFA) against the University of North Carolina at Chapel Hill1 and Harvard University (Cambridge, Massachusetts)2 that addressed college admissions practices dealing with the use of race as a selection criterion in the application process. The cases alleged that these universities had overly emphasized race in the admissions process and thus were in violation of the Civil Rights Act of 1964 as well as the 14th Amendment.1,2
The SCOTUS justices voted 6 to 3 in favor of the argument presented by the SFFA, determining that the use of race in the college admissions process essentially constituted a form of racial discrimination. The ruling was in contrast to a prior decision in 2003 that centered on law school admissions at the University of Michigan (Ann Arbor, Michigan) in which SCOTUS previously had determined that race could be used as one factor amongst other criteria in the higher education selection process.3 In the 2023 decision siding with SFFA, SCOTUS did acknowledge that it was still acceptable for selection processes to consider “an applicant’s discussion of how race affected his or her life, be it through discrimination, inspiration, or otherwise.”2
Effect on Undergraduate Admissions
Prior to the 2023 ruling, several states had already passed independent laws against the use of affirmative action or race-based selection criteria in the admissions process at public colleges and universities.4 As a result, these institutions would already be conforming to the principles set forth in the SCOTUS ruling and major changes to their undergraduate admissions policies would not be expected; however, a considerable number of colleges and universities—particularly those considered highly selective with applicant acceptance rates that are well below the national average—reported the use of race as a factor in their admissions processes in standardized reporting surveys.5 For these institutions, it is no longer considered acceptable (based on the SCOTUS decision) to use race as a singular factor in admissions or to implement race-conscious decision-making—in which individuals are considered differently based solely on their race—as part of the undergraduate selection process.
In light of these rulings, many institutions have explicitly committed to upholding principles of diversity in their recruitment processes, acknowledging the multifaceted nature of diversity beyond strictly racial terms—including but not limited to socioeconomic diversity, religious diversity, or gender diversity—which is in compliance with the interpretation ruling by the US Department of Education and the US Department of Justice.6 Additionally, select institutions have taken approaches to explicitly include questions on ways in which applicants have overcome obstacles or challenges, allowing an opportunity for individuals who have had such experiences related to race an opportunity to incorporate these elements into their applications. Finally, some institutions have taken a more limited approach, eliminating ways in which race is explicitly addressed in the application and focusing on race-neutral elements of the application in their approach to selection.7
Because the first college admission cycle since the 2023 SCOTUS ruling is still underway, we have yet to witness the full impact of this decision on the current undergraduate admissions landscape.
Effect on Medical School Admissions and Rotations
Although SCOTUS specifically examined the undergraduate admissions process, the ruling on race-conscious admissions also had a profound impact on graduate school admissions including medical school admission processes.1,2,8,9 This is because the language of the majority opinion refers to “university programs” in its ruling, which also has been broadly interpreted to include graduate school programs. As with undergraduate admissions, it has been interpreted by national medical education organizations and institutions that medical schools also cannot consider an applicant’s race or ethnicity as a specific factor in the admissions process.1,2,8,9
Lived individual experiences, including essays that speak to an applicant’s lived experiences and career aspirations related to race, still can be taken into account. In particular, holistic review still can be utilized to evaluate medical school candidates and may play a more integral role in the medical school admissions process now than in the past.8,10,11 After the ruling, Justice Sonia Sotomayor noted that “today’s decision leaves intact holistic college admissions and recruitment efforts that seek to enroll diverse classes without using racial classifications.”1
The ruling asserted that universities may define their mission as they see fit. As a result, the ruling did not affect medical school missions or strategic plans, including those that may aim to diversify the health care workforce.8,10,11 The ruling also did not affect the ability to utilize pathway programs to encourage a career in medicine or recruitment relationships with diverse undergraduate or community-based organizations. Student interest groups also can be involved in the relationship-building or recruitment activities for medical schools.8,10,11 Guidance from the US Department of Education and US Department of Justice noted that institutions may consider race in identifying prospective applicants through recruitment and outreach, “provided that their outreach and recruitment programs do not provide targeted groups of prospective students preference in the admissions process, and provided that all students—whether part of a specifically targeted group or not—enjoy the same opportunity to apply and compete for admission.”12
In regard to pathways programs, slots cannot be reserved and preference cannot be given to applicants who participated in these programs if race was a factor in selecting participants.8 Similarly, medical school away electives related to diversity cannot be reserved for those of a specific race or ethnicity; however, these electives can utilize commitment to stated aims and missions of the rotation, such as a commitment to diversity within medicine, as a basis to selecting candidates.8
The ruling did not address how race or ethnicity is factored into financial aid or scholarship determination. There has been concern in higher education that the legal framework utilized in the SCOTUS decision could affect financial aid and scholarship decisions; therefore, many institutions are proceeding with caution in their approach.8
Effect on Residency Selection
Because the SCOTUS ruling references colleges and universities, not health care employers, it should not affect the residency selection process; however, there is variability in how health care institutions are interpreting the impact of the ruling on residency selection, with some taking a more prescriptive and cautious view on the matter. Additionally, with that said, residency selection is considered an employment practice covered by Title VII of the Civil Rights Act of 1964,13 which already prohibits the consideration of race in hiring decisions.7 Under Title VII, it is unlawful for employers to discriminate against someone because of race, color, religion, sex, or national origin, and it is “unlawful to use policies or practices that seem neutral but have the effect of discriminating against people because of their race, color, religion, sex … or national origin.” Title VII also states that employers cannot “make employment decisions based on stereotypes or assumptions about a person’s abilities, traits, or performance because of their race, color, religion, sex … or national origin.”13
Importantly, Title VII does not imply that employers need to abandon their diversity, equity, or inclusion initiatives, and it does not imply that employers must revoke their mission to improve diversity in the workforce. Title VII does not state that racial information cannot be available. It would be permissible to use racial data to assess recruitment trends, identify inequities, and create programs to eliminate barriers and decrease bias14; for example, if a program identified that, based on their current review system, students who are underrepresented in medicine were disproportionately screened out of the applicant pool or interview group, they may wish to revisit their review process to identify and eliminate possible biases. Programs also may wish to adopt educational programs for reviewers (eg, implicit bias training) or educational content on the potential for bias in commonly used review criteria, such as the US Medical Licensing Examination, clerkship grades, and the Medical Student Performance Evaluation.15 Reviewers can and should consider applications in an individualized and holistic manner in which experiences, traits, skills, and academic metrics are assessed together for compatibility with the values and mission of the training program.16
Future Directions for Dermatology
Beyond the SCOTUS ruling, there have been other shifts in the dermatology residency application process that have affected candidate review. Dermatology programs recently have adopted the use of preference signaling in residency applications. Preliminary data from the Association of American Medical Colleges for the 2024 application cycle indicated that of the 81 programs analyzed, there was a nearly 0% chance of an applicant receiving an interview invitation from a program that they did not signal. The median signal-to-interview conversion rate for the 81 dermatology programs analyzed was 55% for gold signals and 15% for silver signals.17 It can be inferred from these data that programs are using preference signaling as important criteria for consideration of interview invitation. Programs may choose to focus most of their attention on the applicant pool who has signaled them. Because the number and type of signals available is equal among all applicants, we hope that this provides an equitable way for all applicants to garner holistic review from programs that interested them. In addition, there has been a 30% decrease in average applications submitted per dermatology applicant.18 With a substantial decline in applications to dermatology, we hope that reviewers are able to spend more time devoted to comprehensive holistic review.
Although signals are equitable for applicants, their distribution among programs may not be; for example, in a given year, a program might find that all their gold signals came from non–underrepresented in medicine students. We encourage programs to carefully review applicant data to ensure their recruitment process is not inadvertently discriminatory and is in alignment with their goals and mission.
- Students for Fair Admissions, Inc. v University of North Carolina, 567 F. Supp. 3d 580 (M.D.N.C. 2021).
- Students for Fair Admissions, Inc. v President and Fellows of Harvard College, 600 US ___ (2023).
- Grutter v Bollinger, 539 US 306 (2003).
