User login
Sex differences seen in inflammatory arthritis health care use
Women with inflammatory arthritis (IA) are more likely to use healthcare services than men, a Canadian study found. The results suggest there are biological differences in disease course and sociocultural differences in health care access and patient behavior among the sexes, Sanjana Tarannum said in a presentation at the Lancet Summit on Sex and Gender in Rheumatology.
Ms. Tarannum and colleagues also recently published the study in Annals of the Rheumatic Diseases.
Effectively managing IA patients calls for timely access to and appropriate use of health care resources, said Ms. Tarannum, of the Women’s College Research Institute in Toronto.
Sex and gender are often used interchangeably but they refer to different things. “Sex is the biological characteristic of being male or female. It relates to disease inheritance patterns, pain processing mechanisms, and immune dysregulation in the context of inflammatory arthritis,” Ms. Tarannum said during her presentation.
Gender is a sociocultural construct associated with masculine or feminine traits. In the context of IA, gender relates to coping strategies, pain perception and reporting, and health care–seeking behavior of patients and interaction with care providers.
A patient’s sex relates to healthcare encounters, time to diagnosis, and prescription patterns. These all affect disease outcomes. Previous studies have yielded inconsistent results and mainly focused on rheumatoid arthritis rather than other IA types such as ankylosing spondylitis (AS).
Ms. Tarannum and colleagues sought to compare health care usage between male and female patients for musculoskeletal-related issues before and after IA diagnosis. They used Ontario administrative health data to create three cohorts of patients with RA, AS, and psoriatic arthritis (PsA), the three most common types of IA. The patients were diagnosed during 2010-2017, and outcomes were assessed in each year for 3 years before and after diagnosis.
Health care use indicators included visits to physicians, musculoskeletal imaging, laboratory tests, and dispensation of drugs. Regression models adjusting for sociodemographic factors and comorbidities were used to compare male and female patients.
Sex-related differences emerge in all IA groups
The investigators assessed 41,277 patients with RA (69% female), 8,150 patients with AS (51% female), and 6,446 patients with PsA (54% female). Male patients had more cardiovascular disease, whereas female patients had higher incidences of depression and osteoporosis.
Similar trends of sex-related differences emerged in all three cohorts. Before diagnosis, female patients were more likely to visit rheumatologists or family physicians for musculoskeletal reasons or use musculoskeletal imaging and laboratory tests. Women were also more likely to remain in rheumatology care after diagnosis.
Men were more likely to visit the ED for musculoskeletal reasons immediately before diagnosis.
No sex- or gender-related differences were observed in medication use, although older females with RA or AS were more likely to get prescriptions for NSAIDs and opioids and conventional disease-modifying antirheumatic drugs, respectively.
The findings show that overall musculoskeletal health care use was higher in female patients with IA. “Sex differences were more pronounced the earlier the encounter was from the time of diagnosis and tended to diminish with time,” Ms. Tarannum observed. Sex differences were also more prominent in the RA and AS cohorts.
Women seek out care, do repeat visits
Several reasons may explain why utilization was higher in females. Women with IA have a higher overall risk of musculoskeletal conditions such as osteoarthritis, which could have driven the health care encounters. Numerous studies have also reported that female patients have a lower threshold for pain as well as a greater tendency to seek out health care.
Additionally, female patients often present with pain and fatigue, which are often misdiagnosed as fibromyalgia or depression. Therefore, they often require repeated health care encounters to arrive at an IA diagnosis, Ms. Tarannum said.
An early prodromal phase in females could have triggered a health care encounter as well.
Men, by comparison, are more likely to have acute-onset or severe disease. Objective signs and radiologic features can facilitate diagnosis in men, she said. Male patients also show more reluctance in seeking care, have a higher threshold for pain, and are less likely to have a usual source of care such as a family physician.
Higher confidence in hospital-based emergency services also could have resulted in more ED visits and lower health care use in men. Better response to treatments could also have resulted in fewer episodes of rheumatology care after diagnosis.
The results aren’t surprising, said Scott Zashin, MD, a rheumatologist in Dallas who wasn’t a part of the study.
“At least in terms of musculoskeletal disorders, my clinical experience suggests that women are more compliant with their follow-up than male patients. Especially with gout, a common type of arthritis in men, male patients may wait until their symptoms are severe before seeking medical attention,” Dr. Zashin said.
The Enid Walker Graduate Student Award for Research in Women’s Health provided funding for this study.
A version of this article first appeared on Medscape.com.
Women with inflammatory arthritis (IA) are more likely to use healthcare services than men, a Canadian study found. The results suggest there are biological differences in disease course and sociocultural differences in health care access and patient behavior among the sexes, Sanjana Tarannum said in a presentation at the Lancet Summit on Sex and Gender in Rheumatology.
Ms. Tarannum and colleagues also recently published the study in Annals of the Rheumatic Diseases.
Effectively managing IA patients calls for timely access to and appropriate use of health care resources, said Ms. Tarannum, of the Women’s College Research Institute in Toronto.
Sex and gender are often used interchangeably but they refer to different things. “Sex is the biological characteristic of being male or female. It relates to disease inheritance patterns, pain processing mechanisms, and immune dysregulation in the context of inflammatory arthritis,” Ms. Tarannum said during her presentation.
Gender is a sociocultural construct associated with masculine or feminine traits. In the context of IA, gender relates to coping strategies, pain perception and reporting, and health care–seeking behavior of patients and interaction with care providers.
A patient’s sex relates to healthcare encounters, time to diagnosis, and prescription patterns. These all affect disease outcomes. Previous studies have yielded inconsistent results and mainly focused on rheumatoid arthritis rather than other IA types such as ankylosing spondylitis (AS).
Ms. Tarannum and colleagues sought to compare health care usage between male and female patients for musculoskeletal-related issues before and after IA diagnosis. They used Ontario administrative health data to create three cohorts of patients with RA, AS, and psoriatic arthritis (PsA), the three most common types of IA. The patients were diagnosed during 2010-2017, and outcomes were assessed in each year for 3 years before and after diagnosis.
Health care use indicators included visits to physicians, musculoskeletal imaging, laboratory tests, and dispensation of drugs. Regression models adjusting for sociodemographic factors and comorbidities were used to compare male and female patients.
Sex-related differences emerge in all IA groups
The investigators assessed 41,277 patients with RA (69% female), 8,150 patients with AS (51% female), and 6,446 patients with PsA (54% female). Male patients had more cardiovascular disease, whereas female patients had higher incidences of depression and osteoporosis.
Similar trends of sex-related differences emerged in all three cohorts. Before diagnosis, female patients were more likely to visit rheumatologists or family physicians for musculoskeletal reasons or use musculoskeletal imaging and laboratory tests. Women were also more likely to remain in rheumatology care after diagnosis.
Men were more likely to visit the ED for musculoskeletal reasons immediately before diagnosis.
No sex- or gender-related differences were observed in medication use, although older females with RA or AS were more likely to get prescriptions for NSAIDs and opioids and conventional disease-modifying antirheumatic drugs, respectively.
The findings show that overall musculoskeletal health care use was higher in female patients with IA. “Sex differences were more pronounced the earlier the encounter was from the time of diagnosis and tended to diminish with time,” Ms. Tarannum observed. Sex differences were also more prominent in the RA and AS cohorts.
Women seek out care, do repeat visits
Several reasons may explain why utilization was higher in females. Women with IA have a higher overall risk of musculoskeletal conditions such as osteoarthritis, which could have driven the health care encounters. Numerous studies have also reported that female patients have a lower threshold for pain as well as a greater tendency to seek out health care.
Additionally, female patients often present with pain and fatigue, which are often misdiagnosed as fibromyalgia or depression. Therefore, they often require repeated health care encounters to arrive at an IA diagnosis, Ms. Tarannum said.
An early prodromal phase in females could have triggered a health care encounter as well.
Men, by comparison, are more likely to have acute-onset or severe disease. Objective signs and radiologic features can facilitate diagnosis in men, she said. Male patients also show more reluctance in seeking care, have a higher threshold for pain, and are less likely to have a usual source of care such as a family physician.
Higher confidence in hospital-based emergency services also could have resulted in more ED visits and lower health care use in men. Better response to treatments could also have resulted in fewer episodes of rheumatology care after diagnosis.
The results aren’t surprising, said Scott Zashin, MD, a rheumatologist in Dallas who wasn’t a part of the study.
“At least in terms of musculoskeletal disorders, my clinical experience suggests that women are more compliant with their follow-up than male patients. Especially with gout, a common type of arthritis in men, male patients may wait until their symptoms are severe before seeking medical attention,” Dr. Zashin said.
The Enid Walker Graduate Student Award for Research in Women’s Health provided funding for this study.
A version of this article first appeared on Medscape.com.
Women with inflammatory arthritis (IA) are more likely to use healthcare services than men, a Canadian study found. The results suggest there are biological differences in disease course and sociocultural differences in health care access and patient behavior among the sexes, Sanjana Tarannum said in a presentation at the Lancet Summit on Sex and Gender in Rheumatology.
Ms. Tarannum and colleagues also recently published the study in Annals of the Rheumatic Diseases.
Effectively managing IA patients calls for timely access to and appropriate use of health care resources, said Ms. Tarannum, of the Women’s College Research Institute in Toronto.
Sex and gender are often used interchangeably but they refer to different things. “Sex is the biological characteristic of being male or female. It relates to disease inheritance patterns, pain processing mechanisms, and immune dysregulation in the context of inflammatory arthritis,” Ms. Tarannum said during her presentation.
Gender is a sociocultural construct associated with masculine or feminine traits. In the context of IA, gender relates to coping strategies, pain perception and reporting, and health care–seeking behavior of patients and interaction with care providers.
A patient’s sex relates to healthcare encounters, time to diagnosis, and prescription patterns. These all affect disease outcomes. Previous studies have yielded inconsistent results and mainly focused on rheumatoid arthritis rather than other IA types such as ankylosing spondylitis (AS).
Ms. Tarannum and colleagues sought to compare health care usage between male and female patients for musculoskeletal-related issues before and after IA diagnosis. They used Ontario administrative health data to create three cohorts of patients with RA, AS, and psoriatic arthritis (PsA), the three most common types of IA. The patients were diagnosed during 2010-2017, and outcomes were assessed in each year for 3 years before and after diagnosis.
Health care use indicators included visits to physicians, musculoskeletal imaging, laboratory tests, and dispensation of drugs. Regression models adjusting for sociodemographic factors and comorbidities were used to compare male and female patients.
Sex-related differences emerge in all IA groups
The investigators assessed 41,277 patients with RA (69% female), 8,150 patients with AS (51% female), and 6,446 patients with PsA (54% female). Male patients had more cardiovascular disease, whereas female patients had higher incidences of depression and osteoporosis.
Similar trends of sex-related differences emerged in all three cohorts. Before diagnosis, female patients were more likely to visit rheumatologists or family physicians for musculoskeletal reasons or use musculoskeletal imaging and laboratory tests. Women were also more likely to remain in rheumatology care after diagnosis.
Men were more likely to visit the ED for musculoskeletal reasons immediately before diagnosis.
No sex- or gender-related differences were observed in medication use, although older females with RA or AS were more likely to get prescriptions for NSAIDs and opioids and conventional disease-modifying antirheumatic drugs, respectively.
The findings show that overall musculoskeletal health care use was higher in female patients with IA. “Sex differences were more pronounced the earlier the encounter was from the time of diagnosis and tended to diminish with time,” Ms. Tarannum observed. Sex differences were also more prominent in the RA and AS cohorts.
Women seek out care, do repeat visits
Several reasons may explain why utilization was higher in females. Women with IA have a higher overall risk of musculoskeletal conditions such as osteoarthritis, which could have driven the health care encounters. Numerous studies have also reported that female patients have a lower threshold for pain as well as a greater tendency to seek out health care.
Additionally, female patients often present with pain and fatigue, which are often misdiagnosed as fibromyalgia or depression. Therefore, they often require repeated health care encounters to arrive at an IA diagnosis, Ms. Tarannum said.
An early prodromal phase in females could have triggered a health care encounter as well.
Men, by comparison, are more likely to have acute-onset or severe disease. Objective signs and radiologic features can facilitate diagnosis in men, she said. Male patients also show more reluctance in seeking care, have a higher threshold for pain, and are less likely to have a usual source of care such as a family physician.
Higher confidence in hospital-based emergency services also could have resulted in more ED visits and lower health care use in men. Better response to treatments could also have resulted in fewer episodes of rheumatology care after diagnosis.
The results aren’t surprising, said Scott Zashin, MD, a rheumatologist in Dallas who wasn’t a part of the study.
“At least in terms of musculoskeletal disorders, my clinical experience suggests that women are more compliant with their follow-up than male patients. Especially with gout, a common type of arthritis in men, male patients may wait until their symptoms are severe before seeking medical attention,” Dr. Zashin said.
The Enid Walker Graduate Student Award for Research in Women’s Health provided funding for this study.
A version of this article first appeared on Medscape.com.
FROM THE LANCET SUMMIT ON SEX AND GENDER IN RHEUMATOLOGY
Why can’t U.K. immunocompromised patients get Evusheld?
This transcript has been edited for clarity.
I’m David Kerr, professor of cancer medicine at Oxford. As I’m gearing up to have my autumnal COVID-19 booster vaccine,
This was developed by AstraZeneca. It’s a combination of two relatively long-acting antibodies (tixagevimab and cilgavimab) that bind to the spike protein on the outside of the SARS-CoV-2 virus, the virus that causes COVID-19. The antibody binds to the spike protein and prevents it from binding to and infecting or damaging cells, so it’s what’s called preexposure prophylaxis.
Although vaccination is still the best approach to protecting against and, one would hope, conferring a degree of herd protection to our population as a whole, there are some people who cannot mount an appropriate immune response and we have to take care of these folks. Because the vaccines don’t work very well for them, the vaccine itself is not sufficient to protect them.
Evusheld, in trials that have been done hitherto, can protect people who can’t mount an immune response from being infected. Between 75% and 80% of patients treated with Evusheld didn’t get COVID-19. The duration of effect seemed to be at least for 6 months, possibly longer, so it’s a really good result. This caused our medicines regulatory authority in the United Kingdom to approve the drug in March of this year. Although the drug has been approved, it’s not yet funded and not yet available for vulnerable patients.
These are patients who, for reasons of inborn genetic diseases, cannot mount an immune response; patients who are pharmacologically immune depleted; patients who have had transplants and are on immunosuppressive drugs; and some of our cancer patients, particularly those with blood or hematologic malignancies, who can receive very heavy treatment that can pound the immune system to bits.
These are, in the population as a whole, relatively small numbers, but an important number of people who are still vulnerable to developing COVID-19 despite vaccination.
Why isn’t the drug available? We have a two-stage process in the United Kingdom. We have the scientists and regulatory authorities looking at the evidence and data and saying, “Yes, it stacks up. This drug is effective and safe to some extent.”
The second phase is a health technology assessment undertaken by NICE, our National Institute for Health and Care Excellence – something that I’ve talked about a number of times before and the sometimes seemingly arbitrary decisions that they make. NICE hasn’t evaluated the drug yet, and the British government has held out because they are arguing that we don’t have enough data.
The trials with Evusheld were done before the Omicron variant dominated, as it does now; therefore, they are looking to try to work with AstraZeneca to generate more real-world data to show that Evusheld would prevent infection from the Omicron variant of the virus. Equally as important, how long does that protection last? Is it as protective against Omicron, and what’s the duration of that protection? Those bits of work are going on now.
Some real-world data are starting to emerge, showing that Evusheld will offer some degree of protection against Omicron, but there are still question marks about duration and the proportion of the population that would benefit.
NICE aren’t due to report on this – although the drug was approved in March of this year – until next year some time. That’s what’s caused a degree of consternation in the community of patients that we serve. Some of my clinical colleagues are beating the drum, saying, “We must have this drug now.” We’re still waiting on NICE to announce.
One obvious way to go around this is the government, which has bent over backwards in the United Kingdom to do as much as it can to protect the population from COVID-19. There was fantastic vaccine rollout and an extraordinary economic package to support individuals during lockdown to maintain the workforce, to support families and people at home. They’ve done a fantastic job.
Wanting to damp down this controversy, perhaps the sensible thing would be to ask NICE to evaluate the data that they have just now, to allow AstraZeneca to present whatever real-world evidence they have, and although it may not be perfect, it may be sufficient – we don’t know – to pass the NICE health technology assessment.
Watch this space. Let’s see what happens. If I were government, that’s what I would do. I would ask NICE to bring their appraisal forward. I would ask them to work with AstraZeneca to go over every ounce and iota of data that they have to see if this drug will be sufficiently effective and sufficiently cost-effective to be used before winter comes. I think the whole world is holding its breath, expecting another COVID-19 winter surge. Now would be the time to act.
What do you think? Here we are in the United Kingdom discussing yet another quasi–”health-rationing” problem. It’s not. This is about collecting more data and being as rational as possible. Can we accelerate that process? Perhaps.
Thanks for listening. I’d be very grateful for any comments that you might choose to make.
David J. Kerr, MD, DSc, is a professor of cancer medicine at the University of Oxford (England). He disclosed financial relationships with Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Bayer HealthCare Pharmaceuticals, Genomic Health, Merck Serono, Roche, and Celleron Therapeutics.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m David Kerr, professor of cancer medicine at Oxford. As I’m gearing up to have my autumnal COVID-19 booster vaccine,
This was developed by AstraZeneca. It’s a combination of two relatively long-acting antibodies (tixagevimab and cilgavimab) that bind to the spike protein on the outside of the SARS-CoV-2 virus, the virus that causes COVID-19. The antibody binds to the spike protein and prevents it from binding to and infecting or damaging cells, so it’s what’s called preexposure prophylaxis.
Although vaccination is still the best approach to protecting against and, one would hope, conferring a degree of herd protection to our population as a whole, there are some people who cannot mount an appropriate immune response and we have to take care of these folks. Because the vaccines don’t work very well for them, the vaccine itself is not sufficient to protect them.
Evusheld, in trials that have been done hitherto, can protect people who can’t mount an immune response from being infected. Between 75% and 80% of patients treated with Evusheld didn’t get COVID-19. The duration of effect seemed to be at least for 6 months, possibly longer, so it’s a really good result. This caused our medicines regulatory authority in the United Kingdom to approve the drug in March of this year. Although the drug has been approved, it’s not yet funded and not yet available for vulnerable patients.
