User login
Two consecutive negative FUBC results clear S. aureus bacteremia
reported Caitlin Cardenas-Comfort, MD, of the section of pediatric infectious diseases at Baylor College of Medicine, Houston, and colleagues.

In a retrospective cohort study of 122 pediatric patients with documented Staphylococcus aureus bacteremia (SAB) that were hospitalized at one of three hospitals in the Texas Children’s Hospital network in Houston, Dr. Cardenas-Comfort and colleagues sought to determine whether specific recommendations can be made on the number of follow-up blood cultures (FUBC) needed to document clearance of SAB. Patients included in the study were under 18 years of age and had confirmed diagnosis of SAB between Jan. 1, and Dec. 31, 2018.
Most cases of bacteremia resolve in under 48 hours
In the majority of cases, patients had bacteremia for less than 48 hours and few to no complications. Only 16% of patients experienced bacteremia lasting 3 or more days, and they had either central line-associated bloodstream infection, endocarditis, or osteomyelitis. In such cases, “patients with endovascular and closed-space infections are at an increased risk of persistent bacteremia,” warranting more conservative monitoring and follow-up, cautioned the researchers.
Although Dr. Cardenas-Comfort and colleagues did note an association between the duration of bacteremia and a diagnosis of infectious disease, increased risk for persistent SAB did not appear to be tied to an underlying medical condition, including immunosuppression.
Fewer than 5% of patients with SAB had intermittent positive cultures and fewer than 1% had repeat positive cultures following two negative FUBC results. For those patients with intermittent positive cultures, the risk of being diagnosed with endocarditis or osteomyelitis is more than double. The authors suggested that “source control could be a critical variable” increasing the risk for intermittent positive cultures, noting that surgical debridement occurred more than 24 hours following initial blood draw for every patient in the osteomyelitis group. In contrast, of those who had consistently negative FUBC results, only 2 of 33 (6%) had debridement in the same period, and only 6 of 33 (18%) required more than one debridement.
Children are less likely to have intermittent positive cultures
Dr. Cardenas-Comfort and colleagues also observed that intermittent positive cultures may appear less frequently in children than adults, consistent with a recent study of adults in which intermittent cultures were found in 13% of 1.071 SAB cases. In just 4% of the cases in that study, more than 2 days of negative blood cultures preceded a repeat positive culture.
The researchers noted several study limitations in their own research. Because more than half (61%) of patients had two or less FUBCs collected, and 21% one or less, they acknowledged that their conclusions are based on the presumption that the 61% of patients would not have any further positive cultures if they had been drawn. Relying on provider documentation also suggested that cases of bacteremia without an identified source also likely were overrepresented. The retrospective nature of the study only allowed for limited collection of standardized follow-up metrics with the limited patient sample available. Patient characteristics also may have affected the quality of study results because a large number of patients had underlying medical conditions or were premature infants.
Look for ongoing hemodynamic instability before third FUBC
Dr. Cardenas-Comfort and colleagues only recommend a third FUBC in cases where patients demonstrate ongoing hemodynamic instability. Applying this to their study population, in retrospect, the authors noted that unnecessary FUBCs could have been prevented in 26% of patients included in the study. They further recommend a thorough clinical evaluation for any patients with SAB lasting 3 or more days with an unidentified infection source. Further research could be beneficial in evaluating cost savings that come from eliminating unnecessary cultures. Additionally, performing a powered analysis would help to determine the probability of an increase in complications based on implementation of these recommendations.
In a separate interview, Tina Q. Tan, MD, infectious disease specialist at Ann & Robert H. Lurie Children’s Hospital of Chicago noted: “This study provides some importance evidence-based guidance on deciding how many blood cultures are needed to demonstrate clearance of S. aureus bacteremia, even in children who have intermittent positive cultures after having negative FUBCs. The recommendation that additional blood cultures to document sterility are not needed after 2 FUBC results are negative in well-appearing children is one that has the potential to decrease cost and unnecessary discomfort in patients. The recommendation currently is for well-appearing children; children who are ill appearing may require further blood cultures to document sterility. Even though this is a single-center study with a relatively small number of patients (n = 122), the information provided is a very useful guide to all clinicians who deal with this issue. Further studies are needed to determine the impact on cost reduction by the elimination of unnecessary blood cultures and whether the rate of complications would increase as a result of not obtaining further cultures in well-appearing children who have two negative follow up blood cultures.”
Dr. Cardenas-Comfort and colleagues as well as Dr. Tan had no conflicts of interest and no relevant financial disclosures. There was no external funding for the study.