- Saul S. 9 states have banned affirmative action. here’s what that looks like. The New York Times. October 31, 2022. https://www.nytimes.com/2022/10/31/us/politics/affirmative-action-ban-states.html
- Desilver D. Private, selective colleges are most likely to use race, ethnicity as a factor in admissions decisions. Pew Research Center. July 14, 2023. Accessed May 29, 2024. https://www.pewresearch.org/short-reads/2023/07/14/private-selective-colleges-are-most-likely-to-use-race-ethnicity-as-a-factor-in-admissions-decisions/
- US Department of Education. Justice and education departments release resources to advance diversity and opportunity in higher education. August 14, 2023. Accessed May 17, 2024. https://www.ed.gov/news/press-releases/advance-diversity-and-opportunity-higher-education-justice-and-education-departments-release-resources-advance-diversity-and-opportunity-higher-education
- Amponsah MN, Hamid RD. Harvard overhauls college application in wake of affirmative action decision. The Harvard Crimson. August 3, 2023. Accessed May 17, 2024. https://www.thecrimson.com/article/2023/8/3/harvard-admission-essay-change/
- Association of American Medical Colleges. Frequently asked questions: what does the Harvard and UNC decision mean for medical education? August 24, 2023. Accessed May 17, 2024. https://www.aamc.org/media/68771/download?attachment%3Fattachment
- American Medical Association. Affirmative action ends: how Supreme Court ruling impacts medical schools & the health care workforce. July 7, 2023. Accessed May 17, 2024. https://www.ama-assn.org/medical-students/medical-school-life/affirmative-action-ends-how-supreme-court-ruling-impacts
- Association of American Medical Colleges. How can medical schools boost racial diversity in the wake of the recent Supreme Court ruling? July 27, 2023. Accessed May 17, 2024. https://www.aamc.org/news/how-can-medical-schools-boost-racial-diversity-wake-recent-supreme-court-ruling
- Association of American Medical Colleges. Diversity in medical school admissions. Updated March 18, 2024. Accessed May 17, 2024. https://www.aamc.org/about-us/mission-areas/medical-education/diversity-medical-school-admissions
- United States Department of Justice. Questions and answers regarding the Supreme Court’s decision in Students For Fair Admissions, Inc. v. Harvard College and University of North Carolina. August 14, 2023. Accessed May 29, 2024. https://www.justice.gov/d9/2023-08/post-sffa_resource_faq_final_508.pdf
- US Department of Justice. Title VII of the Civil Rights Act of 1964. Accessed May 17, 2024. https://www.justice.gov/crt/laws-we-enforce
- Zheng L. How to effectively—and legally—use racial data for DEI. Harvard Business Review. July 24, 2023. Accessed May 17, 2024. https://hbr.org/2023/07/how-to-effectively-and-legally-use-racial-data-for-dei
- Crites K, Johnson J, Scott N, et al. Increasing diversity in residency training programs. Cureus. 2022;14:E25962. doi:10.7759/cureus.25962
- Association of American Medical Colleges. Holistic principles in resident selection: an introduction. Accessed May 17, 2024. https://www.aamc.org/media/44586/download?attachment
- Association of American Medical Colleges. Exploring the relationship between program signaling & interview invitations across specialties 2024 ERAS® preliminary analysis. December 29, 2023. Accessed May 17, 2024. https://www.aamc.org/media/74811/download?attachment
- Association of American Medical Colleges. Preliminary program signaling data and their impact on residency selection. October 24, 2023. Accessed May 17, 2024. https://www.aamc.org/services/eras-institutions/program-signaling-data#:~:text=Preliminary%20Program%20Signaling%20Data%20and%20Their%20Impact%20on%20Residency%20Selection,-Oct.&text=Program%20signals%20are%20a%20mechanism,whom%20to%20invite%20for%20interview
- Students for Fair Admissions, Inc. v University of North Carolina, 567 F. Supp. 3d 580 (M.D.N.C. 2021).
- Students for Fair Admissions, Inc. v President and Fellows of Harvard College, 600 US ___ (2023).
- Grutter v Bollinger, 539 US 306 (2003).
- Saul S. 9 states have banned affirmative action. here’s what that looks like. The New York Times. October 31, 2022. https://www.nytimes.com/2022/10/31/us/politics/affirmative-action-ban-states.html
- Desilver D. Private, selective colleges are most likely to use race, ethnicity as a factor in admissions decisions. Pew Research Center. July 14, 2023. Accessed May 29, 2024. https://www.pewresearch.org/short-reads/2023/07/14/private-selective-colleges-are-most-likely-to-use-race-ethnicity-as-a-factor-in-admissions-decisions/
- US Department of Education. Justice and education departments release resources to advance diversity and opportunity in higher education. August 14, 2023. Accessed May 17, 2024. https://www.ed.gov/news/press-releases/advance-diversity-and-opportunity-higher-education-justice-and-education-departments-release-resources-advance-diversity-and-opportunity-higher-education
- Amponsah MN, Hamid RD. Harvard overhauls college application in wake of affirmative action decision. The Harvard Crimson. August 3, 2023. Accessed May 17, 2024. https://www.thecrimson.com/article/2023/8/3/harvard-admission-essay-change/
- Association of American Medical Colleges. Frequently asked questions: what does the Harvard and UNC decision mean for medical education? August 24, 2023. Accessed May 17, 2024. https://www.aamc.org/media/68771/download?attachment%3Fattachment
- American Medical Association. Affirmative action ends: how Supreme Court ruling impacts medical schools & the health care workforce. July 7, 2023. Accessed May 17, 2024. https://www.ama-assn.org/medical-students/medical-school-life/affirmative-action-ends-how-supreme-court-ruling-impacts
- Association of American Medical Colleges. How can medical schools boost racial diversity in the wake of the recent Supreme Court ruling? July 27, 2023. Accessed May 17, 2024. https://www.aamc.org/news/how-can-medical-schools-boost-racial-diversity-wake-recent-supreme-court-ruling
- Association of American Medical Colleges. Diversity in medical school admissions. Updated March 18, 2024. Accessed May 17, 2024. https://www.aamc.org/about-us/mission-areas/medical-education/diversity-medical-school-admissions
- United States Department of Justice. Questions and answers regarding the Supreme Court’s decision in Students For Fair Admissions, Inc. v. Harvard College and University of North Carolina. August 14, 2023. Accessed May 29, 2024. https://www.justice.gov/d9/2023-08/post-sffa_resource_faq_final_508.pdf
- US Department of Justice. Title VII of the Civil Rights Act of 1964. Accessed May 17, 2024. https://www.justice.gov/crt/laws-we-enforce
- Zheng L. How to effectively—and legally—use racial data for DEI. Harvard Business Review. July 24, 2023. Accessed May 17, 2024. https://hbr.org/2023/07/how-to-effectively-and-legally-use-racial-data-for-dei
- Crites K, Johnson J, Scott N, et al. Increasing diversity in residency training programs. Cureus. 2022;14:E25962. doi:10.7759/cureus.25962
- Association of American Medical Colleges. Holistic principles in resident selection: an introduction. Accessed May 17, 2024. https://www.aamc.org/media/44586/download?attachment
- Association of American Medical Colleges. Exploring the relationship between program signaling & interview invitations across specialties 2024 ERAS® preliminary analysis. December 29, 2023. Accessed May 17, 2024. https://www.aamc.org/media/74811/download?attachment
- Association of American Medical Colleges. Preliminary program signaling data and their impact on residency selection. October 24, 2023. Accessed May 17, 2024. https://www.aamc.org/services/eras-institutions/program-signaling-data#:~:text=Preliminary%20Program%20Signaling%20Data%20and%20Their%20Impact%20on%20Residency%20Selection,-Oct.&text=Program%20signals%20are%20a%20mechanism,whom%20to%20invite%20for%20interview
Practice Points
- The 2023 ruling by the Supreme Court of the United States on the use of race-based criteria in college admissions may have implications for the selection of individuals into the dermatology workforce.
- We highlight the impacts of these decisions at the college, medical school, and dermatology residency levels and provide context for future directions in the selection processes for practicing dermatologists.
Prospective MS Trial Proves Ocrelizumab Efficacy in Under-Represented Populations
NASHVILLE, Tennessee — , according to the results of a 1-year analysis of the CHIMES trial. The study is the first-ever prospective study of an MS disease-modifying therapy (DMT) exclusively performed in under-represented populations, and offers lessons to researchers aiming to design more inclusive clinical trials to bolster participation by under-represented populations.
“The goal was to better understand efficacy of therapy in under-represented populations because we typically have very low numbers of these patients in our clinical trials, although there are multiple studies over the past decades suggesting that there may be poorer outcomes in Black and Hispanic individuals, particularly in the United States, and that there also may be more aggressive disease,” said Mitzi Williams, MD, who presented the study in a poster session at the annual meeting of the Consortium of Multiple Sclerosis Centers.
The team recruited 113 Black participants and 69 Hispanic participants, and, in fact, over-recruited the target number by 25%, and did so 2 months before the launch of the study in July 2020, which just happened to be in the midst of a global pandemic.
After 48 weeks of ocrelizumab treatment, 46.0% of Black participants and 58.0% of Hispanic participants achieved no evidence of disease activity in three components (NEDA-3), while 94.7% and 95.7% were free from relapses, respectively, and 94.7% and 94.2% were free from disease worsening. Serious adverse events occurred in 6.2% and 4.3% of each group, respectively, and there were no new safety signals in either group.
“The good news is that the efficacy and safety was very similar to what we saw in other clinical trials. I don’t think we really expected it to be much different, because when we think about race, it’s a social construct, not a biologic construct. What we do hope to find out is more about some of the interplay of social determinants of health, and how getting on high efficacy treatment can improve and increase productivity and outcomes in the long term,” said Dr. Williams, who is medical director of Joi Life Wellness Group, Smyrna, Georgia.