These are patients who, for reasons of inborn genetic diseases, cannot mount an immune response; patients who are pharmacologically immune depleted; patients who have had transplants and are on immunosuppressive drugs; and some of our cancer patients, particularly those with blood or hematologic malignancies, who can receive very heavy treatment that can pound the immune system to bits.
These are, in the population as a whole, relatively small numbers, but an important number of people who are still vulnerable to developing COVID-19 despite vaccination.
Why isn’t the drug available? We have a two-stage process in the United Kingdom. We have the scientists and regulatory authorities looking at the evidence and data and saying, “Yes, it stacks up. This drug is effective and safe to some extent.”
The second phase is a health technology assessment undertaken by NICE, our National Institute for Health and Care Excellence – something that I’ve talked about a number of times before and the sometimes seemingly arbitrary decisions that they make. NICE hasn’t evaluated the drug yet, and the British government has held out because they are arguing that we don’t have enough data.
The trials with Evusheld were done before the Omicron variant dominated, as it does now; therefore, they are looking to try to work with AstraZeneca to generate more real-world data to show that Evusheld would prevent infection from the Omicron variant of the virus. Equally as important, how long does that protection last? Is it as protective against Omicron, and what’s the duration of that protection? Those bits of work are going on now.
Some real-world data are starting to emerge, showing that Evusheld will offer some degree of protection against Omicron, but there are still question marks about duration and the proportion of the population that would benefit.
NICE aren’t due to report on this – although the drug was approved in March of this year – until next year some time. That’s what’s caused a degree of consternation in the community of patients that we serve. Some of my clinical colleagues are beating the drum, saying, “We must have this drug now.” We’re still waiting on NICE to announce.
One obvious way to go around this is the government, which has bent over backwards in the United Kingdom to do as much as it can to protect the population from COVID-19. There was fantastic vaccine rollout and an extraordinary economic package to support individuals during lockdown to maintain the workforce, to support families and people at home. They’ve done a fantastic job.
Wanting to damp down this controversy, perhaps the sensible thing would be to ask NICE to evaluate the data that they have just now, to allow AstraZeneca to present whatever real-world evidence they have, and although it may not be perfect, it may be sufficient – we don’t know – to pass the NICE health technology assessment.
Watch this space. Let’s see what happens. If I were government, that’s what I would do. I would ask NICE to bring their appraisal forward. I would ask them to work with AstraZeneca to go over every ounce and iota of data that they have to see if this drug will be sufficiently effective and sufficiently cost-effective to be used before winter comes. I think the whole world is holding its breath, expecting another COVID-19 winter surge. Now would be the time to act.
What do you think? Here we are in the United Kingdom discussing yet another quasi–”health-rationing” problem. It’s not. This is about collecting more data and being as rational as possible. Can we accelerate that process? Perhaps.
Thanks for listening. I’d be very grateful for any comments that you might choose to make.
David J. Kerr, MD, DSc, is a professor of cancer medicine at the University of Oxford (England). He disclosed financial relationships with Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Bayer HealthCare Pharmaceuticals, Genomic Health, Merck Serono, Roche, and Celleron Therapeutics.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m David Kerr, professor of cancer medicine at Oxford. As I’m gearing up to have my autumnal COVID-19 booster vaccine,
This was developed by AstraZeneca. It’s a combination of two relatively long-acting antibodies (tixagevimab and cilgavimab) that bind to the spike protein on the outside of the SARS-CoV-2 virus, the virus that causes COVID-19. The antibody binds to the spike protein and prevents it from binding to and infecting or damaging cells, so it’s what’s called preexposure prophylaxis.
Although vaccination is still the best approach to protecting against and, one would hope, conferring a degree of herd protection to our population as a whole, there are some people who cannot mount an appropriate immune response and we have to take care of these folks. Because the vaccines don’t work very well for them, the vaccine itself is not sufficient to protect them.
Evusheld, in trials that have been done hitherto, can protect people who can’t mount an immune response from being infected. Between 75% and 80% of patients treated with Evusheld didn’t get COVID-19. The duration of effect seemed to be at least for 6 months, possibly longer, so it’s a really good result. This caused our medicines regulatory authority in the United Kingdom to approve the drug in March of this year. Although the drug has been approved, it’s not yet funded and not yet available for vulnerable patients.
These are patients who, for reasons of inborn genetic diseases, cannot mount an immune response; patients who are pharmacologically immune depleted; patients who have had transplants and are on immunosuppressive drugs; and some of our cancer patients, particularly those with blood or hematologic malignancies, who can receive very heavy treatment that can pound the immune system to bits.
These are, in the population as a whole, relatively small numbers, but an important number of people who are still vulnerable to developing COVID-19 despite vaccination.
Why isn’t the drug available? We have a two-stage process in the United Kingdom. We have the scientists and regulatory authorities looking at the evidence and data and saying, “Yes, it stacks up. This drug is effective and safe to some extent.”
The second phase is a health technology assessment undertaken by NICE, our National Institute for Health and Care Excellence – something that I’ve talked about a number of times before and the sometimes seemingly arbitrary decisions that they make. NICE hasn’t evaluated the drug yet, and the British government has held out because they are arguing that we don’t have enough data.
The trials with Evusheld were done before the Omicron variant dominated, as it does now; therefore, they are looking to try to work with AstraZeneca to generate more real-world data to show that Evusheld would prevent infection from the Omicron variant of the virus. Equally as important, how long does that protection last? Is it as protective against Omicron, and what’s the duration of that protection? Those bits of work are going on now.
Some real-world data are starting to emerge, showing that Evusheld will offer some degree of protection against Omicron, but there are still question marks about duration and the proportion of the population that would benefit.
NICE aren’t due to report on this – although the drug was approved in March of this year – until next year some time. That’s what’s caused a degree of consternation in the community of patients that we serve. Some of my clinical colleagues are beating the drum, saying, “We must have this drug now.” We’re still waiting on NICE to announce.
One obvious way to go around this is the government, which has bent over backwards in the United Kingdom to do as much as it can to protect the population from COVID-19. There was fantastic vaccine rollout and an extraordinary economic package to support individuals during lockdown to maintain the workforce, to support families and people at home. They’ve done a fantastic job.
Wanting to damp down this controversy, perhaps the sensible thing would be to ask NICE to evaluate the data that they have just now, to allow AstraZeneca to present whatever real-world evidence they have, and although it may not be perfect, it may be sufficient – we don’t know – to pass the NICE health technology assessment.
Watch this space. Let’s see what happens. If I were government, that’s what I would do. I would ask NICE to bring their appraisal forward. I would ask them to work with AstraZeneca to go over every ounce and iota of data that they have to see if this drug will be sufficiently effective and sufficiently cost-effective to be used before winter comes. I think the whole world is holding its breath, expecting another COVID-19 winter surge. Now would be the time to act.
What do you think? Here we are in the United Kingdom discussing yet another quasi–”health-rationing” problem. It’s not. This is about collecting more data and being as rational as possible. Can we accelerate that process? Perhaps.
Thanks for listening. I’d be very grateful for any comments that you might choose to make.
David J. Kerr, MD, DSc, is a professor of cancer medicine at the University of Oxford (England). He disclosed financial relationships with Oxford Cancer Biomarkers, Afrox, GlaxoSmithKline, Bayer HealthCare Pharmaceuticals, Genomic Health, Merck Serono, Roche, and Celleron Therapeutics.
A version of this article first appeared on Medscape.com.
Cost paramount when choosing metastatic breast cancer treatment
While efficacy and quality of life outcomes are similar across commonly used treatments for endocrine-refractory or triple-negative metastatic breast cancer, the costs of these agents vary widely, a recent analysis reveals.
Notably, the authors found that
Given “razor thin” differences in outcomes, cost should become a major consideration, the researchers concluded.
“As a society, we urgently need more strategies to reduce cancer drug costs without compromising outcomes, and our analysis provides quantifiable evidence to help providers choose lower priced, but equally effective sequences of drugs,” first author Stephanie B. Wheeler, PhD, from the University of North Carolina at Chapel Hill, explained in a press release.
Although the drugs Dr. Wheeler and colleagues studied are reimbursed in the metastatic breast cancer setting, “the optimal sequencing of them has been unclear, which has led to considerable variation in physician preference and practice,” Dr. Wheeler said.
In the study, published in the Journal of Clinical Oncology, Dr. Wheeler and colleagues estimated the cost-effectiveness of different therapeutic options from the first- to third-line setting for this patient population.
The researchers used three dynamic microsimulation computer models to predict how hypothetical sets of 10,000 patients with specific types of metastatic breast cancer would respond to various therapy types and sequences. The cohorts were grouped according to prior chemotherapy exposure: cohort 1 had no taxane or anthracycline exposure, cohort 2 had taxane and anthracycline exposure, and cohort 3 had taxane exposure but was anthracycline naive.
On the basis of feedback from oncologists, the investigators focused on different agents in the three cohorts: paclitaxel, capecitabine, or pegylated liposomal doxorubicin for cohort 1; eribulin, capecitabine, or carboplatin for cohort 2; and pegylated liposomal doxorubicin, capecitabine, or eribulin for cohort 3.
Overall, the models showed “nearly indistinguishable differences” in quality of life. In fact, the “razor-thin incremental differences in quality-adjusted survival” across the treatment sequences often amounted to differences of only a few days or weeks, the authors noted, adding that, even in the most extreme of cases, 3 weeks separated the best and worst options for quality-adjusted life-years.
But the models did show considerable differences in costs.
The authors found that, for cohort 1, treatment with paclitaxel followed by capecitabine and then pegylated liposomal doxorubicin corresponded to the highest expected quality-adjusted life-year gain and the lowest costs – $686 per month versus the highest cost option of $1,765.
For cohort 2, treatment with carboplatin followed by capecitabine and then eribulin corresponded to the highest expected quality-adjusted life-year gain and lowest costs.
For cohort 3, treatment sequences beginning with capecitabine or pegylated liposomal doxorubicin followed by eribulin was most cost effective.
Notably, the authors found that eribulin – the most expensive treatment with a high expected adverse event burden – performed particularly poorly in the two cohorts in which it was evaluated, “suggesting it should be used last in a sequence, on the basis of cost-effectiveness alone.”
In other words, “more spending on cancer care does not necessarily confer greater health benefits,” said Dr. Wheeler, also a professor of health policy.
“I hope our study will help expand the framework that we use to make these decisions from one where we just think about the biologic action of the drug to one where we also consider the bigger picture of what the treatment experience is like for the patient, including their financial burden, investment of time, and side effects,” study coauthor Katherine E. Reeder-Hayes, MD, section chief of breast oncology at UNC, said in the press release.
The results demonstrate that therapeutic decisions in the endocrine-refractory or triple-negative metastatic setting “may prioritize costs without affecting clinical outcomes” and highlight the direct impact that a “high-quality, transparent, and accessible economic analysis” can have on patient care, Scott D. Ramsey, MD, PhD, of Fred Hutchinson Cancer Research Center, Seattle, and colleagues wrote in an accompanying editorial.
Following the treatment sequences outlined in this study would “reduce patient financial burden and save our health system hundreds of millions of dollars annually,” the editorialists wrote.
As for next steps, Dr. Wheeler and colleagues have developed a financial navigation program to help patients manage their out-of-pocket cancer care costs and are currently scaling up the intervention in nine rural and nonrural oncology practices across North Carolina.
The study was supported by the Center for Disease Control and Prevention through the Prevention Research Centers Program. Dr. Wheeler has received research funding and payment for travel, accommodations, and expenses from Pfizer. Dr. Ramsey has had consulting or advisory roles and has received research funding and/or payment for travel, accommodations, and expenses from Bayer, Genentech, AstraZeneca, Merck, GRAIL, Seattle Genetics, Biovica, and/or Flatiron Health. Because of their editorial roles at the journal, the Journal of Clinical Oncology recused Dr. Wheeler and Dr. Ramsey from having any role in the peer review of their respective manuscripts.
A version of this article first appeared on Medscape.com.
While efficacy and quality of life outcomes are similar across commonly used treatments for endocrine-refractory or triple-negative metastatic breast cancer, the costs of these agents vary widely, a recent analysis reveals.
Notably, the authors found that
Given “razor thin” differences in outcomes, cost should become a major consideration, the researchers concluded.
“As a society, we urgently need more strategies to reduce cancer drug costs without compromising outcomes, and our analysis provides quantifiable evidence to help providers choose lower priced, but equally effective sequences of drugs,” first author Stephanie B. Wheeler, PhD, from the University of North Carolina at Chapel Hill, explained in a press release.
Although the drugs Dr. Wheeler and colleagues studied are reimbursed in the metastatic breast cancer setting, “the optimal sequencing of them has been unclear, which has led to considerable variation in physician preference and practice,” Dr. Wheeler said.
In the study, published in the Journal of Clinical Oncology, Dr. Wheeler and colleagues estimated the cost-effectiveness of different therapeutic options from the first- to third-line setting for this patient population.
The researchers used three dynamic microsimulation computer models to predict how hypothetical sets of 10,000 patients with specific types of metastatic breast cancer would respond to various therapy types and sequences. The cohorts were grouped according to prior chemotherapy exposure: cohort 1 had no taxane or anthracycline exposure, cohort 2 had taxane and anthracycline exposure, and cohort 3 had taxane exposure but was anthracycline naive.
On the basis of feedback from oncologists, the investigators focused on different agents in the three cohorts: paclitaxel, capecitabine, or pegylated liposomal doxorubicin for cohort 1; eribulin, capecitabine, or carboplatin for cohort 2; and pegylated liposomal doxorubicin, capecitabine, or eribulin for cohort 3.
Overall, the models showed “nearly indistinguishable differences” in quality of life. In fact, the “razor-thin incremental differences in quality-adjusted survival” across the treatment sequences often amounted to differences of only a few days or weeks, the authors noted, adding that, even in the most extreme of cases, 3 weeks separated the best and worst options for quality-adjusted life-years.
But the models did show considerable differences in costs.
The authors found that, for cohort 1, treatment with paclitaxel followed by capecitabine and then pegylated liposomal doxorubicin corresponded to the highest expected quality-adjusted life-year gain and the lowest costs – $686 per month versus the highest cost option of $1,765.
For cohort 2, treatment with carboplatin followed by capecitabine and then eribulin corresponded to the highest expected quality-adjusted life-year gain and lowest costs.
For cohort 3, treatment sequences beginning with capecitabine or pegylated liposomal doxorubicin followed by eribulin was most cost effective.
Notably, the authors found that eribulin – the most expensive treatment with a high expected adverse event burden – performed particularly poorly in the two cohorts in which it was evaluated, “suggesting it should be used last in a sequence, on the basis of cost-effectiveness alone.”
In other words, “more spending on cancer care does not necessarily confer greater health benefits,” said Dr. Wheeler, also a professor of health policy.
“I hope our study will help expand the framework that we use to make these decisions from one where we just think about the biologic action of the drug to one where we also consider the bigger picture of what the treatment experience is like for the patient, including their financial burden, investment of time, and side effects,” study coauthor Katherine E. Reeder-Hayes, MD, section chief of breast oncology at UNC, said in the press release.
The results demonstrate that therapeutic decisions in the endocrine-refractory or triple-negative metastatic setting “may prioritize costs without affecting clinical outcomes” and highlight the direct impact that a “high-quality, transparent, and accessible economic analysis” can have on patient care, Scott D. Ramsey, MD, PhD, of Fred Hutchinson Cancer Research Center, Seattle, and colleagues wrote in an accompanying editorial.
Following the treatment sequences outlined in this study would “reduce patient financial burden and save our health system hundreds of millions of dollars annually,” the editorialists wrote.
As for next steps, Dr. Wheeler and colleagues have developed a financial navigation program to help patients manage their out-of-pocket cancer care costs and are currently scaling up the intervention in nine rural and nonrural oncology practices across North Carolina.
The study was supported by the Center for Disease Control and Prevention through the Prevention Research Centers Program. Dr. Wheeler has received research funding and payment for travel, accommodations, and expenses from Pfizer. Dr. Ramsey has had consulting or advisory roles and has received research funding and/or payment for travel, accommodations, and expenses from Bayer, Genentech, AstraZeneca, Merck, GRAIL, Seattle Genetics, Biovica, and/or Flatiron Health. Because of their editorial roles at the journal, the Journal of Clinical Oncology recused Dr. Wheeler and Dr. Ramsey from having any role in the peer review of their respective manuscripts.
A version of this article first appeared on Medscape.com.
While efficacy and quality of life outcomes are similar across commonly used treatments for endocrine-refractory or triple-negative metastatic breast cancer, the costs of these agents vary widely, a recent analysis reveals.
Notably, the authors found that
Given “razor thin” differences in outcomes, cost should become a major consideration, the researchers concluded.
“As a society, we urgently need more strategies to reduce cancer drug costs without compromising outcomes, and our analysis provides quantifiable evidence to help providers choose lower priced, but equally effective sequences of drugs,” first author Stephanie B. Wheeler, PhD, from the University of North Carolina at Chapel Hill, explained in a press release.
Although the drugs Dr. Wheeler and colleagues studied are reimbursed in the metastatic breast cancer setting, “the optimal sequencing of them has been unclear, which has led to considerable variation in physician preference and practice,” Dr. Wheeler said.
In the study, published in the Journal of Clinical Oncology, Dr. Wheeler and colleagues estimated the cost-effectiveness of different therapeutic options from the first- to third-line setting for this patient population.
The researchers used three dynamic microsimulation computer models to predict how hypothetical sets of 10,000 patients with specific types of metastatic breast cancer would respond to various therapy types and sequences. The cohorts were grouped according to prior chemotherapy exposure: cohort 1 had no taxane or anthracycline exposure, cohort 2 had taxane and anthracycline exposure, and cohort 3 had taxane exposure but was anthracycline naive.
On the basis of feedback from oncologists, the investigators focused on different agents in the three cohorts: paclitaxel, capecitabine, or pegylated liposomal doxorubicin for cohort 1; eribulin, capecitabine, or carboplatin for cohort 2; and pegylated liposomal doxorubicin, capecitabine, or eribulin for cohort 3.
Overall, the models showed “nearly indistinguishable differences” in quality of life. In fact, the “razor-thin incremental differences in quality-adjusted survival” across the treatment sequences often amounted to differences of only a few days or weeks, the authors noted, adding that, even in the most extreme of cases, 3 weeks separated the best and worst options for quality-adjusted life-years.