SOURCE: Cardenas-Comfort C et al. Pediatrics. 2020. doi: 10.1542/peds.2020-1821.
reported Caitlin Cardenas-Comfort, MD, of the section of pediatric infectious diseases at Baylor College of Medicine, Houston, and colleagues.
In a retrospective cohort study of 122 pediatric patients with documented Staphylococcus aureus bacteremia (SAB) that were hospitalized at one of three hospitals in the Texas Children’s Hospital network in Houston, Dr. Cardenas-Comfort and colleagues sought to determine whether specific recommendations can be made on the number of follow-up blood cultures (FUBC) needed to document clearance of SAB. Patients included in the study were under 18 years of age and had confirmed diagnosis of SAB between Jan. 1, and Dec. 31, 2018.
Most cases of bacteremia resolve in under 48 hours
In the majority of cases, patients had bacteremia for less than 48 hours and few to no complications. Only 16% of patients experienced bacteremia lasting 3 or more days, and they had either central line-associated bloodstream infection, endocarditis, or osteomyelitis. In such cases, “patients with endovascular and closed-space infections are at an increased risk of persistent bacteremia,” warranting more conservative monitoring and follow-up, cautioned the researchers.
Although Dr. Cardenas-Comfort and colleagues did note an association between the duration of bacteremia and a diagnosis of infectious disease, increased risk for persistent SAB did not appear to be tied to an underlying medical condition, including immunosuppression.
Fewer than 5% of patients with SAB had intermittent positive cultures and fewer than 1% had repeat positive cultures following two negative FUBC results. For those patients with intermittent positive cultures, the risk of being diagnosed with endocarditis or osteomyelitis is more than double. The authors suggested that “source control could be a critical variable” increasing the risk for intermittent positive cultures, noting that surgical debridement occurred more than 24 hours following initial blood draw for every patient in the osteomyelitis group. In contrast, of those who had consistently negative FUBC results, only 2 of 33 (6%) had debridement in the same period, and only 6 of 33 (18%) required more than one debridement.
Children are less likely to have intermittent positive cultures
Dr. Cardenas-Comfort and colleagues also observed that intermittent positive cultures may appear less frequently in children than adults, consistent with a recent study of adults in which intermittent cultures were found in 13% of 1.071 SAB cases. In just 4% of the cases in that study, more than 2 days of negative blood cultures preceded a repeat positive culture.
The researchers noted several study limitations in their own research. Because more than half (61%) of patients had two or less FUBCs collected, and 21% one or less, they acknowledged that their conclusions are based on the presumption that the 61% of patients would not have any further positive cultures if they had been drawn. Relying on provider documentation also suggested that cases of bacteremia without an identified source also likely were overrepresented. The retrospective nature of the study only allowed for limited collection of standardized follow-up metrics with the limited patient sample available. Patient characteristics also may have affected the quality of study results because a large number of patients had underlying medical conditions or were premature infants.
Look for ongoing hemodynamic instability before third FUBC
Dr. Cardenas-Comfort and colleagues only recommend a third FUBC in cases where patients demonstrate ongoing hemodynamic instability. Applying this to their study population, in retrospect, the authors noted that unnecessary FUBCs could have been prevented in 26% of patients included in the study. They further recommend a thorough clinical evaluation for any patients with SAB lasting 3 or more days with an unidentified infection source. Further research could be beneficial in evaluating cost savings that come from eliminating unnecessary cultures. Additionally, performing a powered analysis would help to determine the probability of an increase in complications based on implementation of these recommendations.
In a separate interview, Tina Q. Tan, MD, infectious disease specialist at Ann & Robert H. Lurie Children’s Hospital of Chicago noted: “This study provides some importance evidence-based guidance on deciding how many blood cultures are needed to demonstrate clearance of S. aureus bacteremia, even in children who have intermittent positive cultures after having negative FUBCs. The recommendation that additional blood cultures to document sterility are not needed after 2 FUBC results are negative in well-appearing children is one that has the potential to decrease cost and unnecessary discomfort in patients. The recommendation currently is for well-appearing children; children who are ill appearing may require further blood cultures to document sterility. Even though this is a single-center study with a relatively small number of patients (n = 122), the information provided is a very useful guide to all clinicians who deal with this issue. Further studies are needed to determine the impact on cost reduction by the elimination of unnecessary blood cultures and whether the rate of complications would increase as a result of not obtaining further cultures in well-appearing children who have two negative follow up blood cultures.”
Dr. Cardenas-Comfort and colleagues as well as Dr. Tan had no conflicts of interest and no relevant financial disclosures. There was no external funding for the study.