The researchers succeeded by involving patient advocates and advocacy organizations at the very earliest stages of the trial design. “We were very intentional about looking at things like social determinants of health, childcare, transportation, and things like that to ease some of the burden of participating in the trial, obviously in a legal and compliant way,” said Dr. Williams. The team also ensured complete and accurate translation of patient materials into Spanish.
The study was also a phase 4 trial, which may have simplified recruitment. “So it’s a therapy that’s already approved, which may make people feel more comfortable, but obviously the goal is for our phase 3 trials to make sure that we are recruiting represented populations. We’re taking these learnings and applying them to the broader clinical trial population so that hopefully we won’t have to come back and do phase 4 studies like this,” said Dr. Williams.
She noted that the results of more inclusive studies don’t just benefit underserved populations. “You have groups of people that are suffering and having more disability from a condition, and you need to understand why. When we broaden the population to understand those that are most vulnerable and underserved and [having the worst outcomes], it really helps us to better treat everybody. Because if we can get a hold of those factors that make us do the worst, then we can also better understand the factors that make us do the best,” said Dr. Williams.
Inclusive Recruitment in Clinical Trials
Asked for comment, Ahmed Obeidat, MD, PhD, highlighted the importance of inclusive recruitment. “The study is very important because historically and even in most recent clinical trials, these groups were markedly under-represented and most completed clinical trials derive conclusions based on the study of a nondiverse, White-non-Hispanic predominant population,” said Dr. Obeidat, who is an associate professor at the Medical College of Wisconsin, Milwaukee. He pointed to a systematic review showing that the median percentage of White participants in MS clinical trials was 93% and ranged from 86% to 98%.
“Several factors may contribute to the disparity in clinical trial participation, and solutions must be explored and developed. CHIMES is a first step in this direction where the study itself is designed to address disparity in MS clinical trial participation,” said Dr. Obeidat.
Dr. Obeidat also pointed to the need to consider other forms of diversity in clinical trials, such as older patients and those with advanced disability. “Investigators, coordinators, and other staff should all strive to be as inclusive as possible in clinical trials,” he said.
Dr. Williams has received consulting fees from Alexion, Biogen, Bristol Myers Squibb, EMD Serono, Genentech Inc., Janssen, Novartis, Sanofi, and TG Therapeutics, and serves on speakers bureaus for Biogen, Bristol Myers Squibb, EMD Serono, Janssen, Genentech, and TG Therapeutics. Dr. Ahmed Z. Obeidat has financial relationships with Alexion Pharmaceuticals, Banner Life Sciences, BD Biosciences, Biogen, Biologix Solutions, Bristol Myers Squibb, Celgene, EMD Serono, Genentech, GW Pharmaceuticals, Horizon Therapeutics, Jazz Pharmaceuticals, Novartis, Sandoz, Sanofi Genzyme, TG Therapeutics, and Viela Bio.
NASHVILLE, Tennessee — , according to the results of a 1-year analysis of the CHIMES trial. The study is the first-ever prospective study of an MS disease-modifying therapy (DMT) exclusively performed in under-represented populations, and offers lessons to researchers aiming to design more inclusive clinical trials to bolster participation by under-represented populations.
“The goal was to better understand efficacy of therapy in under-represented populations because we typically have very low numbers of these patients in our clinical trials, although there are multiple studies over the past decades suggesting that there may be poorer outcomes in Black and Hispanic individuals, particularly in the United States, and that there also may be more aggressive disease,” said Mitzi Williams, MD, who presented the study in a poster session at the annual meeting of the Consortium of Multiple Sclerosis Centers.
The team recruited 113 Black participants and 69 Hispanic participants, and, in fact, over-recruited the target number by 25%, and did so 2 months before the launch of the study in July 2020, which just happened to be in the midst of a global pandemic.
After 48 weeks of ocrelizumab treatment, 46.0% of Black participants and 58.0% of Hispanic participants achieved no evidence of disease activity in three components (NEDA-3), while 94.7% and 95.7% were free from relapses, respectively, and 94.7% and 94.2% were free from disease worsening. Serious adverse events occurred in 6.2% and 4.3% of each group, respectively, and there were no new safety signals in either group.
“The good news is that the efficacy and safety was very similar to what we saw in other clinical trials. I don’t think we really expected it to be much different, because when we think about race, it’s a social construct, not a biologic construct. What we do hope to find out is more about some of the interplay of social determinants of health, and how getting on high efficacy treatment can improve and increase productivity and outcomes in the long term,” said Dr. Williams, who is medical director of Joi Life Wellness Group, Smyrna, Georgia.
The researchers succeeded by involving patient advocates and advocacy organizations at the very earliest stages of the trial design. “We were very intentional about looking at things like social determinants of health, childcare, transportation, and things like that to ease some of the burden of participating in the trial, obviously in a legal and compliant way,” said Dr. Williams. The team also ensured complete and accurate translation of patient materials into Spanish.
The study was also a phase 4 trial, which may have simplified recruitment. “So it’s a therapy that’s already approved, which may make people feel more comfortable, but obviously the goal is for our phase 3 trials to make sure that we are recruiting represented populations. We’re taking these learnings and applying them to the broader clinical trial population so that hopefully we won’t have to come back and do phase 4 studies like this,” said Dr. Williams.
She noted that the results of more inclusive studies don’t just benefit underserved populations. “You have groups of people that are suffering and having more disability from a condition, and you need to understand why. When we broaden the population to understand those that are most vulnerable and underserved and [having the worst outcomes], it really helps us to better treat everybody. Because if we can get a hold of those factors that make us do the worst, then we can also better understand the factors that make us do the best,” said Dr. Williams.
Inclusive Recruitment in Clinical Trials
Asked for comment, Ahmed Obeidat, MD, PhD, highlighted the importance of inclusive recruitment. “The study is very important because historically and even in most recent clinical trials, these groups were markedly under-represented and most completed clinical trials derive conclusions based on the study of a nondiverse, White-non-Hispanic predominant population,” said Dr. Obeidat, who is an associate professor at the Medical College of Wisconsin, Milwaukee. He pointed to a systematic review showing that the median percentage of White participants in MS clinical trials was 93% and ranged from 86% to 98%.
“Several factors may contribute to the disparity in clinical trial participation, and solutions must be explored and developed. CHIMES is a first step in this direction where the study itself is designed to address disparity in MS clinical trial participation,” said Dr. Obeidat.
Dr. Obeidat also pointed to the need to consider other forms of diversity in clinical trials, such as older patients and those with advanced disability. “Investigators, coordinators, and other staff should all strive to be as inclusive as possible in clinical trials,” he said.
Dr. Williams has received consulting fees from Alexion, Biogen, Bristol Myers Squibb, EMD Serono, Genentech Inc., Janssen, Novartis, Sanofi, and TG Therapeutics, and serves on speakers bureaus for Biogen, Bristol Myers Squibb, EMD Serono, Janssen, Genentech, and TG Therapeutics. Dr. Ahmed Z. Obeidat has financial relationships with Alexion Pharmaceuticals, Banner Life Sciences, BD Biosciences, Biogen, Biologix Solutions, Bristol Myers Squibb, Celgene, EMD Serono, Genentech, GW Pharmaceuticals, Horizon Therapeutics, Jazz Pharmaceuticals, Novartis, Sandoz, Sanofi Genzyme, TG Therapeutics, and Viela Bio.
NASHVILLE, Tennessee — , according to the results of a 1-year analysis of the CHIMES trial. The study is the first-ever prospective study of an MS disease-modifying therapy (DMT) exclusively performed in under-represented populations, and offers lessons to researchers aiming to design more inclusive clinical trials to bolster participation by under-represented populations.
“The goal was to better understand efficacy of therapy in under-represented populations because we typically have very low numbers of these patients in our clinical trials, although there are multiple studies over the past decades suggesting that there may be poorer outcomes in Black and Hispanic individuals, particularly in the United States, and that there also may be more aggressive disease,” said Mitzi Williams, MD, who presented the study in a poster session at the annual meeting of the Consortium of Multiple Sclerosis Centers.
The team recruited 113 Black participants and 69 Hispanic participants, and, in fact, over-recruited the target number by 25%, and did so 2 months before the launch of the study in July 2020, which just happened to be in the midst of a global pandemic.
After 48 weeks of ocrelizumab treatment, 46.0% of Black participants and 58.0% of Hispanic participants achieved no evidence of disease activity in three components (NEDA-3), while 94.7% and 95.7% were free from relapses, respectively, and 94.7% and 94.2% were free from disease worsening. Serious adverse events occurred in 6.2% and 4.3% of each group, respectively, and there were no new safety signals in either group.