But the models did show considerable differences in costs.
The authors found that, for cohort 1, treatment with paclitaxel followed by capecitabine and then pegylated liposomal doxorubicin corresponded to the highest expected quality-adjusted life-year gain and the lowest costs – $686 per month versus the highest cost option of $1,765.
For cohort 2, treatment with carboplatin followed by capecitabine and then eribulin corresponded to the highest expected quality-adjusted life-year gain and lowest costs.
For cohort 3, treatment sequences beginning with capecitabine or pegylated liposomal doxorubicin followed by eribulin was most cost effective.
Notably, the authors found that eribulin – the most expensive treatment with a high expected adverse event burden – performed particularly poorly in the two cohorts in which it was evaluated, “suggesting it should be used last in a sequence, on the basis of cost-effectiveness alone.”
In other words, “more spending on cancer care does not necessarily confer greater health benefits,” said Dr. Wheeler, also a professor of health policy.
“I hope our study will help expand the framework that we use to make these decisions from one where we just think about the biologic action of the drug to one where we also consider the bigger picture of what the treatment experience is like for the patient, including their financial burden, investment of time, and side effects,” study coauthor Katherine E. Reeder-Hayes, MD, section chief of breast oncology at UNC, said in the press release.
The results demonstrate that therapeutic decisions in the endocrine-refractory or triple-negative metastatic setting “may prioritize costs without affecting clinical outcomes” and highlight the direct impact that a “high-quality, transparent, and accessible economic analysis” can have on patient care, Scott D. Ramsey, MD, PhD, of Fred Hutchinson Cancer Research Center, Seattle, and colleagues wrote in an accompanying editorial.
Following the treatment sequences outlined in this study would “reduce patient financial burden and save our health system hundreds of millions of dollars annually,” the editorialists wrote.
As for next steps, Dr. Wheeler and colleagues have developed a financial navigation program to help patients manage their out-of-pocket cancer care costs and are currently scaling up the intervention in nine rural and nonrural oncology practices across North Carolina.
The study was supported by the Center for Disease Control and Prevention through the Prevention Research Centers Program. Dr. Wheeler has received research funding and payment for travel, accommodations, and expenses from Pfizer. Dr. Ramsey has had consulting or advisory roles and has received research funding and/or payment for travel, accommodations, and expenses from Bayer, Genentech, AstraZeneca, Merck, GRAIL, Seattle Genetics, Biovica, and/or Flatiron Health. Because of their editorial roles at the journal, the Journal of Clinical Oncology recused Dr. Wheeler and Dr. Ramsey from having any role in the peer review of their respective manuscripts.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Racial disparities in preventive services use seen among patients with spina bifida or cerebral palsy
Black adults also had lower odds of having a bone density screening, compared with White adults. Plus, comorbidities were highest among the Black patients, according to the paper, which was published in Annals of Family Medicine.
Elham Mahmoudi, PhD, and her coauthors examined private insurance claims from 11,635 patients with cerebral palsy (CP) or spina bifida over ten years from 2007 to 2017. The researchers analyzed comorbidities and compared the rates of different psychological, cardiometabolic, and musculoskeletal conditions among these patients.
Only 23% of Hispanic participants and 18% of Black participants attended an annual wellness visit, compared with 32% of the White participants.
Only 1% of Black and 2% of White participants received any bone density screening (odds ratio = 0.54, 95% confidence interval [CI], 0.31-0.95), a service that is essential for catching a patient’s potential risk for osteoporosis and fractures.
According to the researchers, patients accessed services such as bone density scans, cholesterol assessments, diabetes screenings, and annual wellness visits less than recommended for people with those chronic conditions.
“People with spina bifida and cerebral palsy have complex care needs. We know through our work that chronic conditions are much higher among them compared with adults without disabilities,” Dr. Mahmoudi, associate professor in the department of family medicine at University of Michigan, Ann Arbor, said in an interview. “I was surprised to see even with private insurance, the rate of using preventative services is so low among White people and minority populations.”
Comorbidities highest in Black participants
Black adults had the highest comorbidity score of 2.5, and Hispanic adults had the lowest comorbidity score of 1.8. For White adults in the study, the comorbidity score was 2.0.
Osteoporosis, a common concern for people with spina bifida or cerebral palsy, was detected in around 4% of all participants. Osteoarthritis was detected in 13.38% of Black participants, versus 8.53% of Hispanic participants and 11.09% of White participants.
Diabetes and hypertension were more common among Black participants than among Hispanic and White participants. The percentages of Black patients with hypertension and diabetes were 16.5% and 39.89%, respectively. Among the Hispanic and White adults, the percentages with hypertension were 22.3% and 28.2%, respectively, according to the paper.
Disparities in access
Jamil Paden, racial and health equity manager at the Christopher and Dana Reeve Foundation, said getting access to literature, transportation, tables, chairs, weigh scales, and imaging equipment that accommodate the needs of people with disabilities are some of the biggest challenges for people with disabilities who are trying to receive care.

“It’s not a one size fits all, we have to recognize that if someone doesn’t see themselves in a particular place, then it makes it more challenging for them to feel comfortable speaking up and saying things about their health, which would prevent a person from saying something early on,” Mr. Paden said in an interview. “That particular issue will continue to grow and become more of a health risk, or health challenge down the line.”
Mr. Paden emphasized intersections between class, race, and circumstances which can, together, make health care less equitable for people with disabilities, especially in underserved communities and communities of color. He urged health care providers to distance their practices from a “one size fits all” approach to treatment and engage in their patients’ individual lives and communities.
“It’s not enough to just say, Hey, you have a disability. So let me treat your disability ... You have to recognize that although a patient may have a dire diagnosis, they also are a person of color, and they have to navigate different aspects of life from their counterparts,” he said.
Dr. Mahmoudi said patient and provider understanding of the disability is often lacking. She recommended advocating for patients, noting that giving both patients and providers the tools to further educate themselves and apply that to their regular visits is a good first step.
“Just having access to a facility doesn’t mean they will get the services they need. Preventative services that are recommended for people with disabilities differ from the general population. Providers should be educated about that and the patient needs to be educated about that,” she added.
“Patients who do not approach clinicians get lost in the system. Maybe many facilities are not disability friendly, or they need health literacy. If they don’t know they are at risk for osteoporosis, for example, then they won’t ask,” Dr. Mahmoudi said.
The study was funded by The National Institute on Disability, Independent Living, and Rehabilitation Research. Dr. Mahmoudi and Mr. Paden report no relevant financial relationships.
Black adults also had lower odds of having a bone density screening, compared with White adults. Plus, comorbidities were highest among the Black patients, according to the paper, which was published in Annals of Family Medicine.
Elham Mahmoudi, PhD, and her coauthors examined private insurance claims from 11,635 patients with cerebral palsy (CP) or spina bifida over ten years from 2007 to 2017. The researchers analyzed comorbidities and compared the rates of different psychological, cardiometabolic, and musculoskeletal conditions among these patients.
Only 23% of Hispanic participants and 18% of Black participants attended an annual wellness visit, compared with 32% of the White participants.
Only 1% of Black and 2% of White participants received any bone density screening (odds ratio = 0.54, 95% confidence interval [CI], 0.31-0.95), a service that is essential for catching a patient’s potential risk for osteoporosis and fractures.
According to the researchers, patients accessed services such as bone density scans, cholesterol assessments, diabetes screenings, and annual wellness visits less than recommended for people with those chronic conditions.
“People with spina bifida and cerebral palsy have complex care needs. We know through our work that chronic conditions are much higher among them compared with adults without disabilities,” Dr. Mahmoudi, associate professor in the department of family medicine at University of Michigan, Ann Arbor, said in an interview. “I was surprised to see even with private insurance, the rate of using preventative services is so low among White people and minority populations.”
Comorbidities highest in Black participants
Black adults had the highest comorbidity score of 2.5, and Hispanic adults had the lowest comorbidity score of 1.8. For White adults in the study, the comorbidity score was 2.0.
Osteoporosis, a common concern for people with spina bifida or cerebral palsy, was detected in around 4% of all participants. Osteoarthritis was detected in 13.38% of Black participants, versus 8.53% of Hispanic participants and 11.09% of White participants.
Diabetes and hypertension were more common among Black participants than among Hispanic and White participants. The percentages of Black patients with hypertension and diabetes were 16.5% and 39.89%, respectively. Among the Hispanic and White adults, the percentages with hypertension were 22.3% and 28.2%, respectively, according to the paper.
Disparities in access
Jamil Paden, racial and health equity manager at the Christopher and Dana Reeve Foundation, said getting access to literature, transportation, tables, chairs, weigh scales, and imaging equipment that accommodate the needs of people with disabilities are some of the biggest challenges for people with disabilities who are trying to receive care.
“It’s not a one size fits all, we have to recognize that if someone doesn’t see themselves in a particular place, then it makes it more challenging for them to feel comfortable speaking up and saying things about their health, which would prevent a person from saying something early on,” Mr. Paden said in an interview. “That particular issue will continue to grow and become more of a health risk, or health challenge down the line.”
Mr. Paden emphasized intersections between class, race, and circumstances which can, together, make health care less equitable for people with disabilities, especially in underserved communities and communities of color. He urged health care providers to distance their practices from a “one size fits all” approach to treatment and engage in their patients’ individual lives and communities.
“It’s not enough to just say, Hey, you have a disability. So let me treat your disability ... You have to recognize that although a patient may have a dire diagnosis, they also are a person of color, and they have to navigate different aspects of life from their counterparts,” he said.
Dr. Mahmoudi said patient and provider understanding of the disability is often lacking. She recommended advocating for patients, noting that giving both patients and providers the tools to further educate themselves and apply that to their regular visits is a good first step.
“Just having access to a facility doesn’t mean they will get the services they need. Preventative services that are recommended for people with disabilities differ from the general population. Providers should be educated about that and the patient needs to be educated about that,” she added.
“Patients who do not approach clinicians get lost in the system. Maybe many facilities are not disability friendly, or they need health literacy. If they don’t know they are at risk for osteoporosis, for example, then they won’t ask,” Dr. Mahmoudi said.
The study was funded by The National Institute on Disability, Independent Living, and Rehabilitation Research. Dr. Mahmoudi and Mr. Paden report no relevant financial relationships.
Black adults also had lower odds of having a bone density screening, compared with White adults. Plus, comorbidities were highest among the Black patients, according to the paper, which was published in Annals of Family Medicine.
Elham Mahmoudi, PhD, and her coauthors examined private insurance claims from 11,635 patients with cerebral palsy (CP) or spina bifida over ten years from 2007 to 2017. The researchers analyzed comorbidities and compared the rates of different psychological, cardiometabolic, and musculoskeletal conditions among these patients.
Only 23% of Hispanic participants and 18% of Black participants attended an annual wellness visit, compared with 32% of the White participants.
Only 1% of Black and 2% of White participants received any bone density screening (odds ratio = 0.54, 95% confidence interval [CI], 0.31-0.95), a service that is essential for catching a patient’s potential risk for osteoporosis and fractures.
According to the researchers, patients accessed services such as bone density scans, cholesterol assessments, diabetes screenings, and annual wellness visits less than recommended for people with those chronic conditions.
“People with spina bifida and cerebral palsy have complex care needs. We know through our work that chronic conditions are much higher among them compared with adults without disabilities,” Dr. Mahmoudi, associate professor in the department of family medicine at University of Michigan, Ann Arbor, said in an interview. “I was surprised to see even with private insurance, the rate of using preventative services is so low among White people and minority populations.”
Comorbidities highest in Black participants
Black adults had the highest comorbidity score of 2.5, and Hispanic adults had the lowest comorbidity score of 1.8. For White adults in the study, the comorbidity score was 2.0.
Osteoporosis, a common concern for people with spina bifida or cerebral palsy, was detected in around 4% of all participants. Osteoarthritis was detected in 13.38% of Black participants, versus 8.53% of Hispanic participants and 11.09% of White participants.
Diabetes and hypertension were more common among Black participants than among Hispanic and White participants. The percentages of Black patients with hypertension and diabetes were 16.5% and 39.89%, respectively. Among the Hispanic and White adults, the percentages with hypertension were 22.3% and 28.2%, respectively, according to the paper.
Disparities in access
Jamil Paden, racial and health equity manager at the Christopher and Dana Reeve Foundation, said getting access to literature, transportation, tables, chairs, weigh scales, and imaging equipment that accommodate the needs of people with disabilities are some of the biggest challenges for people with disabilities who are trying to receive care.
“It’s not a one size fits all, we have to recognize that if someone doesn’t see themselves in a particular place, then it makes it more challenging for them to feel comfortable speaking up and saying things about their health, which would prevent a person from saying something early on,” Mr. Paden said in an interview. “That particular issue will continue to grow and become more of a health risk, or health challenge down the line.”
Mr. Paden emphasized intersections between class, race, and circumstances which can, together, make health care less equitable for people with disabilities, especially in underserved communities and communities of color. He urged health care providers to distance their practices from a “one size fits all” approach to treatment and engage in their patients’ individual lives and communities.
“It’s not enough to just say, Hey, you have a disability. So let me treat your disability ... You have to recognize that although a patient may have a dire diagnosis, they also are a person of color, and they have to navigate different aspects of life from their counterparts,” he said.
Dr. Mahmoudi said patient and provider understanding of the disability is often lacking. She recommended advocating for patients, noting that giving both patients and providers the tools to further educate themselves and apply that to their regular visits is a good first step.
“Just having access to a facility doesn’t mean they will get the services they need. Preventative services that are recommended for people with disabilities differ from the general population. Providers should be educated about that and the patient needs to be educated about that,” she added.
“Patients who do not approach clinicians get lost in the system. Maybe many facilities are not disability friendly, or they need health literacy. If they don’t know they are at risk for osteoporosis, for example, then they won’t ask,” Dr. Mahmoudi said.
The study was funded by The National Institute on Disability, Independent Living, and Rehabilitation Research. Dr. Mahmoudi and Mr. Paden report no relevant financial relationships.
FROM ANNALS OF FAMILY MEDICINE
Hormones’ impact described in transgender rheumatology patients
Gender-affirming hormone therapy’s effect on transgender patients with rheumatic disease is unclear but does not appear to modulate its course and does not need to be strictly contraindicated in most patients, according to a case series and systematic literature review.
More doctors are practicing transgender medicine, yet a limited amount of information is available on rheumatic disease in transgender and gender diverse (TGGD) individuals, Kristen Mathias, MD, a rheumatology fellow at Johns Hopkins University, Baltimore, said in her presentation of the study at the Lancet Summit on Sex and Gender in Rheumatology.

“This is important, as it is well known that sex hormones affect the pathogenesis and expression of autoimmune diseases,” Dr. Mathias said. Knowing more about the effects of gender-affirming hormone therapy (GAHT) and gender-affirming surgery on disease activity in TGGD individuals could better inform decisions about care in this population.
Dr. Mathias and colleagues identified 7 transgender patients with rheumatic diseases from a pool of 1,053 patients seen at the Los Angeles County and University of Southern California Medical Center, Los Angeles, from June 2019 to June 2021. This included five transgender males and two transgender females. They ranged in age from 13 to 52 years.
All seven were on GAHT, and its impact on disease activity was considered “possible” in two of the seven patients.
In a systematic literature review, investigators found 11 studies that included 11 transgender women and 2 transgender men, ranging in age from 22 to 49 years. All the patients were on GAHT. In 12 of 13 patients, the hormones were considered possibly related to their rheumatic disease activity.
The 20 patients had diagnoses of rheumatoid arthritis, cutaneous and systemic lupus erythematosus, adult-onset Still disease, spondyloarthritis, myositis, and systemic sclerosis.
GAHT should not be a strict contraindication in these patients, based on these findings, Dr. Mathias noted. Information to clarify the effect of GAHT on rheumatic disease is sparse, however. Physicians should adopt a personalized, shared decision-making approach when consulting patients.
“During patient encounters, they should be screened for psychosocial barriers when appropriate,” Dr. Mathias recommended.
Findings could pave way for larger studies, more data
Studies on the impact and consequences of rheumatic disease in TGGD individuals are sorely lacking, said Vagishwari Murugesan, MBBS, a clinical fellow in rheumatology at the University of Toronto.
“While this is a small study of only seven patients and no conclusive results can be drawn, studies like these can help pave the way for larger multicentric studies, which can give us more definitive data on gender-affirming hormone therapy and its consequences on rheumatic diseases,” said Dr. Murugesan, who was not involved in the study.
A registry would be a great way to collaborate with other stakeholders interested in the same topic and conduct larger studies, she said. “I would recommend that not only do we screen for psychosocial barriers but also actively engage as a health care community in addressing how we can overcome the barriers for patients to access effective health care.”
No external funding was obtained for the study.
A version of this article first appeared on Medscape.com.
Gender-affirming hormone therapy’s effect on transgender patients with rheumatic disease is unclear but does not appear to modulate its course and does not need to be strictly contraindicated in most patients, according to a case series and systematic literature review.
More doctors are practicing transgender medicine, yet a limited amount of information is available on rheumatic disease in transgender and gender diverse (TGGD) individuals, Kristen Mathias, MD, a rheumatology fellow at Johns Hopkins University, Baltimore, said in her presentation of the study at the Lancet Summit on Sex and Gender in Rheumatology.
“This is important, as it is well known that sex hormones affect the pathogenesis and expression of autoimmune diseases,” Dr. Mathias said. Knowing more about the effects of gender-affirming hormone therapy (GAHT) and gender-affirming surgery on disease activity in TGGD individuals could better inform decisions about care in this population.
Dr. Mathias and colleagues identified 7 transgender patients with rheumatic diseases from a pool of 1,053 patients seen at the Los Angeles County and University of Southern California Medical Center, Los Angeles, from June 2019 to June 2021. This included five transgender males and two transgender females. They ranged in age from 13 to 52 years.
All seven were on GAHT, and its impact on disease activity was considered “possible” in two of the seven patients.
In a systematic literature review, investigators found 11 studies that included 11 transgender women and 2 transgender men, ranging in age from 22 to 49 years. All the patients were on GAHT. In 12 of 13 patients, the hormones were considered possibly related to their rheumatic disease activity.
The 20 patients had diagnoses of rheumatoid arthritis, cutaneous and systemic lupus erythematosus, adult-onset Still disease, spondyloarthritis, myositis, and systemic sclerosis.