SOURCE: Cardenas-Comfort C et al. Pediatrics. 2020. doi: 10.1542/peds.2020-1821.
reported Caitlin Cardenas-Comfort, MD, of the section of pediatric infectious diseases at Baylor College of Medicine, Houston, and colleagues.
In a retrospective cohort study of 122 pediatric patients with documented Staphylococcus aureus bacteremia (SAB) that were hospitalized at one of three hospitals in the Texas Children’s Hospital network in Houston, Dr. Cardenas-Comfort and colleagues sought to determine whether specific recommendations can be made on the number of follow-up blood cultures (FUBC) needed to document clearance of SAB. Patients included in the study were under 18 years of age and had confirmed diagnosis of SAB between Jan. 1, and Dec. 31, 2018.
Most cases of bacteremia resolve in under 48 hours
In the majority of cases, patients had bacteremia for less than 48 hours and few to no complications. Only 16% of patients experienced bacteremia lasting 3 or more days, and they had either central line-associated bloodstream infection, endocarditis, or osteomyelitis. In such cases, “patients with endovascular and closed-space infections are at an increased risk of persistent bacteremia,” warranting more conservative monitoring and follow-up, cautioned the researchers.
Although Dr. Cardenas-Comfort and colleagues did note an association between the duration of bacteremia and a diagnosis of infectious disease, increased risk for persistent SAB did not appear to be tied to an underlying medical condition, including immunosuppression.
Fewer than 5% of patients with SAB had intermittent positive cultures and fewer than 1% had repeat positive cultures following two negative FUBC results. For those patients with intermittent positive cultures, the risk of being diagnosed with endocarditis or osteomyelitis is more than double. The authors suggested that “source control could be a critical variable” increasing the risk for intermittent positive cultures, noting that surgical debridement occurred more than 24 hours following initial blood draw for every patient in the osteomyelitis group. In contrast, of those who had consistently negative FUBC results, only 2 of 33 (6%) had debridement in the same period, and only 6 of 33 (18%) required more than one debridement.
Children are less likely to have intermittent positive cultures
Dr. Cardenas-Comfort and colleagues also observed that intermittent positive cultures may appear less frequently in children than adults, consistent with a recent study of adults in which intermittent cultures were found in 13% of 1.071 SAB cases. In just 4% of the cases in that study, more than 2 days of negative blood cultures preceded a repeat positive culture.
The researchers noted several study limitations in their own research. Because more than half (61%) of patients had two or less FUBCs collected, and 21% one or less, they acknowledged that their conclusions are based on the presumption that the 61% of patients would not have any further positive cultures if they had been drawn. Relying on provider documentation also suggested that cases of bacteremia without an identified source also likely were overrepresented. The retrospective nature of the study only allowed for limited collection of standardized follow-up metrics with the limited patient sample available. Patient characteristics also may have affected the quality of study results because a large number of patients had underlying medical conditions or were premature infants.
Look for ongoing hemodynamic instability before third FUBC
Dr. Cardenas-Comfort and colleagues only recommend a third FUBC in cases where patients demonstrate ongoing hemodynamic instability. Applying this to their study population, in retrospect, the authors noted that unnecessary FUBCs could have been prevented in 26% of patients included in the study. They further recommend a thorough clinical evaluation for any patients with SAB lasting 3 or more days with an unidentified infection source. Further research could be beneficial in evaluating cost savings that come from eliminating unnecessary cultures. Additionally, performing a powered analysis would help to determine the probability of an increase in complications based on implementation of these recommendations.
In a separate interview, Tina Q. Tan, MD, infectious disease specialist at Ann & Robert H. Lurie Children’s Hospital of Chicago noted: “This study provides some importance evidence-based guidance on deciding how many blood cultures are needed to demonstrate clearance of S. aureus bacteremia, even in children who have intermittent positive cultures after having negative FUBCs. The recommendation that additional blood cultures to document sterility are not needed after 2 FUBC results are negative in well-appearing children is one that has the potential to decrease cost and unnecessary discomfort in patients. The recommendation currently is for well-appearing children; children who are ill appearing may require further blood cultures to document sterility. Even though this is a single-center study with a relatively small number of patients (n = 122), the information provided is a very useful guide to all clinicians who deal with this issue. Further studies are needed to determine the impact on cost reduction by the elimination of unnecessary blood cultures and whether the rate of complications would increase as a result of not obtaining further cultures in well-appearing children who have two negative follow up blood cultures.”
Dr. Cardenas-Comfort and colleagues as well as Dr. Tan had no conflicts of interest and no relevant financial disclosures. There was no external funding for the study.