“The good news is that the efficacy and safety was very similar to what we saw in other clinical trials. I don’t think we really expected it to be much different, because when we think about race, it’s a social construct, not a biologic construct. What we do hope to find out is more about some of the interplay of social determinants of health, and how getting on high efficacy treatment can improve and increase productivity and outcomes in the long term,” said Dr. Williams, who is medical director of Joi Life Wellness Group, Smyrna, Georgia.
The researchers succeeded by involving patient advocates and advocacy organizations at the very earliest stages of the trial design. “We were very intentional about looking at things like social determinants of health, childcare, transportation, and things like that to ease some of the burden of participating in the trial, obviously in a legal and compliant way,” said Dr. Williams. The team also ensured complete and accurate translation of patient materials into Spanish.
The study was also a phase 4 trial, which may have simplified recruitment. “So it’s a therapy that’s already approved, which may make people feel more comfortable, but obviously the goal is for our phase 3 trials to make sure that we are recruiting represented populations. We’re taking these learnings and applying them to the broader clinical trial population so that hopefully we won’t have to come back and do phase 4 studies like this,” said Dr. Williams.
She noted that the results of more inclusive studies don’t just benefit underserved populations. “You have groups of people that are suffering and having more disability from a condition, and you need to understand why. When we broaden the population to understand those that are most vulnerable and underserved and [having the worst outcomes], it really helps us to better treat everybody. Because if we can get a hold of those factors that make us do the worst, then we can also better understand the factors that make us do the best,” said Dr. Williams.
Inclusive Recruitment in Clinical Trials
Asked for comment, Ahmed Obeidat, MD, PhD, highlighted the importance of inclusive recruitment. “The study is very important because historically and even in most recent clinical trials, these groups were markedly under-represented and most completed clinical trials derive conclusions based on the study of a nondiverse, White-non-Hispanic predominant population,” said Dr. Obeidat, who is an associate professor at the Medical College of Wisconsin, Milwaukee. He pointed to a systematic review showing that the median percentage of White participants in MS clinical trials was 93% and ranged from 86% to 98%.
“Several factors may contribute to the disparity in clinical trial participation, and solutions must be explored and developed. CHIMES is a first step in this direction where the study itself is designed to address disparity in MS clinical trial participation,” said Dr. Obeidat.
Dr. Obeidat also pointed to the need to consider other forms of diversity in clinical trials, such as older patients and those with advanced disability. “Investigators, coordinators, and other staff should all strive to be as inclusive as possible in clinical trials,” he said.
Dr. Williams has received consulting fees from Alexion, Biogen, Bristol Myers Squibb, EMD Serono, Genentech Inc., Janssen, Novartis, Sanofi, and TG Therapeutics, and serves on speakers bureaus for Biogen, Bristol Myers Squibb, EMD Serono, Janssen, Genentech, and TG Therapeutics. Dr. Ahmed Z. Obeidat has financial relationships with Alexion Pharmaceuticals, Banner Life Sciences, BD Biosciences, Biogen, Biologix Solutions, Bristol Myers Squibb, Celgene, EMD Serono, Genentech, GW Pharmaceuticals, Horizon Therapeutics, Jazz Pharmaceuticals, Novartis, Sandoz, Sanofi Genzyme, TG Therapeutics, and Viela Bio.
FROM CMSC 2024
Could British Columbia Eliminate Cervical Cancer by 2031?
To achieve this goal, the province will also need to reach historically underscreened, equity-seeking populations (ie, Black, indigenous, immigrant, LGBTQ, and disabled patients, and those with sexual trauma) through mailed self-screening HPV tests.
The adoption of both these strategies is essential, according to a modeling study that was published on June 3 in CMAJ, especially because the true impact of HPV vaccination has yet to be fully realized.
“In BC, we have a school-based program to increase vaccine coverage in boys and girls starting in grade 6,” study author Reka Pataky, PhD, a senior research health economist at the Canadian Centre for Applied Research in Cancer Control and BC Cancer in Vancouver, British Columbia, Canada, told this news organization. Dr. Pataky noted that this immunization program was launched in 2008 and that some of the initial cohorts haven›t yet reached the average age of diagnosis, which is between 30 and 59 years.
Three’s a Charm
The investigators undertook a modeling study to determine when and how BC might achieve the elimination of cervical cancer following a transition to HPV-based screening. Elimination was defined as an annual age-standardized incidence rate of < 4.0 per 100,000 women.
Modeling scenarios were developed using the Canadian Partnership Against Cancer’s priority targets, which include increasing HPV vaccination through school-based coverage from 70% to 90%, increasing the probability of ever receiving a screening test from 90% to 95%, increasing the rate of on-time screening from 70% to 90%, and improving follow-up to 95% for colposcopy (currently 88%) and HPV testing (currently 80%). Modeling simulated HPV transmission and the natural history of cervical cancer in the Canadian population and relied upon two reference scenarios: One using BC’s cytology-based screening at the time of analysis, and the other an HPV base-case scenario.
The researchers found that with the status quo (ie, cytology-based screening and no change to vaccination or screening participation rates), BC would not eliminate cervical cancer until 2045. Implementation of HPV-based screening at the current 70% participation rate would achieve elimination in 2034 and prevent 942 cases compared with cytology screening. Increasing the proportion of patients who were ever screened or increasing vaccination coverage would result in cervical cancer elimination by 2033. The time line would be shortened even further (to 2031) through a combination of three strategies (ie, improving recruitment, on-time screening, and follow-up compliance).
Low Incidence, Strained System
The incidence of cervical cancer in Canada is relatively low, accounting for 1.3% of all new female cancers and 1.1% of all female cancer deaths.
“The reason that we have such low rates is because we have organized screening programs,” explained Rachel Kupets, MD, associate professor of gynecologic oncology at the University of Toronto and Sunnybrook Hospital, Toronto. She was not involved in the study.
“We’re starting to see what happens when the system gets strained with lower participation rates. I am starting to see a lot more women with invasive cervical cancer. They’re younger, and their cancers are less curable and less treatable,” she said.
Difficulties with access, interest, and education have contributed to low cervical screening rates among equity-seeking populations, according to Dr. Pataky and Dr. Kupets.
“Self-screening is another tool that can incrementally benefit those folks who wouldn’t otherwise undergo screening or don’t want an invasive test,” said Dr. Kupets. It can also play an increasing role, while current access to primary care services in Canada is at an all-time low. Community outreach through centers, mobile coaches, and nursing stations might help ensure participation by at-risk populations. These measures also could boost follow-up for and education about positive results, said Dr. Kupets.
In a related editorial, Shannon Charlebois, MD, medical editor of CMAJ, and Sarah Kean, MD, assistant professor of gynecologic oncology at the University of Manitoba in Winnipeg, Manitoba, Canada, emphasized the need for mailed HPV self-screening kits to be paid for and integrated into provincial cervical cancer screening programs across Canada to support earlier cervical cancer detection and lower invasive cancer rates.
Dr. Pataky concurred. “There have been discussions about making the big transition from traditional cytology to implementing HPV self-screening,” she said. “We have really effective tools for preventing cervical cancer, and it’s important to not lose sight of that goal.”
The study was funded by the National Institutes of Health. Dr. Pataky and Dr. Kupets reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
To achieve this goal, the province will also need to reach historically underscreened, equity-seeking populations (ie, Black, indigenous, immigrant, LGBTQ, and disabled patients, and those with sexual trauma) through mailed self-screening HPV tests.
The adoption of both these strategies is essential, according to a modeling study that was published on June 3 in CMAJ, especially because the true impact of HPV vaccination has yet to be fully realized.
“In BC, we have a school-based program to increase vaccine coverage in boys and girls starting in grade 6,” study author Reka Pataky, PhD, a senior research health economist at the Canadian Centre for Applied Research in Cancer Control and BC Cancer in Vancouver, British Columbia, Canada, told this news organization. Dr. Pataky noted that this immunization program was launched in 2008 and that some of the initial cohorts haven›t yet reached the average age of diagnosis, which is between 30 and 59 years.
Three’s a Charm
The investigators undertook a modeling study to determine when and how BC might achieve the elimination of cervical cancer following a transition to HPV-based screening. Elimination was defined as an annual age-standardized incidence rate of < 4.0 per 100,000 women.
Modeling scenarios were developed using the Canadian Partnership Against Cancer’s priority targets, which include increasing HPV vaccination through school-based coverage from 70% to 90%, increasing the probability of ever receiving a screening test from 90% to 95%, increasing the rate of on-time screening from 70% to 90%, and improving follow-up to 95% for colposcopy (currently 88%) and HPV testing (currently 80%). Modeling simulated HPV transmission and the natural history of cervical cancer in the Canadian population and relied upon two reference scenarios: One using BC’s cytology-based screening at the time of analysis, and the other an HPV base-case scenario.