GAHT should not be a strict contraindication in these patients, based on these findings, Dr. Mathias noted. Information to clarify the effect of GAHT on rheumatic disease is sparse, however. Physicians should adopt a personalized, shared decision-making approach when consulting patients.
“During patient encounters, they should be screened for psychosocial barriers when appropriate,” Dr. Mathias recommended.
Findings could pave way for larger studies, more data
Studies on the impact and consequences of rheumatic disease in TGGD individuals are sorely lacking, said Vagishwari Murugesan, MBBS, a clinical fellow in rheumatology at the University of Toronto.
“While this is a small study of only seven patients and no conclusive results can be drawn, studies like these can help pave the way for larger multicentric studies, which can give us more definitive data on gender-affirming hormone therapy and its consequences on rheumatic diseases,” said Dr. Murugesan, who was not involved in the study.
A registry would be a great way to collaborate with other stakeholders interested in the same topic and conduct larger studies, she said. “I would recommend that not only do we screen for psychosocial barriers but also actively engage as a health care community in addressing how we can overcome the barriers for patients to access effective health care.”
No external funding was obtained for the study.
A version of this article first appeared on Medscape.com.
Gender-affirming hormone therapy’s effect on transgender patients with rheumatic disease is unclear but does not appear to modulate its course and does not need to be strictly contraindicated in most patients, according to a case series and systematic literature review.
More doctors are practicing transgender medicine, yet a limited amount of information is available on rheumatic disease in transgender and gender diverse (TGGD) individuals, Kristen Mathias, MD, a rheumatology fellow at Johns Hopkins University, Baltimore, said in her presentation of the study at the Lancet Summit on Sex and Gender in Rheumatology.
“This is important, as it is well known that sex hormones affect the pathogenesis and expression of autoimmune diseases,” Dr. Mathias said. Knowing more about the effects of gender-affirming hormone therapy (GAHT) and gender-affirming surgery on disease activity in TGGD individuals could better inform decisions about care in this population.
Dr. Mathias and colleagues identified 7 transgender patients with rheumatic diseases from a pool of 1,053 patients seen at the Los Angeles County and University of Southern California Medical Center, Los Angeles, from June 2019 to June 2021. This included five transgender males and two transgender females. They ranged in age from 13 to 52 years.
All seven were on GAHT, and its impact on disease activity was considered “possible” in two of the seven patients.
In a systematic literature review, investigators found 11 studies that included 11 transgender women and 2 transgender men, ranging in age from 22 to 49 years. All the patients were on GAHT. In 12 of 13 patients, the hormones were considered possibly related to their rheumatic disease activity.
The 20 patients had diagnoses of rheumatoid arthritis, cutaneous and systemic lupus erythematosus, adult-onset Still disease, spondyloarthritis, myositis, and systemic sclerosis.
GAHT should not be a strict contraindication in these patients, based on these findings, Dr. Mathias noted. Information to clarify the effect of GAHT on rheumatic disease is sparse, however. Physicians should adopt a personalized, shared decision-making approach when consulting patients.
“During patient encounters, they should be screened for psychosocial barriers when appropriate,” Dr. Mathias recommended.
Findings could pave way for larger studies, more data
Studies on the impact and consequences of rheumatic disease in TGGD individuals are sorely lacking, said Vagishwari Murugesan, MBBS, a clinical fellow in rheumatology at the University of Toronto.
“While this is a small study of only seven patients and no conclusive results can be drawn, studies like these can help pave the way for larger multicentric studies, which can give us more definitive data on gender-affirming hormone therapy and its consequences on rheumatic diseases,” said Dr. Murugesan, who was not involved in the study.
A registry would be a great way to collaborate with other stakeholders interested in the same topic and conduct larger studies, she said. “I would recommend that not only do we screen for psychosocial barriers but also actively engage as a health care community in addressing how we can overcome the barriers for patients to access effective health care.”
No external funding was obtained for the study.
A version of this article first appeared on Medscape.com.
FROM THE LANCET SUMMIT ON SEX AND GENDER IN RHEUMATOLOGY
Alopecia areata: Positive results reported for two investigational JAK inhibitors
in separate studies reported at the annual congress of the European Academy of Dermatology and Venereology.
In the THRIVE-AA1 study, the primary endpoint of a Severity of Alopecia Tool (SALT) score of 20 or lower –which indicates that hair regrowth has occurred on at least 80% of the scalp – was achieved among patients taking deuruxolitinib, which was a significantly higher proportion than with placebo (P < .0001). Importantly, the JAK inhibitor’s effects were seen in as early as 4 weeks, and there was significant improvement in both eyelash and eyebrow hair regrowth.
In the unrelated ALLEGRO-LT study, effects from treatment with the JAK inhibitor ritlecitinib appeared to be sustained for 2 years; 69.6% of patients treated with ritlecitinib had a SALT score of 20 or lower by 24 months.
These data are “very exciting for alopecia areata because the patients selected are very severe,” observed Mahtab Samimi, MD, PhD, who cochaired the late-breaking session in which the study findings were discussed.
THRIVE-AA1 included only patients with hair loss of 50% or more. The ALLEGRO-LT study included patients with total scalp or total body hair loss (areata totalis/areata universalis) of 25%-50% at enrollment.
Moreover, “very stringent criteria” were used. SALT scores of 10 or less were evaluated in both studies, observed Dr. Samimi, professor of dermatology at the University of Tours (France).
“We can be ambitious now for our patients with alopecia areata; that’s really good news,” Dr. Samimi added.
Deuruxolitinib and the THRIVE trials
Deuruxolitinib is an oral JAK1/JAK2 inhibitor that has been tested in two similarly designed, multinational, randomized, double-blind, placebo-controlled phase 3 trials in patients with AA, THRIVE-AA1 and THRIVE-AA2.
Two doses of deuruxolitinib, 8 mg and 12 mg given twice daily, were evaluated in the trials, which altogether included just over 1,200 patients.
Results of THRIVE-AA1 have been reported by the manufacturer. Brett King, MD, PhD, associate professor of dermatology, Yale University, New Haven, Conn., presented a more comprehensive review at the EADV meeting.
He reported that at 24 weeks, SALT scores of 20 or lower were achieved by 30% of adults with AA who were treated with deuruxolitinib 8 mg and by 42% of those treated with deuruxolitinib 12 mg. This primary endpoint was seen in only 1% of the placebo-treated patients.
The more stringent endpoint of having a SALT score of 10 or less, which indicates that hair regrowth has occurred over 90% of the scalp, was met by 21% of patients who received deuruxolitinib 8 mg twice a day and by 35% of those who received the 12-mg dose twice a day at 24 weeks. This endpoint was not reached by any of the placebo-treated patients.
“This is truly transformative therapy,” Dr. King said when presenting the findings. “We know that the chances of spontaneous remission when you have severe disease is next to zero,” he added.
There were reasonably high rates of patient satisfaction with the treatment, according to Dr. King. He said that 42% of those who took 8 mg twice a day and 53% of those who took 12 mg twice a day said they were “very satisfied” or “satisfied” with the degree of scalp hair regrowth achieved, compared with 5% for placebo.
Safety was as expected, and there were no signs of any blood clots, said Dr. King. Common treatment-emergent adverse events (TEAEs) that affected 5% or more of patients included acne and headache. Serious TEAEs were reported by 1.1% and 0.5% of those taking the 8-mg and 12-mg twice-daily doses, respectively, compared with 2.9% of those who received placebo.
Overall, the results look promising for deuruxolitinib, he added. He noted that almost all patients included in the trial have opted to continue in the open-label long-term safety study.
Prescribing information of the JAK inhibitors approved by the U.S. Food and Drug Administration includes a boxed warning about risk of serious infections, mortality, malignancy, major adverse cardiovascular events (MACE), and thrombosis. The warning is based on experience with another JAK inhibitor for patients with rheumatoid arthritis.
Ritlecitinib and the ALLEGRO studies
Interim results of the ongoing, open-label, phase 3 ALLEGRO-LT study with ritlecitinib were presented separately by Athanasios Tsianakas, MD, head of the department of dermatology at Fachklinik Bad Bentheim, Germany.
Ritlecitinib, which targets JAK3 and also the TEC family of tyrosine kinases, had met all of its endpoints in the prior ALLEGRO Phase 2b/3 study, Dr. Tsianakas said. Those included the benchmarks of a SALT score of 20 or less and a SALT score of 10 or less.
“Ritlecitinib showed a very good long-term efficacy and good safety profile in our adolescent and adult patients suffering from alopecia areata,” said Dr. Tsianakas.
A total of 447 patients were included in the trial. They were treated with 50 mg of ritlecitinib every day; some had already participated in the ALLEGRO trial, while others had been newly recruited. The latter group entered the trial after a 4-week run-in period, during which a 200-mg daily loading dose was given for 4 weeks.
Most (86%) patients had been exposed to ritlecitinib for at least 12 months; one-fifth had discontinued treatment at the data cutoff, generally because the patients no longer met the eligibility criteria for the trial.
Safety was paramount, Dr. Tsianakas highlighted. There were few adverse events that led to temporary or permanent discontinuation of the study drug. The most common TEAEs that affected 5% or more of patients included headache and acne. There were two cases of MACE (one nonfatal myocardial infarction and one nonfatal stroke).
The proportion of patients with a SALT score of 20 or less was 2.5% at 1 month, 27.9% at 3 months, 50.1% at 6 months, 59.8% at 9 months, and 65.5% at 12 months. Thereafter, there was little shift in the response. A sustained effect, in which a SALT score of 20 or less was seen out to 24 months, occurred in 69.9% of patients.
A similar pattern was seen for SALT scores of 10 or less, ranging from 16.5% at 3 months to 62.5% at 24 months.
Following in baricitinib’s footsteps?
This not the first time that JAK inhibitors have been shown to have beneficial effects for patients with AA. Baricitinib (Olumiant) recently became the first JAK inhibitor to be granted marketing approval for AA in the United States, largely on the basis of two pivotal phase 3 studies, BRAVE-AA1 and BRAVE-AA2.
“This is just such an incredibly exciting time,” said Dr. King. “Our discoveries in the lab are being translated into effective therapies for patients with diseases for which we’ve not previously had therapies,” he commented.
“Our concept of interferon gamma– and interleukin-15–mediated disease is probably not true for everybody,” said, Dr. King, who acknowledged that some patients with AA do not respond to JAK-inhibitor therapy or may need additional or alternative treatment.
“It’s probably not that homogeneous a disease,” he added. “It’s fascinating that the very first drugs for this disease are showing efficacy in as many patients as they are.”
The THRIVE-AAI study was funded by CONCERT Pharmaceuticals. Dr. King has served on advisory boards, has provided consulting services to, or has been a trial investigator for multiple pharmaceutical companies, including CoNCERT Pharmaceuticals. The ALLEGRO-LT study was funded by Pfizer. Dr. Tsianakas has acted as a clinical trial investigator and speaker for Pfizer.
A version of this article first appeared on Medscape.com.
in separate studies reported at the annual congress of the European Academy of Dermatology and Venereology.
In the THRIVE-AA1 study, the primary endpoint of a Severity of Alopecia Tool (SALT) score of 20 or lower –which indicates that hair regrowth has occurred on at least 80% of the scalp – was achieved among patients taking deuruxolitinib, which was a significantly higher proportion than with placebo (P < .0001). Importantly, the JAK inhibitor’s effects were seen in as early as 4 weeks, and there was significant improvement in both eyelash and eyebrow hair regrowth.
In the unrelated ALLEGRO-LT study, effects from treatment with the JAK inhibitor ritlecitinib appeared to be sustained for 2 years; 69.6% of patients treated with ritlecitinib had a SALT score of 20 or lower by 24 months.
These data are “very exciting for alopecia areata because the patients selected are very severe,” observed Mahtab Samimi, MD, PhD, who cochaired the late-breaking session in which the study findings were discussed.
THRIVE-AA1 included only patients with hair loss of 50% or more. The ALLEGRO-LT study included patients with total scalp or total body hair loss (areata totalis/areata universalis) of 25%-50% at enrollment.
Moreover, “very stringent criteria” were used. SALT scores of 10 or less were evaluated in both studies, observed Dr. Samimi, professor of dermatology at the University of Tours (France).
“We can be ambitious now for our patients with alopecia areata; that’s really good news,” Dr. Samimi added.
Deuruxolitinib and the THRIVE trials
Deuruxolitinib is an oral JAK1/JAK2 inhibitor that has been tested in two similarly designed, multinational, randomized, double-blind, placebo-controlled phase 3 trials in patients with AA, THRIVE-AA1 and THRIVE-AA2.
Two doses of deuruxolitinib, 8 mg and 12 mg given twice daily, were evaluated in the trials, which altogether included just over 1,200 patients.
Results of THRIVE-AA1 have been reported by the manufacturer. Brett King, MD, PhD, associate professor of dermatology, Yale University, New Haven, Conn., presented a more comprehensive review at the EADV meeting.
He reported that at 24 weeks, SALT scores of 20 or lower were achieved by 30% of adults with AA who were treated with deuruxolitinib 8 mg and by 42% of those treated with deuruxolitinib 12 mg. This primary endpoint was seen in only 1% of the placebo-treated patients.
The more stringent endpoint of having a SALT score of 10 or less, which indicates that hair regrowth has occurred over 90% of the scalp, was met by 21% of patients who received deuruxolitinib 8 mg twice a day and by 35% of those who received the 12-mg dose twice a day at 24 weeks. This endpoint was not reached by any of the placebo-treated patients.
“This is truly transformative therapy,” Dr. King said when presenting the findings. “We know that the chances of spontaneous remission when you have severe disease is next to zero,” he added.
There were reasonably high rates of patient satisfaction with the treatment, according to Dr. King. He said that 42% of those who took 8 mg twice a day and 53% of those who took 12 mg twice a day said they were “very satisfied” or “satisfied” with the degree of scalp hair regrowth achieved, compared with 5% for placebo.
Safety was as expected, and there were no signs of any blood clots, said Dr. King. Common treatment-emergent adverse events (TEAEs) that affected 5% or more of patients included acne and headache. Serious TEAEs were reported by 1.1% and 0.5% of those taking the 8-mg and 12-mg twice-daily doses, respectively, compared with 2.9% of those who received placebo.
Overall, the results look promising for deuruxolitinib, he added. He noted that almost all patients included in the trial have opted to continue in the open-label long-term safety study.
Prescribing information of the JAK inhibitors approved by the U.S. Food and Drug Administration includes a boxed warning about risk of serious infections, mortality, malignancy, major adverse cardiovascular events (MACE), and thrombosis. The warning is based on experience with another JAK inhibitor for patients with rheumatoid arthritis.
Ritlecitinib and the ALLEGRO studies
Interim results of the ongoing, open-label, phase 3 ALLEGRO-LT study with ritlecitinib were presented separately by Athanasios Tsianakas, MD, head of the department of dermatology at Fachklinik Bad Bentheim, Germany.
Ritlecitinib, which targets JAK3 and also the TEC family of tyrosine kinases, had met all of its endpoints in the prior ALLEGRO Phase 2b/3 study, Dr. Tsianakas said. Those included the benchmarks of a SALT score of 20 or less and a SALT score of 10 or less.
“Ritlecitinib showed a very good long-term efficacy and good safety profile in our adolescent and adult patients suffering from alopecia areata,” said Dr. Tsianakas.
A total of 447 patients were included in the trial. They were treated with 50 mg of ritlecitinib every day; some had already participated in the ALLEGRO trial, while others had been newly recruited. The latter group entered the trial after a 4-week run-in period, during which a 200-mg daily loading dose was given for 4 weeks.
Most (86%) patients had been exposed to ritlecitinib for at least 12 months; one-fifth had discontinued treatment at the data cutoff, generally because the patients no longer met the eligibility criteria for the trial.
Safety was paramount, Dr. Tsianakas highlighted. There were few adverse events that led to temporary or permanent discontinuation of the study drug. The most common TEAEs that affected 5% or more of patients included headache and acne. There were two cases of MACE (one nonfatal myocardial infarction and one nonfatal stroke).
The proportion of patients with a SALT score of 20 or less was 2.5% at 1 month, 27.9% at 3 months, 50.1% at 6 months, 59.8% at 9 months, and 65.5% at 12 months. Thereafter, there was little shift in the response. A sustained effect, in which a SALT score of 20 or less was seen out to 24 months, occurred in 69.9% of patients.
A similar pattern was seen for SALT scores of 10 or less, ranging from 16.5% at 3 months to 62.5% at 24 months.
Following in baricitinib’s footsteps?
This not the first time that JAK inhibitors have been shown to have beneficial effects for patients with AA. Baricitinib (Olumiant) recently became the first JAK inhibitor to be granted marketing approval for AA in the United States, largely on the basis of two pivotal phase 3 studies, BRAVE-AA1 and BRAVE-AA2.
“This is just such an incredibly exciting time,” said Dr. King. “Our discoveries in the lab are being translated into effective therapies for patients with diseases for which we’ve not previously had therapies,” he commented.
“Our concept of interferon gamma– and interleukin-15–mediated disease is probably not true for everybody,” said, Dr. King, who acknowledged that some patients with AA do not respond to JAK-inhibitor therapy or may need additional or alternative treatment.
“It’s probably not that homogeneous a disease,” he added. “It’s fascinating that the very first drugs for this disease are showing efficacy in as many patients as they are.”
The THRIVE-AAI study was funded by CONCERT Pharmaceuticals. Dr. King has served on advisory boards, has provided consulting services to, or has been a trial investigator for multiple pharmaceutical companies, including CoNCERT Pharmaceuticals. The ALLEGRO-LT study was funded by Pfizer. Dr. Tsianakas has acted as a clinical trial investigator and speaker for Pfizer.
A version of this article first appeared on Medscape.com.
in separate studies reported at the annual congress of the European Academy of Dermatology and Venereology.
In the THRIVE-AA1 study, the primary endpoint of a Severity of Alopecia Tool (SALT) score of 20 or lower –which indicates that hair regrowth has occurred on at least 80% of the scalp – was achieved among patients taking deuruxolitinib, which was a significantly higher proportion than with placebo (P < .0001). Importantly, the JAK inhibitor’s effects were seen in as early as 4 weeks, and there was significant improvement in both eyelash and eyebrow hair regrowth.