SOURCE: Cardenas-Comfort C et al. Pediatrics. 2020. doi: 10.1542/peds.2020-1821.
FROM PEDIATRICS
Cervical cancer recurrence patterns differ after laparoscopic and open hysterectomy
When cervical cancer recurs after radical hysterectomy, the likelihood of recurrence at certain sites and the timing of recurrence may be associated with the surgical approach, according to a retrospective study.

according to a propensity-matched analysis of data from 105 patients with recurrence.
And recurrence in the pelvic cavity and peritoneal carcinomatosis were more common after laparoscopic hysterectomy than after open surgery. Overall survival was similar between the groups, however.
The different patterns of recurrence may relate to dissemination of the disease during colpotomy, but the reasons are unknown, study author Giorgio Bogani, MD, PhD, said at the meeting sponsored by AAGL.
To examine patterns of recurrence after laparoscopic and open abdominal radical hysterectomy for cervical cancer, Dr. Bogani of the department of gynecologic surgery at the National Cancer Institute in Milan and colleagues analyzed data from patients with cervical cancer who developed recurrence after surgery at two oncologic referral centers between 1990 and 2018 (Int J Gynecol Cancer. 2020 Jul. doi: 10.1136/ijgc-2020-001381).
The investigators applied a propensity-matching algorithm to reduce possible confounding factors. They matched 35 patients who had recurrence after laparoscopic hysterectomy to 70 patients who had recurrence after open surgery. The groups had similar baseline characteristics.
As in the Laparoscopic Approach to Cervical Cancer (LACC) trial, patients who had minimally invasive surgery were more likely to have a worse disease-free survival, compared with patients who had open surgery, Dr. Bogani said. Patients who underwent laparoscopic radical hysterectomy had a median progression-free survival of 8 months, whereas patients who underwent open abdominal procedures had a median progression-free survival of 15.8 months.
Although vaginal, lymphatic, and distant recurrences were similar between the groups, a greater percentage of patients in the laparoscopic hysterectomy group had recurrence in the pelvic cavity (74% vs. 34%) and peritoneal carcinomatosis (17% vs. 1.5%).
The LACC trial, which found significantly lower disease-free and overall survival with laparoscopic hysterectomy, sent a “shockwave through the gynecologic oncology community” when it was published in 2018, said Masoud Azodi, MD, in a discussion following Dr. Bogani’s presentation.
Researchers have raised questions about that trial’s design and validity, noted Dr. Azodi, director of minimally invasive and robotic surgery at Yale University in New Haven, Conn.
It could be that local recurrences are attributable to surgical technique, rather than to the minimally invasive approach in itself, Dr. Azodi said. Prior studies of laparoscopic hysterectomy for cervical cancer had indicated better surgical outcomes and equivalent oncologic results, relative to open surgery.
Before the LACC trial, Dr. Bogani used the minimally invasive approach for almost all surgeries. Since then, he has performed open surgeries. If he were to use a minimally invasive approach now, it would be in the context of a clinical trial, Dr. Bogani said.
Dr. Bogani and Dr. Azodi had no relevant financial disclosures.
SOURCE: Bogani G et al. J Minim Invasive Gynecol. 2020 Nov. doi: 10.1016/j.jmig.2020.08.069.
When cervical cancer recurs after radical hysterectomy, the likelihood of recurrence at certain sites and the timing of recurrence may be associated with the surgical approach, according to a retrospective study.
according to a propensity-matched analysis of data from 105 patients with recurrence.
And recurrence in the pelvic cavity and peritoneal carcinomatosis were more common after laparoscopic hysterectomy than after open surgery. Overall survival was similar between the groups, however.
The different patterns of recurrence may relate to dissemination of the disease during colpotomy, but the reasons are unknown, study author Giorgio Bogani, MD, PhD, said at the meeting sponsored by AAGL.
To examine patterns of recurrence after laparoscopic and open abdominal radical hysterectomy for cervical cancer, Dr. Bogani of the department of gynecologic surgery at the National Cancer Institute in Milan and colleagues analyzed data from patients with cervical cancer who developed recurrence after surgery at two oncologic referral centers between 1990 and 2018 (Int J Gynecol Cancer. 2020 Jul. doi: 10.1136/ijgc-2020-001381).
The investigators applied a propensity-matching algorithm to reduce possible confounding factors. They matched 35 patients who had recurrence after laparoscopic hysterectomy to 70 patients who had recurrence after open surgery. The groups had similar baseline characteristics.