The researchers found that with the status quo (ie, cytology-based screening and no change to vaccination or screening participation rates), BC would not eliminate cervical cancer until 2045. Implementation of HPV-based screening at the current 70% participation rate would achieve elimination in 2034 and prevent 942 cases compared with cytology screening. Increasing the proportion of patients who were ever screened or increasing vaccination coverage would result in cervical cancer elimination by 2033. The time line would be shortened even further (to 2031) through a combination of three strategies (ie, improving recruitment, on-time screening, and follow-up compliance).
Low Incidence, Strained System
The incidence of cervical cancer in Canada is relatively low, accounting for 1.3% of all new female cancers and 1.1% of all female cancer deaths.
“The reason that we have such low rates is because we have organized screening programs,” explained Rachel Kupets, MD, associate professor of gynecologic oncology at the University of Toronto and Sunnybrook Hospital, Toronto. She was not involved in the study.
“We’re starting to see what happens when the system gets strained with lower participation rates. I am starting to see a lot more women with invasive cervical cancer. They’re younger, and their cancers are less curable and less treatable,” she said.
Difficulties with access, interest, and education have contributed to low cervical screening rates among equity-seeking populations, according to Dr. Pataky and Dr. Kupets.
“Self-screening is another tool that can incrementally benefit those folks who wouldn’t otherwise undergo screening or don’t want an invasive test,” said Dr. Kupets. It can also play an increasing role, while current access to primary care services in Canada is at an all-time low. Community outreach through centers, mobile coaches, and nursing stations might help ensure participation by at-risk populations. These measures also could boost follow-up for and education about positive results, said Dr. Kupets.
In a related editorial, Shannon Charlebois, MD, medical editor of CMAJ, and Sarah Kean, MD, assistant professor of gynecologic oncology at the University of Manitoba in Winnipeg, Manitoba, Canada, emphasized the need for mailed HPV self-screening kits to be paid for and integrated into provincial cervical cancer screening programs across Canada to support earlier cervical cancer detection and lower invasive cancer rates.
Dr. Pataky concurred. “There have been discussions about making the big transition from traditional cytology to implementing HPV self-screening,” she said. “We have really effective tools for preventing cervical cancer, and it’s important to not lose sight of that goal.”
The study was funded by the National Institutes of Health. Dr. Pataky and Dr. Kupets reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
To achieve this goal, the province will also need to reach historically underscreened, equity-seeking populations (ie, Black, indigenous, immigrant, LGBTQ, and disabled patients, and those with sexual trauma) through mailed self-screening HPV tests.
The adoption of both these strategies is essential, according to a modeling study that was published on June 3 in CMAJ, especially because the true impact of HPV vaccination has yet to be fully realized.
“In BC, we have a school-based program to increase vaccine coverage in boys and girls starting in grade 6,” study author Reka Pataky, PhD, a senior research health economist at the Canadian Centre for Applied Research in Cancer Control and BC Cancer in Vancouver, British Columbia, Canada, told this news organization. Dr. Pataky noted that this immunization program was launched in 2008 and that some of the initial cohorts haven›t yet reached the average age of diagnosis, which is between 30 and 59 years.
Three’s a Charm
The investigators undertook a modeling study to determine when and how BC might achieve the elimination of cervical cancer following a transition to HPV-based screening. Elimination was defined as an annual age-standardized incidence rate of < 4.0 per 100,000 women.
Modeling scenarios were developed using the Canadian Partnership Against Cancer’s priority targets, which include increasing HPV vaccination through school-based coverage from 70% to 90%, increasing the probability of ever receiving a screening test from 90% to 95%, increasing the rate of on-time screening from 70% to 90%, and improving follow-up to 95% for colposcopy (currently 88%) and HPV testing (currently 80%). Modeling simulated HPV transmission and the natural history of cervical cancer in the Canadian population and relied upon two reference scenarios: One using BC’s cytology-based screening at the time of analysis, and the other an HPV base-case scenario.
The researchers found that with the status quo (ie, cytology-based screening and no change to vaccination or screening participation rates), BC would not eliminate cervical cancer until 2045. Implementation of HPV-based screening at the current 70% participation rate would achieve elimination in 2034 and prevent 942 cases compared with cytology screening. Increasing the proportion of patients who were ever screened or increasing vaccination coverage would result in cervical cancer elimination by 2033. The time line would be shortened even further (to 2031) through a combination of three strategies (ie, improving recruitment, on-time screening, and follow-up compliance).
Low Incidence, Strained System
The incidence of cervical cancer in Canada is relatively low, accounting for 1.3% of all new female cancers and 1.1% of all female cancer deaths.
“The reason that we have such low rates is because we have organized screening programs,” explained Rachel Kupets, MD, associate professor of gynecologic oncology at the University of Toronto and Sunnybrook Hospital, Toronto. She was not involved in the study.
“We’re starting to see what happens when the system gets strained with lower participation rates. I am starting to see a lot more women with invasive cervical cancer. They’re younger, and their cancers are less curable and less treatable,” she said.
Difficulties with access, interest, and education have contributed to low cervical screening rates among equity-seeking populations, according to Dr. Pataky and Dr. Kupets.
“Self-screening is another tool that can incrementally benefit those folks who wouldn’t otherwise undergo screening or don’t want an invasive test,” said Dr. Kupets. It can also play an increasing role, while current access to primary care services in Canada is at an all-time low. Community outreach through centers, mobile coaches, and nursing stations might help ensure participation by at-risk populations. These measures also could boost follow-up for and education about positive results, said Dr. Kupets.
In a related editorial, Shannon Charlebois, MD, medical editor of CMAJ, and Sarah Kean, MD, assistant professor of gynecologic oncology at the University of Manitoba in Winnipeg, Manitoba, Canada, emphasized the need for mailed HPV self-screening kits to be paid for and integrated into provincial cervical cancer screening programs across Canada to support earlier cervical cancer detection and lower invasive cancer rates.
Dr. Pataky concurred. “There have been discussions about making the big transition from traditional cytology to implementing HPV self-screening,” she said. “We have really effective tools for preventing cervical cancer, and it’s important to not lose sight of that goal.”
The study was funded by the National Institutes of Health. Dr. Pataky and Dr. Kupets reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
Features of Merkel Cell in Hispanic Patients Explored
. In addition, the most affected site was the upper limb/shoulder, which differs from what has been reported in previous studies.
Those are key findings from a retrospective study of national cancer data that was presented during a poster session at the annual meeting of the Society for Investigative Dermatology.
“Merkel cell carcinoma is an infrequent and aggressive form of neuroendocrine skin cancer that mainly impacts individuals of White ethnicity, with a general occurrence rate of 0.7 instances per 100,000 person-years,” one of the study authors, Luis J. Borda, MD, chief dermatology resident at Eastern Virginia Medical School, Norfolk, Virginia, told this news organization. The incidence of MCC is increasing among all racial groups, especially in the Hispanic population, he added.
To determine how age, sex, and primary site of MCC differ in White vs non-White Hispanic patients, the researchers evaluated the 22 population-based cancer registries of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program from 2000 through 2020. They reported categorical variables as counts and percentages and used chi-square test with Yates’s correction to assess the association between categorical variables.
Of the 17,920 MCCs identified by the researchers, 40 (0.22%) were in non-White Hispanic patients. Compared with the White patients with MCC, significantly fewer non-White Hispanic patients were age 70 years or older (50% vs 72.1%, respectively; P < .001), and MCC was more common in female non-White Hispanic patients (23, or 57.5%), while White patients with MCC were predominantly male (11,309, or 63.2%; P < .05). “This suggests that MCC in non-White Hispanic patients may involve different risk factors related to age beyond just cumulative UV exposure and aging-related immunosenescence, which may additionally account for the higher prevalence of females in this cohort, as historically male outdoor occupation has resulted in increased lifetime cumulative UV exposure,” Dr. Borda said.
The head and neck were the most common sites of disease involvement in White patients (41.9% vs 27.5% in non-White Hispanic patients; P = .09), while the upper limb and shoulder were the most common sites of disease involvement in non-White Hispanic patients (37.5% vs 23.8% in White patients; P = .06). This finding “differs from previous studies showing head/neck being the most common site in Hispanics,” Dr. Borda said, adding that this could be a result of White patients not being included in the Hispanic cohort in this study. “Because non-White Hispanic patients have darker skin, they may have proportionally more cases on sun-protected skin, as is described by the present data, suggesting that they are less likely to have UV-driven MCC.”
The study “highlights distinct demographic and clinical characteristics of MCC among non-White Hispanic patients compared to their White counterparts, emphasizing the importance of considering race/ethnicity in understanding the epidemiology of this rare but increasingly prevalent cancer,” Dr. Borda said. He and his co-authors are planning to do further research on the increasing incidence of MCC in non-White Hispanic patients and on staging at diagnosis compared to White patients.
Dr. Borda acknowledged certain limitations of the analysis, including the small sample size in the non-White Hispanic group, the retrospective nature of SEER data, selection bias, and the potential for underreporting. He and his co-authors reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
. In addition, the most affected site was the upper limb/shoulder, which differs from what has been reported in previous studies.