In the unrelated ALLEGRO-LT study, effects from treatment with the JAK inhibitor ritlecitinib appeared to be sustained for 2 years; 69.6% of patients treated with ritlecitinib had a SALT score of 20 or lower by 24 months.
These data are “very exciting for alopecia areata because the patients selected are very severe,” observed Mahtab Samimi, MD, PhD, who cochaired the late-breaking session in which the study findings were discussed.
THRIVE-AA1 included only patients with hair loss of 50% or more. The ALLEGRO-LT study included patients with total scalp or total body hair loss (areata totalis/areata universalis) of 25%-50% at enrollment.
Moreover, “very stringent criteria” were used. SALT scores of 10 or less were evaluated in both studies, observed Dr. Samimi, professor of dermatology at the University of Tours (France).
“We can be ambitious now for our patients with alopecia areata; that’s really good news,” Dr. Samimi added.
Deuruxolitinib and the THRIVE trials
Deuruxolitinib is an oral JAK1/JAK2 inhibitor that has been tested in two similarly designed, multinational, randomized, double-blind, placebo-controlled phase 3 trials in patients with AA, THRIVE-AA1 and THRIVE-AA2.
Two doses of deuruxolitinib, 8 mg and 12 mg given twice daily, were evaluated in the trials, which altogether included just over 1,200 patients.
Results of THRIVE-AA1 have been reported by the manufacturer. Brett King, MD, PhD, associate professor of dermatology, Yale University, New Haven, Conn., presented a more comprehensive review at the EADV meeting.
He reported that at 24 weeks, SALT scores of 20 or lower were achieved by 30% of adults with AA who were treated with deuruxolitinib 8 mg and by 42% of those treated with deuruxolitinib 12 mg. This primary endpoint was seen in only 1% of the placebo-treated patients.
The more stringent endpoint of having a SALT score of 10 or less, which indicates that hair regrowth has occurred over 90% of the scalp, was met by 21% of patients who received deuruxolitinib 8 mg twice a day and by 35% of those who received the 12-mg dose twice a day at 24 weeks. This endpoint was not reached by any of the placebo-treated patients.
“This is truly transformative therapy,” Dr. King said when presenting the findings. “We know that the chances of spontaneous remission when you have severe disease is next to zero,” he added.
There were reasonably high rates of patient satisfaction with the treatment, according to Dr. King. He said that 42% of those who took 8 mg twice a day and 53% of those who took 12 mg twice a day said they were “very satisfied” or “satisfied” with the degree of scalp hair regrowth achieved, compared with 5% for placebo.
Safety was as expected, and there were no signs of any blood clots, said Dr. King. Common treatment-emergent adverse events (TEAEs) that affected 5% or more of patients included acne and headache. Serious TEAEs were reported by 1.1% and 0.5% of those taking the 8-mg and 12-mg twice-daily doses, respectively, compared with 2.9% of those who received placebo.
Overall, the results look promising for deuruxolitinib, he added. He noted that almost all patients included in the trial have opted to continue in the open-label long-term safety study.
Prescribing information of the JAK inhibitors approved by the U.S. Food and Drug Administration includes a boxed warning about risk of serious infections, mortality, malignancy, major adverse cardiovascular events (MACE), and thrombosis. The warning is based on experience with another JAK inhibitor for patients with rheumatoid arthritis.
Ritlecitinib and the ALLEGRO studies
Interim results of the ongoing, open-label, phase 3 ALLEGRO-LT study with ritlecitinib were presented separately by Athanasios Tsianakas, MD, head of the department of dermatology at Fachklinik Bad Bentheim, Germany.
Ritlecitinib, which targets JAK3 and also the TEC family of tyrosine kinases, had met all of its endpoints in the prior ALLEGRO Phase 2b/3 study, Dr. Tsianakas said. Those included the benchmarks of a SALT score of 20 or less and a SALT score of 10 or less.
“Ritlecitinib showed a very good long-term efficacy and good safety profile in our adolescent and adult patients suffering from alopecia areata,” said Dr. Tsianakas.
A total of 447 patients were included in the trial. They were treated with 50 mg of ritlecitinib every day; some had already participated in the ALLEGRO trial, while others had been newly recruited. The latter group entered the trial after a 4-week run-in period, during which a 200-mg daily loading dose was given for 4 weeks.
Most (86%) patients had been exposed to ritlecitinib for at least 12 months; one-fifth had discontinued treatment at the data cutoff, generally because the patients no longer met the eligibility criteria for the trial.
Safety was paramount, Dr. Tsianakas highlighted. There were few adverse events that led to temporary or permanent discontinuation of the study drug. The most common TEAEs that affected 5% or more of patients included headache and acne. There were two cases of MACE (one nonfatal myocardial infarction and one nonfatal stroke).
The proportion of patients with a SALT score of 20 or less was 2.5% at 1 month, 27.9% at 3 months, 50.1% at 6 months, 59.8% at 9 months, and 65.5% at 12 months. Thereafter, there was little shift in the response. A sustained effect, in which a SALT score of 20 or less was seen out to 24 months, occurred in 69.9% of patients.
A similar pattern was seen for SALT scores of 10 or less, ranging from 16.5% at 3 months to 62.5% at 24 months.
Following in baricitinib’s footsteps?
This not the first time that JAK inhibitors have been shown to have beneficial effects for patients with AA. Baricitinib (Olumiant) recently became the first JAK inhibitor to be granted marketing approval for AA in the United States, largely on the basis of two pivotal phase 3 studies, BRAVE-AA1 and BRAVE-AA2.
“This is just such an incredibly exciting time,” said Dr. King. “Our discoveries in the lab are being translated into effective therapies for patients with diseases for which we’ve not previously had therapies,” he commented.
“Our concept of interferon gamma– and interleukin-15–mediated disease is probably not true for everybody,” said, Dr. King, who acknowledged that some patients with AA do not respond to JAK-inhibitor therapy or may need additional or alternative treatment.
“It’s probably not that homogeneous a disease,” he added. “It’s fascinating that the very first drugs for this disease are showing efficacy in as many patients as they are.”
The THRIVE-AAI study was funded by CONCERT Pharmaceuticals. Dr. King has served on advisory boards, has provided consulting services to, or has been a trial investigator for multiple pharmaceutical companies, including CoNCERT Pharmaceuticals. The ALLEGRO-LT study was funded by Pfizer. Dr. Tsianakas has acted as a clinical trial investigator and speaker for Pfizer.
A version of this article first appeared on Medscape.com.
FROM THE EADV CONGRESS
Training program linked to less hand eczema for hairdressers
The study was conducted in Denmark, where about 40% of hairdressers develop occupational hand eczema (OHE), according to researchers. Hairdressers globally are exposed to wet work and myriad skin irritants and allergens, including dyes, permanent-wave solutions, persulfates, preservatives, and fragrances. The study, which was funded by the Danish hairdressers and beauticians union, was published in Contact Dermatitis.
Lead author Martin Havmose, BSc, of the National Allergy Research Center, department of dermatology and allergy, University of Copenhagen, Hellerup, Denmark, and colleagues wrote that prevention is critical, inasmuch as eczema can cut careers short and have lasting health effects.
Up to 70% of hairdressers experience some sort of work-related skin damage in their careers, as reported by this news organization.
Hand eczema also is common among hairdressers in the United States, Mark Denis Davis, MD, chair of dermatology at the Mayo Clinic in Rochester, Minn., told this news organization. It can be quite debilitating, itchy, and painful, he said.
“Often it is associated with painful fissuring, cracks in the skin, particularly involving the fingers. It may also be unsightly,” he said.
Dr. Davis said he hears anecdotally in his practice that many hairdressers are reluctant to wear gloves because of the touch and dexterity needed in their work.
The researchers evaluated the risk of OHE and compliance with skin protection measures among hairdressers who were trained before Denmark rolled out a nationwide skin protection program in hairdressing vocational schools in 2011.
Questionnaires were sent in May 2009 to all hairdressers (96.4% women; average age, 26) who had graduated from 1985 to 2007; in May 2020, questionnaires were sent to all hairdressers who had graduated from 2008 to 2018.
The average time worked in the trade was 8 years, and 28.8% no longer worked as hairdressers, data show.
The response rate was 66.6% (305/460) for the 2009 survey and 29.9% (363/1215) for the 2020 survey.
Prevalence of OHE dropped after program
The prevalence of OHE during career time dropped from 42.8% to 29% (adjusted odds ratio, 0.55; 95% confidence interval [CI], 0.40-0.77) between the two surveys.
In addition, the incidence rate of OHE decreased from 57.5 (95% CI, 48.4-68.4) to 42.0 (95% CI, 34.6-50.9) per 1,000 person-years (incidence rate ratio, 0.73; 95% CI, 0.560.95) in that period.
There was an increase in the use of gloves between the two surveys. There was more glove use when the hairdressers engaged in wet work and handled dyes, products with bleach, and permanent-wave solutions (P < .05).
The nationwide program educates hairdressing apprentices on contact allergy/urticaria, how to prevent occupational skin disease, and skin biology. Teaching materials focus on 11 recommendations, 7 of which are related to glove use.
“The lack of primary prevention of OHE in hairdressing vocational schools may be a missed opportunity in the prevention of the disease,” the authors concluded.
Dr. Davis said hairdressers with hand eczema should know that in the short term, topical corticosteroids can be used to decrease the inflammation of the skin.
He highlighted the following advice from the authors:
- Gloves should be used when washing, dyeing, bleaching, and creating perms.
- Disposable gloves should never be reused.
- Gloves should be used only as long as necessary.
- Rings should not be worn at work.
- Cotton gloves should be worn underneath protective gloves.
- For clients who are having their hair both cut and dyed, the hair should be cut before it is dyed.
- Nitrile gloves should be used without rubber accelerators.
“In the longer term,” said Dr. Davis, “the most important thing is to avoid exposure to the precipitating factors, such as wet work – working with water, which irritates the skin – and avoiding any allergens that are contributing to the eczema.”
The study was funded by an unrestricted grant from the Danish hairdressers and beauticians union. Two coauthors have links to industry, as listed in the original article. Dr. Davis reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study was conducted in Denmark, where about 40% of hairdressers develop occupational hand eczema (OHE), according to researchers. Hairdressers globally are exposed to wet work and myriad skin irritants and allergens, including dyes, permanent-wave solutions, persulfates, preservatives, and fragrances. The study, which was funded by the Danish hairdressers and beauticians union, was published in Contact Dermatitis.
Lead author Martin Havmose, BSc, of the National Allergy Research Center, department of dermatology and allergy, University of Copenhagen, Hellerup, Denmark, and colleagues wrote that prevention is critical, inasmuch as eczema can cut careers short and have lasting health effects.
Up to 70% of hairdressers experience some sort of work-related skin damage in their careers, as reported by this news organization.
Hand eczema also is common among hairdressers in the United States, Mark Denis Davis, MD, chair of dermatology at the Mayo Clinic in Rochester, Minn., told this news organization. It can be quite debilitating, itchy, and painful, he said.
“Often it is associated with painful fissuring, cracks in the skin, particularly involving the fingers. It may also be unsightly,” he said.
Dr. Davis said he hears anecdotally in his practice that many hairdressers are reluctant to wear gloves because of the touch and dexterity needed in their work.
The researchers evaluated the risk of OHE and compliance with skin protection measures among hairdressers who were trained before Denmark rolled out a nationwide skin protection program in hairdressing vocational schools in 2011.
Questionnaires were sent in May 2009 to all hairdressers (96.4% women; average age, 26) who had graduated from 1985 to 2007; in May 2020, questionnaires were sent to all hairdressers who had graduated from 2008 to 2018.
The average time worked in the trade was 8 years, and 28.8% no longer worked as hairdressers, data show.
The response rate was 66.6% (305/460) for the 2009 survey and 29.9% (363/1215) for the 2020 survey.
Prevalence of OHE dropped after program
The prevalence of OHE during career time dropped from 42.8% to 29% (adjusted odds ratio, 0.55; 95% confidence interval [CI], 0.40-0.77) between the two surveys.
In addition, the incidence rate of OHE decreased from 57.5 (95% CI, 48.4-68.4) to 42.0 (95% CI, 34.6-50.9) per 1,000 person-years (incidence rate ratio, 0.73; 95% CI, 0.560.95) in that period.
There was an increase in the use of gloves between the two surveys. There was more glove use when the hairdressers engaged in wet work and handled dyes, products with bleach, and permanent-wave solutions (P < .05).
The nationwide program educates hairdressing apprentices on contact allergy/urticaria, how to prevent occupational skin disease, and skin biology. Teaching materials focus on 11 recommendations, 7 of which are related to glove use.
“The lack of primary prevention of OHE in hairdressing vocational schools may be a missed opportunity in the prevention of the disease,” the authors concluded.
Dr. Davis said hairdressers with hand eczema should know that in the short term, topical corticosteroids can be used to decrease the inflammation of the skin.
He highlighted the following advice from the authors:
- Gloves should be used when washing, dyeing, bleaching, and creating perms.
- Disposable gloves should never be reused.
- Gloves should be used only as long as necessary.
- Rings should not be worn at work.
- Cotton gloves should be worn underneath protective gloves.
- For clients who are having their hair both cut and dyed, the hair should be cut before it is dyed.
- Nitrile gloves should be used without rubber accelerators.
“In the longer term,” said Dr. Davis, “the most important thing is to avoid exposure to the precipitating factors, such as wet work – working with water, which irritates the skin – and avoiding any allergens that are contributing to the eczema.”
The study was funded by an unrestricted grant from the Danish hairdressers and beauticians union. Two coauthors have links to industry, as listed in the original article. Dr. Davis reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study was conducted in Denmark, where about 40% of hairdressers develop occupational hand eczema (OHE), according to researchers. Hairdressers globally are exposed to wet work and myriad skin irritants and allergens, including dyes, permanent-wave solutions, persulfates, preservatives, and fragrances. The study, which was funded by the Danish hairdressers and beauticians union, was published in Contact Dermatitis.
Lead author Martin Havmose, BSc, of the National Allergy Research Center, department of dermatology and allergy, University of Copenhagen, Hellerup, Denmark, and colleagues wrote that prevention is critical, inasmuch as eczema can cut careers short and have lasting health effects.
Up to 70% of hairdressers experience some sort of work-related skin damage in their careers, as reported by this news organization.
Hand eczema also is common among hairdressers in the United States, Mark Denis Davis, MD, chair of dermatology at the Mayo Clinic in Rochester, Minn., told this news organization. It can be quite debilitating, itchy, and painful, he said.
“Often it is associated with painful fissuring, cracks in the skin, particularly involving the fingers. It may also be unsightly,” he said.
Dr. Davis said he hears anecdotally in his practice that many hairdressers are reluctant to wear gloves because of the touch and dexterity needed in their work.
The researchers evaluated the risk of OHE and compliance with skin protection measures among hairdressers who were trained before Denmark rolled out a nationwide skin protection program in hairdressing vocational schools in 2011.
Questionnaires were sent in May 2009 to all hairdressers (96.4% women; average age, 26) who had graduated from 1985 to 2007; in May 2020, questionnaires were sent to all hairdressers who had graduated from 2008 to 2018.
The average time worked in the trade was 8 years, and 28.8% no longer worked as hairdressers, data show.
The response rate was 66.6% (305/460) for the 2009 survey and 29.9% (363/1215) for the 2020 survey.
Prevalence of OHE dropped after program
The prevalence of OHE during career time dropped from 42.8% to 29% (adjusted odds ratio, 0.55; 95% confidence interval [CI], 0.40-0.77) between the two surveys.
In addition, the incidence rate of OHE decreased from 57.5 (95% CI, 48.4-68.4) to 42.0 (95% CI, 34.6-50.9) per 1,000 person-years (incidence rate ratio, 0.73; 95% CI, 0.560.95) in that period.
There was an increase in the use of gloves between the two surveys. There was more glove use when the hairdressers engaged in wet work and handled dyes, products with bleach, and permanent-wave solutions (P < .05).
The nationwide program educates hairdressing apprentices on contact allergy/urticaria, how to prevent occupational skin disease, and skin biology. Teaching materials focus on 11 recommendations, 7 of which are related to glove use.
“The lack of primary prevention of OHE in hairdressing vocational schools may be a missed opportunity in the prevention of the disease,” the authors concluded.
Dr. Davis said hairdressers with hand eczema should know that in the short term, topical corticosteroids can be used to decrease the inflammation of the skin.
He highlighted the following advice from the authors:
- Gloves should be used when washing, dyeing, bleaching, and creating perms.
- Disposable gloves should never be reused.
- Gloves should be used only as long as necessary.
- Rings should not be worn at work.
- Cotton gloves should be worn underneath protective gloves.
- For clients who are having their hair both cut and dyed, the hair should be cut before it is dyed.
- Nitrile gloves should be used without rubber accelerators.
“In the longer term,” said Dr. Davis, “the most important thing is to avoid exposure to the precipitating factors, such as wet work – working with water, which irritates the skin – and avoiding any allergens that are contributing to the eczema.”
The study was funded by an unrestricted grant from the Danish hairdressers and beauticians union. Two coauthors have links to industry, as listed in the original article. Dr. Davis reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CONTACT DERMATITIS
Study identifies skin biomarkers that predict newborn eczema risk
It might be possible to develop a simple test to identify newborn children who are at risk of later developing atopic dermatitis (AD), according to findings from a Danish prospective birth cohort study.
but also for having more severe disease.
“We are able to identify predictive immune biomarkers of atopic dermatitis using a noninvasive method that was not associated with any pain,” one of the study’s investigators, Anne-Sofie Halling, MD, said at a press briefing at the annual congress of the European Academy of Dermatology and Venereology.
“Importantly, we were able to predict atopic dermatitis occurring months after [sample] collection,” said Dr. Halling, who works at Bispebjerg Hospital and is a PhD student at the University of Copenhagen.
These findings could hopefully be used to help identify children “so that preventive strategies can target these children ... and decrease the incidence of this common disease,” she added.
AD is caused “by a complex interplay between skin barrier dysfunction and immune dysregulation,” Dr. Halling said, and it is “the first step in the so-called atopic march, where children also develop food allergy, asthma, and rhinitis.” Almost all cases of AD begin during the first years of life. Approximately 15%-20% of children can be affected, she noted, emphasizing the high burden of the disease and pointing out that strategies are shifting toward trying to prevent the disease in those at risk.
Copenhagen BABY cohort
This is where the BABY study comes in, Dr. Halling said. The study enrolled 450 children at birth and followed them until age 2 years. Gene mutation testing was performed at enrollment. All children underwent skin examination, and skin samples were taken using tape strips. Tape strips were applied to the back of the hand of children born at term and between the shoulder blades on the back of children who were premature.
Skin examinations were repeated, and skin samples were obtained again at age 2 months. They were taken again only if there were any signs of AD. For those diagnosed with AD, disease severity was assessed using the Eczema Area and Severity Index (EASI) by the treating physician. Children were excluded if they had AD at the time the tape strip testing was due to be performed.
Comparing term and preterm children
Dr. Halling noted that analyses were performed separately for the 300 children born at term and for the 150 who were preterm.
The prevalence of AD was higher among children born at term than among the preterm children (34.6% vs. 21.2%), and the median time to onset was shorter (6 months vs. 8 months). There were also differences in the EASI scores among those who developed AD; median scores were higher in the children born at term than in the preterm children (4.1 vs. 1.6).
More children born at term than preterm children had moderate to severe AD (23.3% vs. 8%), Dr. Halling reported.
TARC, IL-8, and IL-18 predictive of AD
Multiple immune biomarkers were tested, including various cytokines and filaggrin degradation products. On examination of skin samples collected at birth, no particular biomarkers were found at higher levels among children who developed AD in comparison with those who did not develop AD.
With regard to biomarkers examined in skin samples at 2 months of age, however, the results were different, Dr. Halling said. One particular cytokine, thymus and activation-regulated chemokine (TARC), was seen to double the risk of AD in the first 2 years of a child’s life.
This doubled risk was seen not only among the children born at term but also among those born preterm, although the data were only significant with regard to the children born at term.
The unadjusted hazard ratios and adjusted HRs (adjusted for parental atopy and filaggrin gene mutations) in term children were 2.11 (95% confidence interval, 1.36-3.26; P = .0008) and 1.85 (95% CI, 1.18-2.89; P = .007), respectively.
For preterm children, the HRs were 2.23 (95% CI, 0.85-5.86; P = .1) and 2.60 (95% CI, 0.98-6.85; P =.05), respectively.
These findings were in line with findings of other studies, Dr. Halling said. “It is well recognized that TARC is currently the best biomarker in patients with established atopic dermatitis.” Moreover, she reported that TARC was associated with a cumulative increase in the risk for AD and that levels were found to be higher in children in whom onset occurred at a later age than among those diagnosed before 6 months of age.
“This is important, as these findings shows that TARC levels predict atopic dermatitis that occurred many months later,” Dr. Halling said.
And, in term-born children at least, TARC upped the chances that the severity of AD would be greater than had it not been present (adjusted HR, 4.65; 95% CI, 1.91-11.31; P = .0007).
Increased levels of interleukin-8 (IL-8) and IL-18 at 2 months of age were also found to be predictive of having moderate to severe AD. The risk was more than double in comparison with those in whom levels were not increased, again only in term-born children.
‘Stimulating and interesting findings’
These data are “very stimulating and interesting,” Dedee Murrell, MD, professor and head of the department of dermatology at St. George Hospital, University of New South Wales, Sydney, observed at the press briefing.
“You found this significant association mainly in the newborn children born at term, and the association in the preterm babies wasn’t as high. Is that anything to do with how they were taken care of in the hospital?” Dr. Murrell asked.
“That’s a really good question,” Dr. Halling said. “Maybe they need to be exposed for a month or two before we are actually able to identify which children will develop atopic dermatitis.”
The study was funded by the Lundbeck Foundation. Dr. Halling has acted as a consultant for Coloplast and as a speaker for Leo Pharma. Dr. Murrell has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It might be possible to develop a simple test to identify newborn children who are at risk of later developing atopic dermatitis (AD), according to findings from a Danish prospective birth cohort study.
but also for having more severe disease.
“We are able to identify predictive immune biomarkers of atopic dermatitis using a noninvasive method that was not associated with any pain,” one of the study’s investigators, Anne-Sofie Halling, MD, said at a press briefing at the annual congress of the European Academy of Dermatology and Venereology.
“Importantly, we were able to predict atopic dermatitis occurring months after [sample] collection,” said Dr. Halling, who works at Bispebjerg Hospital and is a PhD student at the University of Copenhagen.
These findings could hopefully be used to help identify children “so that preventive strategies can target these children ... and decrease the incidence of this common disease,” she added.
AD is caused “by a complex interplay between skin barrier dysfunction and immune dysregulation,” Dr. Halling said, and it is “the first step in the so-called atopic march, where children also develop food allergy, asthma, and rhinitis.” Almost all cases of AD begin during the first years of life. Approximately 15%-20% of children can be affected, she noted, emphasizing the high burden of the disease and pointing out that strategies are shifting toward trying to prevent the disease in those at risk.
Copenhagen BABY cohort
This is where the BABY study comes in, Dr. Halling said. The study enrolled 450 children at birth and followed them until age 2 years. Gene mutation testing was performed at enrollment. All children underwent skin examination, and skin samples were taken using tape strips. Tape strips were applied to the back of the hand of children born at term and between the shoulder blades on the back of children who were premature.
Skin examinations were repeated, and skin samples were obtained again at age 2 months. They were taken again only if there were any signs of AD. For those diagnosed with AD, disease severity was assessed using the Eczema Area and Severity Index (EASI) by the treating physician. Children were excluded if they had AD at the time the tape strip testing was due to be performed.
Comparing term and preterm children
Dr. Halling noted that analyses were performed separately for the 300 children born at term and for the 150 who were preterm.
The prevalence of AD was higher among children born at term than among the preterm children (34.6% vs. 21.2%), and the median time to onset was shorter (6 months vs. 8 months). There were also differences in the EASI scores among those who developed AD; median scores were higher in the children born at term than in the preterm children (4.1 vs. 1.6).
More children born at term than preterm children had moderate to severe AD (23.3% vs. 8%), Dr. Halling reported.
TARC, IL-8, and IL-18 predictive of AD
Multiple immune biomarkers were tested, including various cytokines and filaggrin degradation products. On examination of skin samples collected at birth, no particular biomarkers were found at higher levels among children who developed AD in comparison with those who did not develop AD.
With regard to biomarkers examined in skin samples at 2 months of age, however, the results were different, Dr. Halling said. One particular cytokine, thymus and activation-regulated chemokine (TARC), was seen to double the risk of AD in the first 2 years of a child’s life.
This doubled risk was seen not only among the children born at term but also among those born preterm, although the data were only significant with regard to the children born at term.
The unadjusted hazard ratios and adjusted HRs (adjusted for parental atopy and filaggrin gene mutations) in term children were 2.11 (95% confidence interval, 1.36-3.26; P = .0008) and 1.85 (95% CI, 1.18-2.89; P = .007), respectively.
For preterm children, the HRs were 2.23 (95% CI, 0.85-5.86; P = .1) and 2.60 (95% CI, 0.98-6.85; P =.05), respectively.
These findings were in line with findings of other studies, Dr. Halling said. “It is well recognized that TARC is currently the best biomarker in patients with established atopic dermatitis.” Moreover, she reported that TARC was associated with a cumulative increase in the risk for AD and that levels were found to be higher in children in whom onset occurred at a later age than among those diagnosed before 6 months of age.
“This is important, as these findings shows that TARC levels predict atopic dermatitis that occurred many months later,” Dr. Halling said.
And, in term-born children at least, TARC upped the chances that the severity of AD would be greater than had it not been present (adjusted HR, 4.65; 95% CI, 1.91-11.31; P = .0007).
Increased levels of interleukin-8 (IL-8) and IL-18 at 2 months of age were also found to be predictive of having moderate to severe AD. The risk was more than double in comparison with those in whom levels were not increased, again only in term-born children.
‘Stimulating and interesting findings’
These data are “very stimulating and interesting,” Dedee Murrell, MD, professor and head of the department of dermatology at St. George Hospital, University of New South Wales, Sydney, observed at the press briefing.
“You found this significant association mainly in the newborn children born at term, and the association in the preterm babies wasn’t as high. Is that anything to do with how they were taken care of in the hospital?” Dr. Murrell asked.
“That’s a really good question,” Dr. Halling said. “Maybe they need to be exposed for a month or two before we are actually able to identify which children will develop atopic dermatitis.”
The study was funded by the Lundbeck Foundation. Dr. Halling has acted as a consultant for Coloplast and as a speaker for Leo Pharma. Dr. Murrell has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It might be possible to develop a simple test to identify newborn children who are at risk of later developing atopic dermatitis (AD), according to findings from a Danish prospective birth cohort study.
but also for having more severe disease.
“We are able to identify predictive immune biomarkers of atopic dermatitis using a noninvasive method that was not associated with any pain,” one of the study’s investigators, Anne-Sofie Halling, MD, said at a press briefing at the annual congress of the European Academy of Dermatology and Venereology.
“Importantly, we were able to predict atopic dermatitis occurring months after [sample] collection,” said Dr. Halling, who works at Bispebjerg Hospital and is a PhD student at the University of Copenhagen.
These findings could hopefully be used to help identify children “so that preventive strategies can target these children ... and decrease the incidence of this common disease,” she added.
AD is caused “by a complex interplay between skin barrier dysfunction and immune dysregulation,” Dr. Halling said, and it is “the first step in the so-called atopic march, where children also develop food allergy, asthma, and rhinitis.” Almost all cases of AD begin during the first years of life. Approximately 15%-20% of children can be affected, she noted, emphasizing the high burden of the disease and pointing out that strategies are shifting toward trying to prevent the disease in those at risk.
Copenhagen BABY cohort
This is where the BABY study comes in, Dr. Halling said. The study enrolled 450 children at birth and followed them until age 2 years. Gene mutation testing was performed at enrollment. All children underwent skin examination, and skin samples were taken using tape strips. Tape strips were applied to the back of the hand of children born at term and between the shoulder blades on the back of children who were premature.
Skin examinations were repeated, and skin samples were obtained again at age 2 months. They were taken again only if there were any signs of AD. For those diagnosed with AD, disease severity was assessed using the Eczema Area and Severity Index (EASI) by the treating physician. Children were excluded if they had AD at the time the tape strip testing was due to be performed.
Comparing term and preterm children
Dr. Halling noted that analyses were performed separately for the 300 children born at term and for the 150 who were preterm.
The prevalence of AD was higher among children born at term than among the preterm children (34.6% vs. 21.2%), and the median time to onset was shorter (6 months vs. 8 months). There were also differences in the EASI scores among those who developed AD; median scores were higher in the children born at term than in the preterm children (4.1 vs. 1.6).
More children born at term than preterm children had moderate to severe AD (23.3% vs. 8%), Dr. Halling reported.
TARC, IL-8, and IL-18 predictive of AD
Multiple immune biomarkers were tested, including various cytokines and filaggrin degradation products. On examination of skin samples collected at birth, no particular biomarkers were found at higher levels among children who developed AD in comparison with those who did not develop AD.
With regard to biomarkers examined in skin samples at 2 months of age, however, the results were different, Dr. Halling said. One particular cytokine, thymus and activation-regulated chemokine (TARC), was seen to double the risk of AD in the first 2 years of a child’s life.
This doubled risk was seen not only among the children born at term but also among those born preterm, although the data were only significant with regard to the children born at term.
The unadjusted hazard ratios and adjusted HRs (adjusted for parental atopy and filaggrin gene mutations) in term children were 2.11 (95% confidence interval, 1.36-3.26; P = .0008) and 1.85 (95% CI, 1.18-2.89; P = .007), respectively.
For preterm children, the HRs were 2.23 (95% CI, 0.85-5.86; P = .1) and 2.60 (95% CI, 0.98-6.85; P =.05), respectively.
These findings were in line with findings of other studies, Dr. Halling said. “It is well recognized that TARC is currently the best biomarker in patients with established atopic dermatitis.” Moreover, she reported that TARC was associated with a cumulative increase in the risk for AD and that levels were found to be higher in children in whom onset occurred at a later age than among those diagnosed before 6 months of age.
“This is important, as these findings shows that TARC levels predict atopic dermatitis that occurred many months later,” Dr. Halling said.
And, in term-born children at least, TARC upped the chances that the severity of AD would be greater than had it not been present (adjusted HR, 4.65; 95% CI, 1.91-11.31; P = .0007).
Increased levels of interleukin-8 (IL-8) and IL-18 at 2 months of age were also found to be predictive of having moderate to severe AD. The risk was more than double in comparison with those in whom levels were not increased, again only in term-born children.
‘Stimulating and interesting findings’
These data are “very stimulating and interesting,” Dedee Murrell, MD, professor and head of the department of dermatology at St. George Hospital, University of New South Wales, Sydney, observed at the press briefing.
“You found this significant association mainly in the newborn children born at term, and the association in the preterm babies wasn’t as high. Is that anything to do with how they were taken care of in the hospital?” Dr. Murrell asked.
“That’s a really good question,” Dr. Halling said. “Maybe they need to be exposed for a month or two before we are actually able to identify which children will develop atopic dermatitis.”
The study was funded by the Lundbeck Foundation. Dr. Halling has acted as a consultant for Coloplast and as a speaker for Leo Pharma. Dr. Murrell has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE EADV CONGRESS
Ezetimibe-statin combo lowers liver fat in open-label trial
Ezetimibe given in combination with rosuvastatin has a beneficial effect on liver fat in people with nonalcoholic fatty liver disease (NAFLD), according results of a randomized, active-controlled trial.
The findings, which come from the investigator-initiated ESSENTIAL trial, are likely to add to the debate over whether or not the lipid-lowering combination could be of benefit beyond its effects in the blood.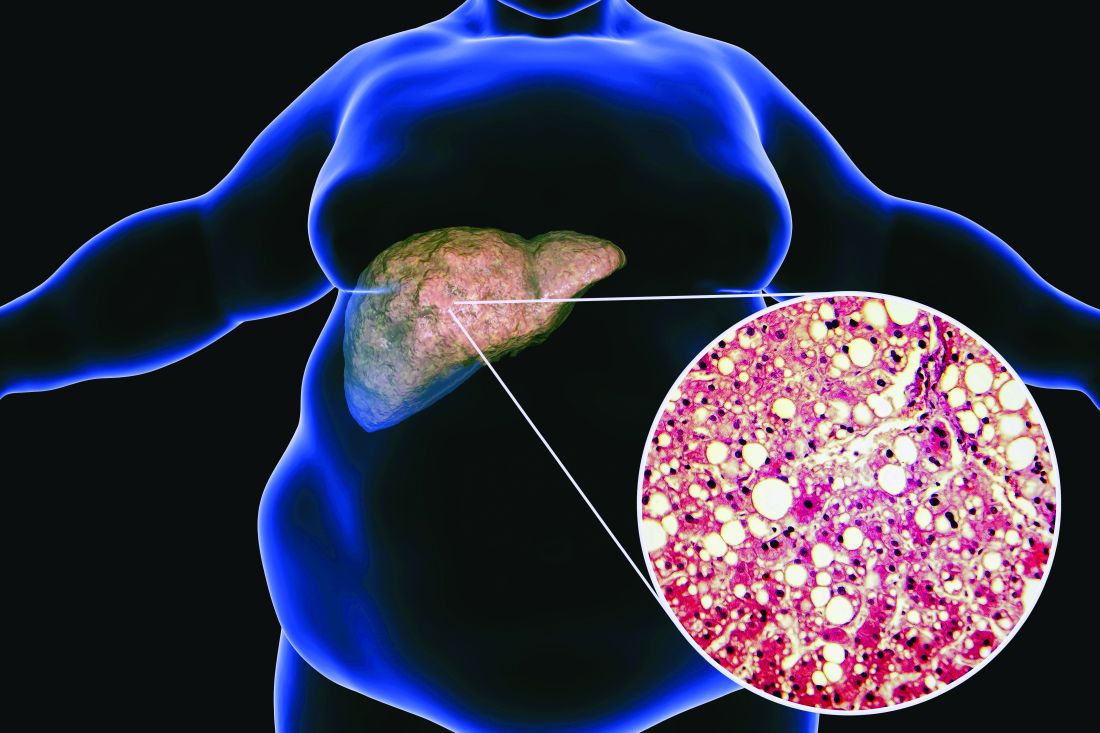
“We used magnetic resonance imaging-derived proton density fat fraction [MRI-PDFF], which is highly reliable method of assessing hepatic steatosis,” Youngjoon Kim, PhD, one of the study investigators, said at the annual meeting of the European Association for the Study of Diabetes in Barcelona.
“It enables accurate, repeatable and reproducible quantitative assessment of liver fat over the entire liver,” observed Dr. Kim, who works at Severance Hospital, part of Yonsei University in Seoul.
He reported that there was a significant 5.8% decrease in liver fat following 24 weeks’ treatment with ezetimibe and rosuvastatin comparing baseline with end of treatment MRI-PDFF values; a drop that was significant (18.2% vs. 12.3%, P < .001).
Rosuvastatin monotherapy also reduced liver fat from 15.0% at baseline to 12.4% after 24 weeks; this drop of 2.6% was also significant (P = .003).
This gave an absolute mean difference between the two study arms of 3.2% (P = .02).
Rationale for the ESSENTIAL study
Dr. Kim observed during his presentation that NAFLD is burgeoning problem around the world. Ezetimibe plus rosuvastatin was a combination treatment already used widely in clinical practice, and there had been some suggestion that ezetimibe might have an effect on liver fat.
“Although the effect of ezetimibe on hepatic steatosis is still controversial, ezetimibe has been reported to reduce visceral fat and improve insulin resistance in several studies” Dr. Kim said.
“Recently, our group reported that the use of ezetimibe affects autophagy of hepatocytes and the NLRP3 [NOD-like receptors containing pyrin domain 3] inflammasome,” he said.
Moreover, he added, “ezetimibe improved NASH [nonalcoholic steatohepatitis] in an animal model. However, the effects of ezetimibe have not been clearly shown in a human study.”
Dr. Kim also acknowledged a prior randomized control trial that had looked at the role of ezetimibe in 50 patients with NASH, but had not shown a benefit for the drug over placebo in terms of liver fat reduction.
Addressing the Hawthorne effect
“The size of the effect by that might actually be more modest due to the Hawthorne effect,” said session chair Onno Holleboom, MD, PhD, of Amsterdam UMC in the Netherlands.
“What we observe in the large clinical trials is an enormous Hawthorne effect – participating in a NAFLD trial makes people live healthier because they have health checks,” he said.