Those are key findings from a retrospective study of national cancer data that was presented during a poster session at the annual meeting of the Society for Investigative Dermatology.
“Merkel cell carcinoma is an infrequent and aggressive form of neuroendocrine skin cancer that mainly impacts individuals of White ethnicity, with a general occurrence rate of 0.7 instances per 100,000 person-years,” one of the study authors, Luis J. Borda, MD, chief dermatology resident at Eastern Virginia Medical School, Norfolk, Virginia, told this news organization. The incidence of MCC is increasing among all racial groups, especially in the Hispanic population, he added.
To determine how age, sex, and primary site of MCC differ in White vs non-White Hispanic patients, the researchers evaluated the 22 population-based cancer registries of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program from 2000 through 2020. They reported categorical variables as counts and percentages and used chi-square test with Yates’s correction to assess the association between categorical variables.
Of the 17,920 MCCs identified by the researchers, 40 (0.22%) were in non-White Hispanic patients. Compared with the White patients with MCC, significantly fewer non-White Hispanic patients were age 70 years or older (50% vs 72.1%, respectively; P < .001), and MCC was more common in female non-White Hispanic patients (23, or 57.5%), while White patients with MCC were predominantly male (11,309, or 63.2%; P < .05). “This suggests that MCC in non-White Hispanic patients may involve different risk factors related to age beyond just cumulative UV exposure and aging-related immunosenescence, which may additionally account for the higher prevalence of females in this cohort, as historically male outdoor occupation has resulted in increased lifetime cumulative UV exposure,” Dr. Borda said.
The head and neck were the most common sites of disease involvement in White patients (41.9% vs 27.5% in non-White Hispanic patients; P = .09), while the upper limb and shoulder were the most common sites of disease involvement in non-White Hispanic patients (37.5% vs 23.8% in White patients; P = .06). This finding “differs from previous studies showing head/neck being the most common site in Hispanics,” Dr. Borda said, adding that this could be a result of White patients not being included in the Hispanic cohort in this study. “Because non-White Hispanic patients have darker skin, they may have proportionally more cases on sun-protected skin, as is described by the present data, suggesting that they are less likely to have UV-driven MCC.”
The study “highlights distinct demographic and clinical characteristics of MCC among non-White Hispanic patients compared to their White counterparts, emphasizing the importance of considering race/ethnicity in understanding the epidemiology of this rare but increasingly prevalent cancer,” Dr. Borda said. He and his co-authors are planning to do further research on the increasing incidence of MCC in non-White Hispanic patients and on staging at diagnosis compared to White patients.
Dr. Borda acknowledged certain limitations of the analysis, including the small sample size in the non-White Hispanic group, the retrospective nature of SEER data, selection bias, and the potential for underreporting. He and his co-authors reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
. In addition, the most affected site was the upper limb/shoulder, which differs from what has been reported in previous studies.
Those are key findings from a retrospective study of national cancer data that was presented during a poster session at the annual meeting of the Society for Investigative Dermatology.
“Merkel cell carcinoma is an infrequent and aggressive form of neuroendocrine skin cancer that mainly impacts individuals of White ethnicity, with a general occurrence rate of 0.7 instances per 100,000 person-years,” one of the study authors, Luis J. Borda, MD, chief dermatology resident at Eastern Virginia Medical School, Norfolk, Virginia, told this news organization. The incidence of MCC is increasing among all racial groups, especially in the Hispanic population, he added.
To determine how age, sex, and primary site of MCC differ in White vs non-White Hispanic patients, the researchers evaluated the 22 population-based cancer registries of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program from 2000 through 2020. They reported categorical variables as counts and percentages and used chi-square test with Yates’s correction to assess the association between categorical variables.
Of the 17,920 MCCs identified by the researchers, 40 (0.22%) were in non-White Hispanic patients. Compared with the White patients with MCC, significantly fewer non-White Hispanic patients were age 70 years or older (50% vs 72.1%, respectively; P < .001), and MCC was more common in female non-White Hispanic patients (23, or 57.5%), while White patients with MCC were predominantly male (11,309, or 63.2%; P < .05). “This suggests that MCC in non-White Hispanic patients may involve different risk factors related to age beyond just cumulative UV exposure and aging-related immunosenescence, which may additionally account for the higher prevalence of females in this cohort, as historically male outdoor occupation has resulted in increased lifetime cumulative UV exposure,” Dr. Borda said.
The head and neck were the most common sites of disease involvement in White patients (41.9% vs 27.5% in non-White Hispanic patients; P = .09), while the upper limb and shoulder were the most common sites of disease involvement in non-White Hispanic patients (37.5% vs 23.8% in White patients; P = .06). This finding “differs from previous studies showing head/neck being the most common site in Hispanics,” Dr. Borda said, adding that this could be a result of White patients not being included in the Hispanic cohort in this study. “Because non-White Hispanic patients have darker skin, they may have proportionally more cases on sun-protected skin, as is described by the present data, suggesting that they are less likely to have UV-driven MCC.”
The study “highlights distinct demographic and clinical characteristics of MCC among non-White Hispanic patients compared to their White counterparts, emphasizing the importance of considering race/ethnicity in understanding the epidemiology of this rare but increasingly prevalent cancer,” Dr. Borda said. He and his co-authors are planning to do further research on the increasing incidence of MCC in non-White Hispanic patients and on staging at diagnosis compared to White patients.
Dr. Borda acknowledged certain limitations of the analysis, including the small sample size in the non-White Hispanic group, the retrospective nature of SEER data, selection bias, and the potential for underreporting. He and his co-authors reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
FROM SID 2024
Need a Wood Lamp Alternative? Grab Your Smartphone
Practice Gap
The Wood lamp commonly is used as a diagnostic tool for pigmentary skin conditions (eg, vitiligo) or skin conditions that exhibit fluorescence (eg, erythrasma).1 Recently, its diagnostic efficacy has extended to scabies, in which it unveils a distinctive wavy, bluish-white, linear fluorescence upon illumination.2
Functionally, the Wood lamp operates by subjecting phosphors to UV light within the wavelength range of 320 to 400 nm, inducing fluorescence in substances such as collagen and elastin. In the context of vitiligo, this process manifests as a preferential chalk white fluorescence in areas lacking melanin.1
Despite its demonstrated effectiveness, the Wood lamp is not without limitations. It comes with a notable financial investment ranging from $70 to $500, requires periodic maintenance such as light bulb replacements, and can be unwieldy.3 Furthermore, its reliance on a power source poses a challenge in settings where immediate access to convenient power outlets is limited, such as inpatient and rural dermatology clinics. These limitations underscore the need for alternative solutions and innovations to address challenges and ensure accessibility in diverse health care environments.
The Tools
Free smartphone applications (apps), such as Ultraviolet Light-UV Lamp by AppBrain or Blacklight UV Light Simulator by That Smile, can simulate UV light and functionally serve as a Wood lamp.
The Technique
UV light apps use LED or organic LED screen pixels to emit a blue light equivalent at 467 nm.4 Although these apps are not designed specifically for dermatologic uses, they are mostly free, widely available for Android and iPhone users, and portable. Importantly, they can demonstrate good performance in visualizing vitiligo, as shown in Figure 1—albeit perhaps not reaching the same level as the Wood lamp (Figure 2).