“That’s a major problem for showing efficacy for the intervention arm,” he added, but of course the open design meant that the trial only had intervention arms; “there was no placebo arm.”
A randomized, active-controlled, clinician-initiated trial
The main objective of the ESSENTIAL trial was therefore to take another look at the potential effect of ezetimibe on hepatic steatosis and doing so in the setting of statin therapy.
In all, 70 patients with NAFLD that had been confirmed via ultrasound were recruited into the prospective, single center, phase 4 trial. Participants were randomized 1:1 to received either ezetimibe 10 mg plus rosuvastatin 5 mg daily or rosuvastatin 5 mg for up to 24 weeks.
Change in liver fat was measured via MRI-PDFF, taking the average values in each of nine liver segments. Magnetic resonance elastography (MRE) was also used to measure liver fibrosis, although results did not show any differences either from baseline to end of treatment values in either group or when the two treatment groups were compared.
Dr. Kim reported that both treatment with the ezetimibe-rosuvastatin combination and rosuvastatin monotherapy reduced parameters that might be associated with a negative outcome in NAFLD, such as body mass index and waist circumference, triglycerides, and LDL cholesterol. There was also a reduction in C-reactive protein levels in the blood, and interleulin-18. There was no change in liver enzymes.
Several subgroup analyses were performed indicating that “individuals with higher BMI, type 2 diabetes, insulin resistance, and severe liver fibrosis were likely to be good responders to ezetimibe treatment,” Dr. Kim said.
“These data indicate that ezetimibe plus rosuvastatin is a safe and effective therapeutic option to treat patients with NAFLD and dyslipidemia,” he concluded.
The results of the ESSENTIAL study have been published in BMC Medicine.
The study was funded by the Yuhan Corporation. Dr. Kim had no conflicts of interest to report. Dr. Holleboom was not involved in the study and had no conflicts of interest.
Ezetimibe given in combination with rosuvastatin has a beneficial effect on liver fat in people with nonalcoholic fatty liver disease (NAFLD), according results of a randomized, active-controlled trial.
The findings, which come from the investigator-initiated ESSENTIAL trial, are likely to add to the debate over whether or not the lipid-lowering combination could be of benefit beyond its effects in the blood.
“We used magnetic resonance imaging-derived proton density fat fraction [MRI-PDFF], which is highly reliable method of assessing hepatic steatosis,” Youngjoon Kim, PhD, one of the study investigators, said at the annual meeting of the European Association for the Study of Diabetes in Barcelona.
“It enables accurate, repeatable and reproducible quantitative assessment of liver fat over the entire liver,” observed Dr. Kim, who works at Severance Hospital, part of Yonsei University in Seoul.
He reported that there was a significant 5.8% decrease in liver fat following 24 weeks’ treatment with ezetimibe and rosuvastatin comparing baseline with end of treatment MRI-PDFF values; a drop that was significant (18.2% vs. 12.3%, P < .001).
Rosuvastatin monotherapy also reduced liver fat from 15.0% at baseline to 12.4% after 24 weeks; this drop of 2.6% was also significant (P = .003).
This gave an absolute mean difference between the two study arms of 3.2% (P = .02).
Rationale for the ESSENTIAL study
Dr. Kim observed during his presentation that NAFLD is burgeoning problem around the world. Ezetimibe plus rosuvastatin was a combination treatment already used widely in clinical practice, and there had been some suggestion that ezetimibe might have an effect on liver fat.
“Although the effect of ezetimibe on hepatic steatosis is still controversial, ezetimibe has been reported to reduce visceral fat and improve insulin resistance in several studies” Dr. Kim said.
“Recently, our group reported that the use of ezetimibe affects autophagy of hepatocytes and the NLRP3 [NOD-like receptors containing pyrin domain 3] inflammasome,” he said.
Moreover, he added, “ezetimibe improved NASH [nonalcoholic steatohepatitis] in an animal model. However, the effects of ezetimibe have not been clearly shown in a human study.”
Dr. Kim also acknowledged a prior randomized control trial that had looked at the role of ezetimibe in 50 patients with NASH, but had not shown a benefit for the drug over placebo in terms of liver fat reduction.
Addressing the Hawthorne effect
“The size of the effect by that might actually be more modest due to the Hawthorne effect,” said session chair Onno Holleboom, MD, PhD, of Amsterdam UMC in the Netherlands.
“What we observe in the large clinical trials is an enormous Hawthorne effect – participating in a NAFLD trial makes people live healthier because they have health checks,” he said.
“That’s a major problem for showing efficacy for the intervention arm,” he added, but of course the open design meant that the trial only had intervention arms; “there was no placebo arm.”
A randomized, active-controlled, clinician-initiated trial
The main objective of the ESSENTIAL trial was therefore to take another look at the potential effect of ezetimibe on hepatic steatosis and doing so in the setting of statin therapy.
In all, 70 patients with NAFLD that had been confirmed via ultrasound were recruited into the prospective, single center, phase 4 trial. Participants were randomized 1:1 to received either ezetimibe 10 mg plus rosuvastatin 5 mg daily or rosuvastatin 5 mg for up to 24 weeks.
Change in liver fat was measured via MRI-PDFF, taking the average values in each of nine liver segments. Magnetic resonance elastography (MRE) was also used to measure liver fibrosis, although results did not show any differences either from baseline to end of treatment values in either group or when the two treatment groups were compared.
Dr. Kim reported that both treatment with the ezetimibe-rosuvastatin combination and rosuvastatin monotherapy reduced parameters that might be associated with a negative outcome in NAFLD, such as body mass index and waist circumference, triglycerides, and LDL cholesterol. There was also a reduction in C-reactive protein levels in the blood, and interleulin-18. There was no change in liver enzymes.
Several subgroup analyses were performed indicating that “individuals with higher BMI, type 2 diabetes, insulin resistance, and severe liver fibrosis were likely to be good responders to ezetimibe treatment,” Dr. Kim said.
“These data indicate that ezetimibe plus rosuvastatin is a safe and effective therapeutic option to treat patients with NAFLD and dyslipidemia,” he concluded.
The results of the ESSENTIAL study have been published in BMC Medicine.
The study was funded by the Yuhan Corporation. Dr. Kim had no conflicts of interest to report. Dr. Holleboom was not involved in the study and had no conflicts of interest.
Ezetimibe given in combination with rosuvastatin has a beneficial effect on liver fat in people with nonalcoholic fatty liver disease (NAFLD), according results of a randomized, active-controlled trial.
The findings, which come from the investigator-initiated ESSENTIAL trial, are likely to add to the debate over whether or not the lipid-lowering combination could be of benefit beyond its effects in the blood.
“We used magnetic resonance imaging-derived proton density fat fraction [MRI-PDFF], which is highly reliable method of assessing hepatic steatosis,” Youngjoon Kim, PhD, one of the study investigators, said at the annual meeting of the European Association for the Study of Diabetes in Barcelona.
“It enables accurate, repeatable and reproducible quantitative assessment of liver fat over the entire liver,” observed Dr. Kim, who works at Severance Hospital, part of Yonsei University in Seoul.
He reported that there was a significant 5.8% decrease in liver fat following 24 weeks’ treatment with ezetimibe and rosuvastatin comparing baseline with end of treatment MRI-PDFF values; a drop that was significant (18.2% vs. 12.3%, P < .001).
Rosuvastatin monotherapy also reduced liver fat from 15.0% at baseline to 12.4% after 24 weeks; this drop of 2.6% was also significant (P = .003).
This gave an absolute mean difference between the two study arms of 3.2% (P = .02).
Rationale for the ESSENTIAL study
Dr. Kim observed during his presentation that NAFLD is burgeoning problem around the world. Ezetimibe plus rosuvastatin was a combination treatment already used widely in clinical practice, and there had been some suggestion that ezetimibe might have an effect on liver fat.
“Although the effect of ezetimibe on hepatic steatosis is still controversial, ezetimibe has been reported to reduce visceral fat and improve insulin resistance in several studies” Dr. Kim said.
“Recently, our group reported that the use of ezetimibe affects autophagy of hepatocytes and the NLRP3 [NOD-like receptors containing pyrin domain 3] inflammasome,” he said.
Moreover, he added, “ezetimibe improved NASH [nonalcoholic steatohepatitis] in an animal model. However, the effects of ezetimibe have not been clearly shown in a human study.”
Dr. Kim also acknowledged a prior randomized control trial that had looked at the role of ezetimibe in 50 patients with NASH, but had not shown a benefit for the drug over placebo in terms of liver fat reduction.
Addressing the Hawthorne effect
“The size of the effect by that might actually be more modest due to the Hawthorne effect,” said session chair Onno Holleboom, MD, PhD, of Amsterdam UMC in the Netherlands.
“What we observe in the large clinical trials is an enormous Hawthorne effect – participating in a NAFLD trial makes people live healthier because they have health checks,” he said.
“That’s a major problem for showing efficacy for the intervention arm,” he added, but of course the open design meant that the trial only had intervention arms; “there was no placebo arm.”
A randomized, active-controlled, clinician-initiated trial
The main objective of the ESSENTIAL trial was therefore to take another look at the potential effect of ezetimibe on hepatic steatosis and doing so in the setting of statin therapy.
In all, 70 patients with NAFLD that had been confirmed via ultrasound were recruited into the prospective, single center, phase 4 trial. Participants were randomized 1:1 to received either ezetimibe 10 mg plus rosuvastatin 5 mg daily or rosuvastatin 5 mg for up to 24 weeks.
Change in liver fat was measured via MRI-PDFF, taking the average values in each of nine liver segments. Magnetic resonance elastography (MRE) was also used to measure liver fibrosis, although results did not show any differences either from baseline to end of treatment values in either group or when the two treatment groups were compared.
Dr. Kim reported that both treatment with the ezetimibe-rosuvastatin combination and rosuvastatin monotherapy reduced parameters that might be associated with a negative outcome in NAFLD, such as body mass index and waist circumference, triglycerides, and LDL cholesterol. There was also a reduction in C-reactive protein levels in the blood, and interleulin-18. There was no change in liver enzymes.
Several subgroup analyses were performed indicating that “individuals with higher BMI, type 2 diabetes, insulin resistance, and severe liver fibrosis were likely to be good responders to ezetimibe treatment,” Dr. Kim said.
“These data indicate that ezetimibe plus rosuvastatin is a safe and effective therapeutic option to treat patients with NAFLD and dyslipidemia,” he concluded.
The results of the ESSENTIAL study have been published in BMC Medicine.
The study was funded by the Yuhan Corporation. Dr. Kim had no conflicts of interest to report. Dr. Holleboom was not involved in the study and had no conflicts of interest.
FROM EASD 2022
Why private practice will always survive: Seven doctors who left employment tell why
Employed physicians are often torn. Many relish the steady salary and ability to focus on being a physician rather than handle administrative duties, but they bemoan their employers’ rules and their lack of input into key decisions. And thus, many doctors are leaving employment to start a private practice. For this article,
Leaving employment is ‘an invigorating time’
On Sept. 9, Aaron Przybysz, MD, gave notice to his employer, a large academic medical center in Southern California, that he would be leaving to start a private practice.
“It’s an invigorating time,” said Dr. Przybysz, 41, an anesthesiologist and pain management physician who plans to open his new pain management practice on Dec. 1 in Orange County. He has picked out the space he will rent but has not yet hired his staff.
“I’ve been serious about doing this for at least a year,” Dr. Przybysz said. “What held me back is the concern that my business could fail. But even if that happens, what’s the worst that could occur? I’d have to find a new job as an employed physician.
“I feel comfortable with the business side of medicine,” he said. His father was an executive in the automotive industry and his father-in-law is an entrepreneur in construction and housing.
“One of the biggest reasons for moving to private practice is making sure I don’t miss my kids’ activities,” he said, referring to his children, ages 9 and 7. Recently, he said, “I had to spend the whole weekend on call in the hospital. I came home and had to sleep most of the next day.
“I love the people that I have been working with and I’ve learned and matured as a physician during that time,” he said. “But it was time to move on.”
The desire to be in charge
In Medscape’s recent Employed Physicians Report, doctors said they enjoy the steady salary and ability to focus on patients, which comes with being employed.
Other physicians feel differently. John Machata, MD, a solo family physician in the village of Wickford, R.I., 20 miles south of Providence, chose private practice because “I have total control,” he said. “I make decisions that I couldn’t have made as an employed physician, such as closing my practice to new patients.”
He can also decide on his work hours. “I see patients for 35 hours, 4 days a week and then I have a 3-day weekend.” In a large organization, “the focus is on revenue,” said Dr. Machata. “They’re always measuring your productivity. If you are slower, you won’t make enough money for them.”
When he worked for a large group practice about a decade ago, “I felt burnt out every day,” he said. “I had to see patients every 10 minutes, with no breaks for anything in between. Within a month I was devising my exit strategy.”
Dr. Machata maintains long appointments – 25 minutes for a typical follow-up visit and 55 minutes for an annual check-in – but he still earns above the state average for primary care doctors. “I have no nurse or front-office staff, which means I can save $125,000 to $150,000 a year,” he said.
In 2018, for the first time, employed physicians outnumbered self-employed physicians, according to a survey by the American Medical Association (AMA). By the end of 2021, more than half (52.1%) of U.S. physicians were employed by hospitals or health systems.
Yet the negatives of employment have begun to turn some physicians back toward private practice. Many physicians who were employed by a hospital or a large practice have become disillusioned and want to return to private practice.
His practice is the ‘best of both worlds’
Adam Bruggeman, MD, a 42-year-old spine surgeon who is CEO of Texas Spine Care Center, a solo practice in San Antonio, said he has “the best of both worlds.”
“As a solo physician, I have total control over how I practice,” he said. “But I also have access to value-based contracts and the data and staff needed to implement them.
“You need a lot of administrative overhead to take on these contracts, which a private practice normally doesn’t have,” he said. But Dr. Bruggeman gets this work done through a clinically integrated network (CIN) of private practices, Spinalytics of Texas, where he is chief medical director.
The CIN represents 150 musculoskeletal care providers and provides access to bundled networks, such as a total joint bundle with Blue Cross Blue Shield of Texas, as well as fee-for-service contracts.
He is also building a new ambulatory surgery center (ASC) that is scheduled to open in January. There, he plans to perform total joint and spine surgeries at a lower cost than at the hospital, which will be useful for value-based contracts through the CIN.
Dr. Bruggeman said it would be hard to run his private practice without the CIN and the ASC. “Private practice has changed,” he said. “The days of hanging up a shingle and immediately being successful are gone. You’ve got to be smart about business to run a successful practice.”
He started his practice while the pandemic raged
Joe Greene, MD, 42, an orthopedic surgeon in Louisville, Ky., had to open his hip and knee surgery practice when the COVID-19 pandemic was raging a year and a half ago, but that did not stop him.
“Federal financing of small bank loans completely stopped, but that only amounted to a small delay because our bank took care of it,” said Dr. Greene, who codirects his new practice with another orthopedic surgeon.
Even during the pandemic, “we could be very nimble,” he said. “For instance, when we want to institute new technology or a new patient-centric educational platform, we can do it immediately rather than going through an approval process at a health system.”
The partners, both ex-employees of a health system, also have an ASC, which allows them better control over their surgery schedules. “At a hospital, you can be bumped from the schedule by other surgeries, and you can’t be as productive as an ASC in the number of surgeries per day,” he said.
Dr. Greene attributes the practice’s success to long and careful planning. “We had to learn about business,” he said. “We did 3 to 4 years of research to find the right business model and implement it.”
As they were considering the new practice, a survey of patients showed that more than 75% chose them by word-of-mouth – because they specialize in complex and revision surgeries – rather than through referrals within their health system. This meant they could survive without their employer.
Planning for the new practice took up all his free time, but now he can relax and spend time with his three daughters, ages 12, 10, and 8. Dr. Greene currently coaches two of their teams. “We’re loving it,” he said.
Colleagues want to know how he did it
Clinton Sheets, MD, an ophthalmologist in Hudson and Clearwater, Fla., went solo in 2019 after being in a group practice for 11 years. Since he opened up, “I get phone calls from colleagues all the time, asking me about how I did it,” he said. “At least two of them followed in my footsteps.
“I tell them it’s very doable,” he said. “If you have the motivation, you can do it. Depending on your competence, you can outsource as much or as little as you want. Some management companies can do almost all of the nonclinical work for you.
“Smaller practices can streamline processes because they have a flatter organizational structure and have fewer issues with administrative bloat than larger organizations,” he said.
“Technology hinders and helps a private practice,” he said. On the one hand, he had to buy a lot of expensive equipment that otherwise would be shared by a group of doctors. On the other hand, using the cloud makes it possible to easily store practice management software and the electronic health record.
He’s opening a private practice while staying employed
In December, Dev Basu, MD, a hospitalist in Baltimore, plans to start his own private practice, seeing patients in skilled nursing homes, while still working as a nocturnist in a large health care system.
He said his employer has been supportive of his plans. “My work will not directly compete with them and it will benefit them by serving patients discharged from their hospitals,” said Dr. Basu, 38. He added, however, that he will be allowed to work only at certain facilities, and these will be subject to annual review.
“The financial risk of the new practice is low, because I haven’t had to invest much,” he said. “I won’t have a staff or an office.” He plans to maintain his full schedule as an employee, working 12 nights a month, because it will give him a great deal of time to do the new work.
“I also have no particular interest in running a business,” he said. “I come from a family of doctors, professors, and teachers who never ran a business. But I’m willing to learn so that I can practice medicine the way I want to.
“The ability to set my own schedule and deal with patients in the way I think is best is very important to me,” he said.
Private practitioners don’t have to face ‘moral distress’
One thing private practitioners typically don’t have to contend with is “moral distress,” which occurs when you have to follow institutional concerns on how much time you can spend with a patient or on the need to keep referrals in-house, according to Marie T. Brown, MD.
Dr. Brown is an internist who ran a small private practice in Oak Park, Ill., and is now the physician lead for the American Medical Association’s STEPS Forward program, which provides strategies on how to improve a medical practice.
“In my private practice, I could control the time I spent with each patient,” she said. “I also had control over my schedule. If I didn’t have the time, I just took a lower income, but that was okay.”
Dr. Brown said it is a myth that employment offers a better work-life balance. “Young physicians who take employment for this reason may find that they’re not allowed to drop off and pick up their children from school at a certain time. But you can do that in a private practice.”
She said it’s not that hard to run a practice. “Young physicians don’t think they could run a practice because they don’t have any business skills,” she said. “Yes, you do need some management skills, and you have to devote time to management. But you don’t need to have special expertise. You can outsource much of the work.”
A growing trend?
David J. Zetter, a consultant in Mechanicsburg, Pa., who helps doctors set up private practices, sees more interest in this in the past 5 years. “The overwhelming trend used to be private practices being bought up by hospitals and other entities,” he said. “Now we’re seeing the pendulum swing in the opposite direction.
“Generally, these doctors are fed up with being employed at a large organization,” he added. “Recently I got a call from a doctor who had never thought about running his own business, but he’s had it with being an employed physician.”
Switching to private practice is scary for a lot of them, but the alternative is worse. “A podiatrist I’m working with tells me she is scared to death about setting up a private practice, but she’s doing it because she doesn’t want to be employed anymore,” Mr. Zetter said.
A version of this article first appeared on Medscape.com.
Employed physicians are often torn. Many relish the steady salary and ability to focus on being a physician rather than handle administrative duties, but they bemoan their employers’ rules and their lack of input into key decisions. And thus, many doctors are leaving employment to start a private practice. For this article,
Leaving employment is ‘an invigorating time’
On Sept. 9, Aaron Przybysz, MD, gave notice to his employer, a large academic medical center in Southern California, that he would be leaving to start a private practice.
“It’s an invigorating time,” said Dr. Przybysz, 41, an anesthesiologist and pain management physician who plans to open his new pain management practice on Dec. 1 in Orange County. He has picked out the space he will rent but has not yet hired his staff.
“I’ve been serious about doing this for at least a year,” Dr. Przybysz said. “What held me back is the concern that my business could fail. But even if that happens, what’s the worst that could occur? I’d have to find a new job as an employed physician.
“I feel comfortable with the business side of medicine,” he said. His father was an executive in the automotive industry and his father-in-law is an entrepreneur in construction and housing.
“One of the biggest reasons for moving to private practice is making sure I don’t miss my kids’ activities,” he said, referring to his children, ages 9 and 7. Recently, he said, “I had to spend the whole weekend on call in the hospital. I came home and had to sleep most of the next day.
“I love the people that I have been working with and I’ve learned and matured as a physician during that time,” he said. “But it was time to move on.”
The desire to be in charge
In Medscape’s recent Employed Physicians Report, doctors said they enjoy the steady salary and ability to focus on patients, which comes with being employed.
Other physicians feel differently. John Machata, MD, a solo family physician in the village of Wickford, R.I., 20 miles south of Providence, chose private practice because “I have total control,” he said. “I make decisions that I couldn’t have made as an employed physician, such as closing my practice to new patients.”
He can also decide on his work hours. “I see patients for 35 hours, 4 days a week and then I have a 3-day weekend.” In a large organization, “the focus is on revenue,” said Dr. Machata. “They’re always measuring your productivity. If you are slower, you won’t make enough money for them.”
When he worked for a large group practice about a decade ago, “I felt burnt out every day,” he said. “I had to see patients every 10 minutes, with no breaks for anything in between. Within a month I was devising my exit strategy.”
Dr. Machata maintains long appointments – 25 minutes for a typical follow-up visit and 55 minutes for an annual check-in – but he still earns above the state average for primary care doctors. “I have no nurse or front-office staff, which means I can save $125,000 to $150,000 a year,” he said.
In 2018, for the first time, employed physicians outnumbered self-employed physicians, according to a survey by the American Medical Association (AMA). By the end of 2021, more than half (52.1%) of U.S. physicians were employed by hospitals or health systems.
Yet the negatives of employment have begun to turn some physicians back toward private practice. Many physicians who were employed by a hospital or a large practice have become disillusioned and want to return to private practice.
His practice is the ‘best of both worlds’
Adam Bruggeman, MD, a 42-year-old spine surgeon who is CEO of Texas Spine Care Center, a solo practice in San Antonio, said he has “the best of both worlds.”
“As a solo physician, I have total control over how I practice,” he said. “But I also have access to value-based contracts and the data and staff needed to implement them.
“You need a lot of administrative overhead to take on these contracts, which a private practice normally doesn’t have,” he said. But Dr. Bruggeman gets this work done through a clinically integrated network (CIN) of private practices, Spinalytics of Texas, where he is chief medical director.
The CIN represents 150 musculoskeletal care providers and provides access to bundled networks, such as a total joint bundle with Blue Cross Blue Shield of Texas, as well as fee-for-service contracts.
He is also building a new ambulatory surgery center (ASC) that is scheduled to open in January. There, he plans to perform total joint and spine surgeries at a lower cost than at the hospital, which will be useful for value-based contracts through the CIN.
Dr. Bruggeman said it would be hard to run his private practice without the CIN and the ASC. “Private practice has changed,” he said. “The days of hanging up a shingle and immediately being successful are gone. You’ve got to be smart about business to run a successful practice.”
He started his practice while the pandemic raged
Joe Greene, MD, 42, an orthopedic surgeon in Louisville, Ky., had to open his hip and knee surgery practice when the COVID-19 pandemic was raging a year and a half ago, but that did not stop him.
“Federal financing of small bank loans completely stopped, but that only amounted to a small delay because our bank took care of it,” said Dr. Greene, who codirects his new practice with another orthopedic surgeon.
Even during the pandemic, “we could be very nimble,” he said. “For instance, when we want to institute new technology or a new patient-centric educational platform, we can do it immediately rather than going through an approval process at a health system.”
The partners, both ex-employees of a health system, also have an ASC, which allows them better control over their surgery schedules. “At a hospital, you can be bumped from the schedule by other surgeries, and you can’t be as productive as an ASC in the number of surgeries per day,” he said.
Dr. Greene attributes the practice’s success to long and careful planning. “We had to learn about business,” he said. “We did 3 to 4 years of research to find the right business model and implement it.”
As they were considering the new practice, a survey of patients showed that more than 75% chose them by word-of-mouth – because they specialize in complex and revision surgeries – rather than through referrals within their health system. This meant they could survive without their employer.
Planning for the new practice took up all his free time, but now he can relax and spend time with his three daughters, ages 12, 10, and 8. Dr. Greene currently coaches two of their teams. “We’re loving it,” he said.
Colleagues want to know how he did it
Clinton Sheets, MD, an ophthalmologist in Hudson and Clearwater, Fla., went solo in 2019 after being in a group practice for 11 years. Since he opened up, “I get phone calls from colleagues all the time, asking me about how I did it,” he said. “At least two of them followed in my footsteps.
“I tell them it’s very doable,” he said. “If you have the motivation, you can do it. Depending on your competence, you can outsource as much or as little as you want. Some management companies can do almost all of the nonclinical work for you.
“Smaller practices can streamline processes because they have a flatter organizational structure and have fewer issues with administrative bloat than larger organizations,” he said.
“Technology hinders and helps a private practice,” he said. On the one hand, he had to buy a lot of expensive equipment that otherwise would be shared by a group of doctors. On the other hand, using the cloud makes it possible to easily store practice management software and the electronic health record.
He’s opening a private practice while staying employed
In December, Dev Basu, MD, a hospitalist in Baltimore, plans to start his own private practice, seeing patients in skilled nursing homes, while still working as a nocturnist in a large health care system.
He said his employer has been supportive of his plans. “My work will not directly compete with them and it will benefit them by serving patients discharged from their hospitals,” said Dr. Basu, 38. He added, however, that he will be allowed to work only at certain facilities, and these will be subject to annual review.
“The financial risk of the new practice is low, because I haven’t had to invest much,” he said. “I won’t have a staff or an office.” He plans to maintain his full schedule as an employee, working 12 nights a month, because it will give him a great deal of time to do the new work.
“I also have no particular interest in running a business,” he said. “I come from a family of doctors, professors, and teachers who never ran a business. But I’m willing to learn so that I can practice medicine the way I want to.
“The ability to set my own schedule and deal with patients in the way I think is best is very important to me,” he said.
Private practitioners don’t have to face ‘moral distress’
One thing private practitioners typically don’t have to contend with is “moral distress,” which occurs when you have to follow institutional concerns on how much time you can spend with a patient or on the need to keep referrals in-house, according to Marie T. Brown, MD.
Dr. Brown is an internist who ran a small private practice in Oak Park, Ill., and is now the physician lead for the American Medical Association’s STEPS Forward program, which provides strategies on how to improve a medical practice.
“In my private practice, I could control the time I spent with each patient,” she said. “I also had control over my schedule. If I didn’t have the time, I just took a lower income, but that was okay.”
Dr. Brown said it is a myth that employment offers a better work-life balance. “Young physicians who take employment for this reason may find that they’re not allowed to drop off and pick up their children from school at a certain time. But you can do that in a private practice.”
She said it’s not that hard to run a practice. “Young physicians don’t think they could run a practice because they don’t have any business skills,” she said. “Yes, you do need some management skills, and you have to devote time to management. But you don’t need to have special expertise. You can outsource much of the work.”
A growing trend?
David J. Zetter, a consultant in Mechanicsburg, Pa., who helps doctors set up private practices, sees more interest in this in the past 5 years. “The overwhelming trend used to be private practices being bought up by hospitals and other entities,” he said. “Now we’re seeing the pendulum swing in the opposite direction.
“Generally, these doctors are fed up with being employed at a large organization,” he added. “Recently I got a call from a doctor who had never thought about running his own business, but he’s had it with being an employed physician.”
Switching to private practice is scary for a lot of them, but the alternative is worse. “A podiatrist I’m working with tells me she is scared to death about setting up a private practice, but she’s doing it because she doesn’t want to be employed anymore,” Mr. Zetter said.
A version of this article first appeared on Medscape.com.
Employed physicians are often torn. Many relish the steady salary and ability to focus on being a physician rather than handle administrative duties, but they bemoan their employers’ rules and their lack of input into key decisions. And thus, many doctors are leaving employment to start a private practice. For this article,
Leaving employment is ‘an invigorating time’
On Sept. 9, Aaron Przybysz, MD, gave notice to his employer, a large academic medical center in Southern California, that he would be leaving to start a private practice.
“It’s an invigorating time,” said Dr. Przybysz, 41, an anesthesiologist and pain management physician who plans to open his new pain management practice on Dec. 1 in Orange County. He has picked out the space he will rent but has not yet hired his staff.
“I’ve been serious about doing this for at least a year,” Dr. Przybysz said. “What held me back is the concern that my business could fail. But even if that happens, what’s the worst that could occur? I’d have to find a new job as an employed physician.
“I feel comfortable with the business side of medicine,” he said. His father was an executive in the automotive industry and his father-in-law is an entrepreneur in construction and housing.
“One of the biggest reasons for moving to private practice is making sure I don’t miss my kids’ activities,” he said, referring to his children, ages 9 and 7. Recently, he said, “I had to spend the whole weekend on call in the hospital. I came home and had to sleep most of the next day.
“I love the people that I have been working with and I’ve learned and matured as a physician during that time,” he said. “But it was time to move on.”
The desire to be in charge
In Medscape’s recent Employed Physicians Report, doctors said they enjoy the steady salary and ability to focus on patients, which comes with being employed.
Other physicians feel differently. John Machata, MD, a solo family physician in the village of Wickford, R.I., 20 miles south of Providence, chose private practice because “I have total control,” he said. “I make decisions that I couldn’t have made as an employed physician, such as closing my practice to new patients.”
He can also decide on his work hours. “I see patients for 35 hours, 4 days a week and then I have a 3-day weekend.” In a large organization, “the focus is on revenue,” said Dr. Machata. “They’re always measuring your productivity. If you are slower, you won’t make enough money for them.”
When he worked for a large group practice about a decade ago, “I felt burnt out every day,” he said. “I had to see patients every 10 minutes, with no breaks for anything in between. Within a month I was devising my exit strategy.”
Dr. Machata maintains long appointments – 25 minutes for a typical follow-up visit and 55 minutes for an annual check-in – but he still earns above the state average for primary care doctors. “I have no nurse or front-office staff, which means I can save $125,000 to $150,000 a year,” he said.
In 2018, for the first time, employed physicians outnumbered self-employed physicians, according to a survey by the American Medical Association (AMA). By the end of 2021, more than half (52.1%) of U.S. physicians were employed by hospitals or health systems.
Yet the negatives of employment have begun to turn some physicians back toward private practice. Many physicians who were employed by a hospital or a large practice have become disillusioned and want to return to private practice.
His practice is the ‘best of both worlds’
Adam Bruggeman, MD, a 42-year-old spine surgeon who is CEO of Texas Spine Care Center, a solo practice in San Antonio, said he has “the best of both worlds.”
“As a solo physician, I have total control over how I practice,” he said. “But I also have access to value-based contracts and the data and staff needed to implement them.
“You need a lot of administrative overhead to take on these contracts, which a private practice normally doesn’t have,” he said. But Dr. Bruggeman gets this work done through a clinically integrated network (CIN) of private practices, Spinalytics of Texas, where he is chief medical director.
The CIN represents 150 musculoskeletal care providers and provides access to bundled networks, such as a total joint bundle with Blue Cross Blue Shield of Texas, as well as fee-for-service contracts.
He is also building a new ambulatory surgery center (ASC) that is scheduled to open in January. There, he plans to perform total joint and spine surgeries at a lower cost than at the hospital, which will be useful for value-based contracts through the CIN.
Dr. Bruggeman said it would be hard to run his private practice without the CIN and the ASC. “Private practice has changed,” he said. “The days of hanging up a shingle and immediately being successful are gone. You’ve got to be smart about business to run a successful practice.”
He started his practice while the pandemic raged
Joe Greene, MD, 42, an orthopedic surgeon in Louisville, Ky., had to open his hip and knee surgery practice when the COVID-19 pandemic was raging a year and a half ago, but that did not stop him.
“Federal financing of small bank loans completely stopped, but that only amounted to a small delay because our bank took care of it,” said Dr. Greene, who codirects his new practice with another orthopedic surgeon.
Even during the pandemic, “we could be very nimble,” he said. “For instance, when we want to institute new technology or a new patient-centric educational platform, we can do it immediately rather than going through an approval process at a health system.”
The partners, both ex-employees of a health system, also have an ASC, which allows them better control over their surgery schedules. “At a hospital, you can be bumped from the schedule by other surgeries, and you can’t be as productive as an ASC in the number of surgeries per day,” he said.
Dr. Greene attributes the practice’s success to long and careful planning. “We had to learn about business,” he said. “We did 3 to 4 years of research to find the right business model and implement it.”
As they were considering the new practice, a survey of patients showed that more than 75% chose them by word-of-mouth – because they specialize in complex and revision surgeries – rather than through referrals within their health system. This meant they could survive without their employer.
Planning for the new practice took up all his free time, but now he can relax and spend time with his three daughters, ages 12, 10, and 8. Dr. Greene currently coaches two of their teams. “We’re loving it,” he said.
Colleagues want to know how he did it
Clinton Sheets, MD, an ophthalmologist in Hudson and Clearwater, Fla., went solo in 2019 after being in a group practice for 11 years. Since he opened up, “I get phone calls from colleagues all the time, asking me about how I did it,” he said. “At least two of them followed in my footsteps.
“I tell them it’s very doable,” he said. “If you have the motivation, you can do it. Depending on your competence, you can outsource as much or as little as you want. Some management companies can do almost all of the nonclinical work for you.
“Smaller practices can streamline processes because they have a flatter organizational structure and have fewer issues with administrative bloat than larger organizations,” he said.
“Technology hinders and helps a private practice,” he said. On the one hand, he had to buy a lot of expensive equipment that otherwise would be shared by a group of doctors. On the other hand, using the cloud makes it possible to easily store practice management software and the electronic health record.
He’s opening a private practice while staying employed
In December, Dev Basu, MD, a hospitalist in Baltimore, plans to start his own private practice, seeing patients in skilled nursing homes, while still working as a nocturnist in a large health care system.
He said his employer has been supportive of his plans. “My work will not directly compete with them and it will benefit them by serving patients discharged from their hospitals,” said Dr. Basu, 38. He added, however, that he will be allowed to work only at certain facilities, and these will be subject to annual review.
“The financial risk of the new practice is low, because I haven’t had to invest much,” he said. “I won’t have a staff or an office.” He plans to maintain his full schedule as an employee, working 12 nights a month, because it will give him a great deal of time to do the new work.
“I also have no particular interest in running a business,” he said. “I come from a family of doctors, professors, and teachers who never ran a business. But I’m willing to learn so that I can practice medicine the way I want to.
“The ability to set my own schedule and deal with patients in the way I think is best is very important to me,” he said.
Private practitioners don’t have to face ‘moral distress’
One thing private practitioners typically don’t have to contend with is “moral distress,” which occurs when you have to follow institutional concerns on how much time you can spend with a patient or on the need to keep referrals in-house, according to Marie T. Brown, MD.
Dr. Brown is an internist who ran a small private practice in Oak Park, Ill., and is now the physician lead for the American Medical Association’s STEPS Forward program, which provides strategies on how to improve a medical practice.
“In my private practice, I could control the time I spent with each patient,” she said. “I also had control over my schedule. If I didn’t have the time, I just took a lower income, but that was okay.”
Dr. Brown said it is a myth that employment offers a better work-life balance. “Young physicians who take employment for this reason may find that they’re not allowed to drop off and pick up their children from school at a certain time. But you can do that in a private practice.”
She said it’s not that hard to run a practice. “Young physicians don’t think they could run a practice because they don’t have any business skills,” she said. “Yes, you do need some management skills, and you have to devote time to management. But you don’t need to have special expertise. You can outsource much of the work.”
A growing trend?
David J. Zetter, a consultant in Mechanicsburg, Pa., who helps doctors set up private practices, sees more interest in this in the past 5 years. “The overwhelming trend used to be private practices being bought up by hospitals and other entities,” he said. “Now we’re seeing the pendulum swing in the opposite direction.
“Generally, these doctors are fed up with being employed at a large organization,” he added. “Recently I got a call from a doctor who had never thought about running his own business, but he’s had it with being an employed physician.”
Switching to private practice is scary for a lot of them, but the alternative is worse. “A podiatrist I’m working with tells me she is scared to death about setting up a private practice, but she’s doing it because she doesn’t want to be employed anymore,” Mr. Zetter said.
A version of this article first appeared on Medscape.com.