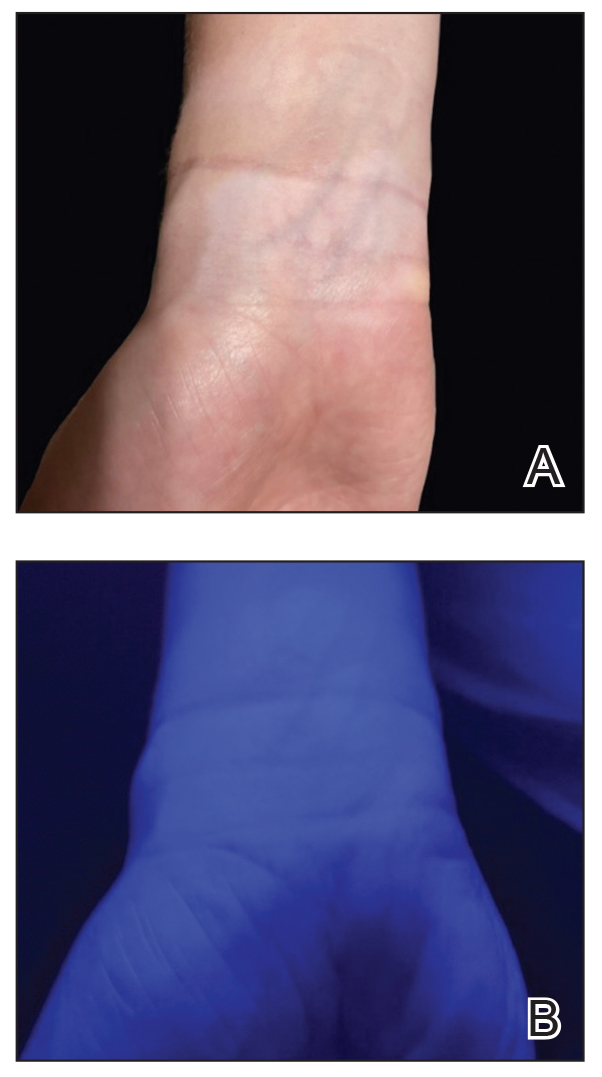
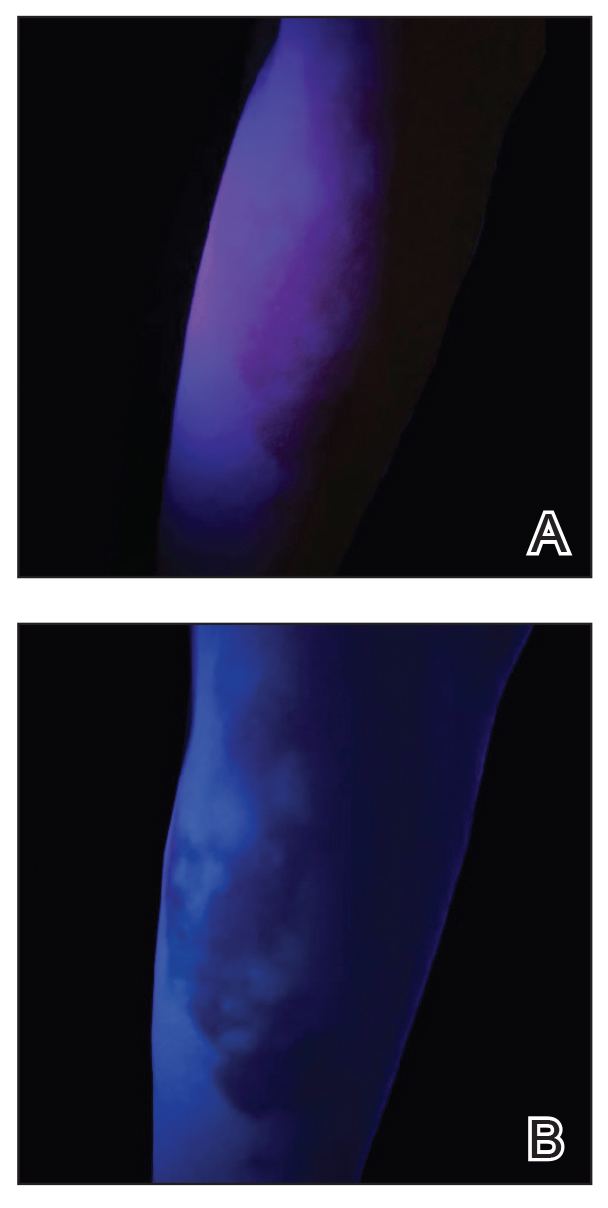
Because these UV light apps are not regulated and their efficacy for medical use has not been firmly established, the Wood lamp remains the gold standard. Therefore, we propose the use of UV light apps in situations when a Wood lamp is not available or convenient, such as in rural, inpatient, or international health care settings.
Practice Implications
Exploring and adopting these free alternatives can contribute to improved accessibility and diagnostic capabilities in diverse health care environments, particularly for communities facing financial constraints. Continued research and validation of these apps in clinical settings will be essential to establish their reliability and effectiveness in enhancing diagnostic practices.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Scanni G. Facilitations in the clinical diagnosis of human scabies through the use of ultraviolet light (UV-scab scanning): a case-series study. Trop Med Infect Dis. 2022;7:422. doi:10.3390/tropicalmed7120422
- USA Medical and Surgical Supplies. Top 9 medical diagnostic applications for a Woods lamp. February 26, 2019. Accessed May 20, 2024.
- Huang Y, Hsiang E-L, Deng M-Y, et al. Mini-led, micro-led and OLED displays: present status and future perspectives. Light Sci Appl. 2020;9:105. doi:10.1038/s41377-020-0341-9
Practice Gap
The Wood lamp commonly is used as a diagnostic tool for pigmentary skin conditions (eg, vitiligo) or skin conditions that exhibit fluorescence (eg, erythrasma).1 Recently, its diagnostic efficacy has extended to scabies, in which it unveils a distinctive wavy, bluish-white, linear fluorescence upon illumination.2
Functionally, the Wood lamp operates by subjecting phosphors to UV light within the wavelength range of 320 to 400 nm, inducing fluorescence in substances such as collagen and elastin. In the context of vitiligo, this process manifests as a preferential chalk white fluorescence in areas lacking melanin.1
Despite its demonstrated effectiveness, the Wood lamp is not without limitations. It comes with a notable financial investment ranging from $70 to $500, requires periodic maintenance such as light bulb replacements, and can be unwieldy.3 Furthermore, its reliance on a power source poses a challenge in settings where immediate access to convenient power outlets is limited, such as inpatient and rural dermatology clinics. These limitations underscore the need for alternative solutions and innovations to address challenges and ensure accessibility in diverse health care environments.
The Tools
Free smartphone applications (apps), such as Ultraviolet Light-UV Lamp by AppBrain or Blacklight UV Light Simulator by That Smile, can simulate UV light and functionally serve as a Wood lamp.
The Technique
UV light apps use LED or organic LED screen pixels to emit a blue light equivalent at 467 nm.4 Although these apps are not designed specifically for dermatologic uses, they are mostly free, widely available for Android and iPhone users, and portable. Importantly, they can demonstrate good performance in visualizing vitiligo, as shown in Figure 1—albeit perhaps not reaching the same level as the Wood lamp (Figure 2).
Because these UV light apps are not regulated and their efficacy for medical use has not been firmly established, the Wood lamp remains the gold standard. Therefore, we propose the use of UV light apps in situations when a Wood lamp is not available or convenient, such as in rural, inpatient, or international health care settings.
Practice Implications
Exploring and adopting these free alternatives can contribute to improved accessibility and diagnostic capabilities in diverse health care environments, particularly for communities facing financial constraints. Continued research and validation of these apps in clinical settings will be essential to establish their reliability and effectiveness in enhancing diagnostic practices.
Practice Gap
The Wood lamp commonly is used as a diagnostic tool for pigmentary skin conditions (eg, vitiligo) or skin conditions that exhibit fluorescence (eg, erythrasma).1 Recently, its diagnostic efficacy has extended to scabies, in which it unveils a distinctive wavy, bluish-white, linear fluorescence upon illumination.2
Functionally, the Wood lamp operates by subjecting phosphors to UV light within the wavelength range of 320 to 400 nm, inducing fluorescence in substances such as collagen and elastin. In the context of vitiligo, this process manifests as a preferential chalk white fluorescence in areas lacking melanin.1
Despite its demonstrated effectiveness, the Wood lamp is not without limitations. It comes with a notable financial investment ranging from $70 to $500, requires periodic maintenance such as light bulb replacements, and can be unwieldy.3 Furthermore, its reliance on a power source poses a challenge in settings where immediate access to convenient power outlets is limited, such as inpatient and rural dermatology clinics. These limitations underscore the need for alternative solutions and innovations to address challenges and ensure accessibility in diverse health care environments.
The Tools
Free smartphone applications (apps), such as Ultraviolet Light-UV Lamp by AppBrain or Blacklight UV Light Simulator by That Smile, can simulate UV light and functionally serve as a Wood lamp.
The Technique
UV light apps use LED or organic LED screen pixels to emit a blue light equivalent at 467 nm.4 Although these apps are not designed specifically for dermatologic uses, they are mostly free, widely available for Android and iPhone users, and portable. Importantly, they can demonstrate good performance in visualizing vitiligo, as shown in Figure 1—albeit perhaps not reaching the same level as the Wood lamp (Figure 2).
Because these UV light apps are not regulated and their efficacy for medical use has not been firmly established, the Wood lamp remains the gold standard. Therefore, we propose the use of UV light apps in situations when a Wood lamp is not available or convenient, such as in rural, inpatient, or international health care settings.
Practice Implications
Exploring and adopting these free alternatives can contribute to improved accessibility and diagnostic capabilities in diverse health care environments, particularly for communities facing financial constraints. Continued research and validation of these apps in clinical settings will be essential to establish their reliability and effectiveness in enhancing diagnostic practices.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Scanni G. Facilitations in the clinical diagnosis of human scabies through the use of ultraviolet light (UV-scab scanning): a case-series study. Trop Med Infect Dis. 2022;7:422. doi:10.3390/tropicalmed7120422
- USA Medical and Surgical Supplies. Top 9 medical diagnostic applications for a Woods lamp. February 26, 2019. Accessed May 20, 2024.
- Huang Y, Hsiang E-L, Deng M-Y, et al. Mini-led, micro-led and OLED displays: present status and future perspectives. Light Sci Appl. 2020;9:105. doi:10.1038/s41377-020-0341-9
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Scanni G. Facilitations in the clinical diagnosis of human scabies through the use of ultraviolet light (UV-scab scanning): a case-series study. Trop Med Infect Dis. 2022;7:422. doi:10.3390/tropicalmed7120422
- USA Medical and Surgical Supplies. Top 9 medical diagnostic applications for a Woods lamp. February 26, 2019. Accessed May 20, 2024.
- Huang Y, Hsiang E-L, Deng M-Y, et al. Mini-led, micro-led and OLED displays: present status and future perspectives. Light Sci Appl. 2020;9:105. doi:10.1038/s41377-020-0341-9
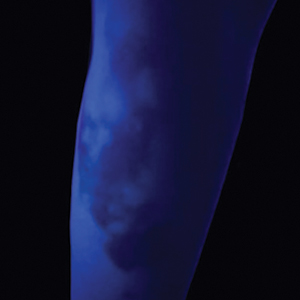
The Value of Early Education
Early education is right up there with motherhood and apple pie as unarguable positive concepts. How could exposing young children to a school-like atmosphere not be a benefit, particularly in communities dominated by socioeconomic challenges? While there are some questions about the value of playing Mozart to infants, early education in the traditional sense continues to be viewed as a key strategy for providing young children a preschool foundation on which a successful academic career can be built. Several oft-cited randomized controlled trials have fueled both private and public interest and funding.
However, a recent commentary published in Science suggests that all programs are “not unequivocally positive and much more research is needed.” “Worrisome results in Tennessee,” “Success in Boston,” and “Largely null results for Headstart” are just a few of the article’s section titles and convey a sense of the inconsistency the investigators found as they reviewed early education systems around the country.

While there may be some politicians who may attempt to use the results of this investigation as a reason to cancel public funding of underperforming early education programs, the authors avoid this baby-and-the-bathwater conclusion. Instead, they urge more rigorous research “to understand how effective programs can be designed and implemented.”
The kind of re-thinking and brainstorming these investigators suggest takes time. While we’re waiting for this process to gain traction, this might be a good time to consider some of the benefits of early education that we don’t usually consider when our focus is on academic metrics.
A recent paper in Children’s Health Care by investigators at the Boston University Medical Center and School of Medicine considered the diet of children attending preschool. Looking at the dietary records of more than 300 children attending 30 childcare centers, the researchers found that the children’s diets before arrival at daycare was less healthy than while they were in daycare. “The hour after pickup appeared to be the least healthful” of any of the time periods surveyed. Of course, we will all conjure up images of what this chaotic post-daycare pickup may look like and cut the harried parents and grandparents some slack when it comes to nutritional choices. However, the bottom line is that for the group of children surveyed being in preschool or daycare protected them from a less healthy diet they were being provided outside of school hours.
Our recent experience with pandemic-related school closures provides more evidence that being in school was superior to any remote experience academically. School-age children and adolescents gained weight when school closures were the norm. Play patterns for children shifted from outdoor play to indoor play — often dominated by more sedentary video games. Both fatal and non-fatal gun-related injuries surged during the pandemic and, by far, the majority of these occur in the home and not at school.
Stepping back to look at this broader picture that includes diet, physical activity, and safety — not to mention the benefits of socialization — leads one to arrive at the unfortunate conclusion that Of course there will be those who point to the belief that schools are petri dishes putting children at greater risk for respiratory infections. On the other hand, we must accept that schools haven’t proved to be a major factor in the spread of COVID that many had feared.
The authors of the study in Science are certainly correct in recommending a more thorough investigation into the academic benefits of preschool education. However, we must keep in mind that preschool offers an environment that can be a positive influence on young children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Early education is right up there with motherhood and apple pie as unarguable positive concepts. How could exposing young children to a school-like atmosphere not be a benefit, particularly in communities dominated by socioeconomic challenges? While there are some questions about the value of playing Mozart to infants, early education in the traditional sense continues to be viewed as a key strategy for providing young children a preschool foundation on which a successful academic career can be built. Several oft-cited randomized controlled trials have fueled both private and public interest and funding.
However, a recent commentary published in Science suggests that all programs are “not unequivocally positive and much more research is needed.” “Worrisome results in Tennessee,” “Success in Boston,” and “Largely null results for Headstart” are just a few of the article’s section titles and convey a sense of the inconsistency the investigators found as they reviewed early education systems around the country.
While there may be some politicians who may attempt to use the results of this investigation as a reason to cancel public funding of underperforming early education programs, the authors avoid this baby-and-the-bathwater conclusion. Instead, they urge more rigorous research “to understand how effective programs can be designed and implemented.”
The kind of re-thinking and brainstorming these investigators suggest takes time. While we’re waiting for this process to gain traction, this might be a good time to consider some of the benefits of early education that we don’t usually consider when our focus is on academic metrics.
A recent paper in Children’s Health Care by investigators at the Boston University Medical Center and School of Medicine considered the diet of children attending preschool. Looking at the dietary records of more than 300 children attending 30 childcare centers, the researchers found that the children’s diets before arrival at daycare was less healthy than while they were in daycare. “The hour after pickup appeared to be the least healthful” of any of the time periods surveyed. Of course, we will all conjure up images of what this chaotic post-daycare pickup may look like and cut the harried parents and grandparents some slack when it comes to nutritional choices. However, the bottom line is that for the group of children surveyed being in preschool or daycare protected them from a less healthy diet they were being provided outside of school hours.
Our recent experience with pandemic-related school closures provides more evidence that being in school was superior to any remote experience academically. School-age children and adolescents gained weight when school closures were the norm. Play patterns for children shifted from outdoor play to indoor play — often dominated by more sedentary video games. Both fatal and non-fatal gun-related injuries surged during the pandemic and, by far, the majority of these occur in the home and not at school.
Stepping back to look at this broader picture that includes diet, physical activity, and safety — not to mention the benefits of socialization — leads one to arrive at the unfortunate conclusion that Of course there will be those who point to the belief that schools are petri dishes putting children at greater risk for respiratory infections. On the other hand, we must accept that schools haven’t proved to be a major factor in the spread of COVID that many had feared.
The authors of the study in Science are certainly correct in recommending a more thorough investigation into the academic benefits of preschool education. However, we must keep in mind that preschool offers an environment that can be a positive influence on young children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Early education is right up there with motherhood and apple pie as unarguable positive concepts. How could exposing young children to a school-like atmosphere not be a benefit, particularly in communities dominated by socioeconomic challenges? While there are some questions about the value of playing Mozart to infants, early education in the traditional sense continues to be viewed as a key strategy for providing young children a preschool foundation on which a successful academic career can be built. Several oft-cited randomized controlled trials have fueled both private and public interest and funding.
However, a recent commentary published in Science suggests that all programs are “not unequivocally positive and much more research is needed.” “Worrisome results in Tennessee,” “Success in Boston,” and “Largely null results for Headstart” are just a few of the article’s section titles and convey a sense of the inconsistency the investigators found as they reviewed early education systems around the country.
While there may be some politicians who may attempt to use the results of this investigation as a reason to cancel public funding of underperforming early education programs, the authors avoid this baby-and-the-bathwater conclusion. Instead, they urge more rigorous research “to understand how effective programs can be designed and implemented.”
The kind of re-thinking and brainstorming these investigators suggest takes time. While we’re waiting for this process to gain traction, this might be a good time to consider some of the benefits of early education that we don’t usually consider when our focus is on academic metrics.
A recent paper in Children’s Health Care by investigators at the Boston University Medical Center and School of Medicine considered the diet of children attending preschool. Looking at the dietary records of more than 300 children attending 30 childcare centers, the researchers found that the children’s diets before arrival at daycare was less healthy than while they were in daycare. “The hour after pickup appeared to be the least healthful” of any of the time periods surveyed. Of course, we will all conjure up images of what this chaotic post-daycare pickup may look like and cut the harried parents and grandparents some slack when it comes to nutritional choices. However, the bottom line is that for the group of children surveyed being in preschool or daycare protected them from a less healthy diet they were being provided outside of school hours.
Our recent experience with pandemic-related school closures provides more evidence that being in school was superior to any remote experience academically. School-age children and adolescents gained weight when school closures were the norm. Play patterns for children shifted from outdoor play to indoor play — often dominated by more sedentary video games. Both fatal and non-fatal gun-related injuries surged during the pandemic and, by far, the majority of these occur in the home and not at school.
Stepping back to look at this broader picture that includes diet, physical activity, and safety — not to mention the benefits of socialization — leads one to arrive at the unfortunate conclusion that Of course there will be those who point to the belief that schools are petri dishes putting children at greater risk for respiratory infections. On the other hand, we must accept that schools haven’t proved to be a major factor in the spread of COVID that many had feared.
The authors of the study in Science are certainly correct in recommending a more thorough investigation into the academic benefits of preschool education. However, we must keep in mind that preschool offers an environment that can be a positive influence on young children.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].