As in the Laparoscopic Approach to Cervical Cancer (LACC) trial, patients who had minimally invasive surgery were more likely to have a worse disease-free survival, compared with patients who had open surgery, Dr. Bogani said. Patients who underwent laparoscopic radical hysterectomy had a median progression-free survival of 8 months, whereas patients who underwent open abdominal procedures had a median progression-free survival of 15.8 months.
Although vaginal, lymphatic, and distant recurrences were similar between the groups, a greater percentage of patients in the laparoscopic hysterectomy group had recurrence in the pelvic cavity (74% vs. 34%) and peritoneal carcinomatosis (17% vs. 1.5%).
The LACC trial, which found significantly lower disease-free and overall survival with laparoscopic hysterectomy, sent a “shockwave through the gynecologic oncology community” when it was published in 2018, said Masoud Azodi, MD, in a discussion following Dr. Bogani’s presentation.
Researchers have raised questions about that trial’s design and validity, noted Dr. Azodi, director of minimally invasive and robotic surgery at Yale University in New Haven, Conn.
It could be that local recurrences are attributable to surgical technique, rather than to the minimally invasive approach in itself, Dr. Azodi said. Prior studies of laparoscopic hysterectomy for cervical cancer had indicated better surgical outcomes and equivalent oncologic results, relative to open surgery.
Before the LACC trial, Dr. Bogani used the minimally invasive approach for almost all surgeries. Since then, he has performed open surgeries. If he were to use a minimally invasive approach now, it would be in the context of a clinical trial, Dr. Bogani said.
Dr. Bogani and Dr. Azodi had no relevant financial disclosures.
SOURCE: Bogani G et al. J Minim Invasive Gynecol. 2020 Nov. doi: 10.1016/j.jmig.2020.08.069.
When cervical cancer recurs after radical hysterectomy, the likelihood of recurrence at certain sites and the timing of recurrence may be associated with the surgical approach, according to a retrospective study.
according to a propensity-matched analysis of data from 105 patients with recurrence.
And recurrence in the pelvic cavity and peritoneal carcinomatosis were more common after laparoscopic hysterectomy than after open surgery. Overall survival was similar between the groups, however.
The different patterns of recurrence may relate to dissemination of the disease during colpotomy, but the reasons are unknown, study author Giorgio Bogani, MD, PhD, said at the meeting sponsored by AAGL.
To examine patterns of recurrence after laparoscopic and open abdominal radical hysterectomy for cervical cancer, Dr. Bogani of the department of gynecologic surgery at the National Cancer Institute in Milan and colleagues analyzed data from patients with cervical cancer who developed recurrence after surgery at two oncologic referral centers between 1990 and 2018 (Int J Gynecol Cancer. 2020 Jul. doi: 10.1136/ijgc-2020-001381).
The investigators applied a propensity-matching algorithm to reduce possible confounding factors. They matched 35 patients who had recurrence after laparoscopic hysterectomy to 70 patients who had recurrence after open surgery. The groups had similar baseline characteristics.
As in the Laparoscopic Approach to Cervical Cancer (LACC) trial, patients who had minimally invasive surgery were more likely to have a worse disease-free survival, compared with patients who had open surgery, Dr. Bogani said. Patients who underwent laparoscopic radical hysterectomy had a median progression-free survival of 8 months, whereas patients who underwent open abdominal procedures had a median progression-free survival of 15.8 months.
Although vaginal, lymphatic, and distant recurrences were similar between the groups, a greater percentage of patients in the laparoscopic hysterectomy group had recurrence in the pelvic cavity (74% vs. 34%) and peritoneal carcinomatosis (17% vs. 1.5%).
The LACC trial, which found significantly lower disease-free and overall survival with laparoscopic hysterectomy, sent a “shockwave through the gynecologic oncology community” when it was published in 2018, said Masoud Azodi, MD, in a discussion following Dr. Bogani’s presentation.
Researchers have raised questions about that trial’s design and validity, noted Dr. Azodi, director of minimally invasive and robotic surgery at Yale University in New Haven, Conn.
It could be that local recurrences are attributable to surgical technique, rather than to the minimally invasive approach in itself, Dr. Azodi said. Prior studies of laparoscopic hysterectomy for cervical cancer had indicated better surgical outcomes and equivalent oncologic results, relative to open surgery.
Before the LACC trial, Dr. Bogani used the minimally invasive approach for almost all surgeries. Since then, he has performed open surgeries. If he were to use a minimally invasive approach now, it would be in the context of a clinical trial, Dr. Bogani said.
Dr. Bogani and Dr. Azodi had no relevant financial disclosures.
SOURCE: Bogani G et al. J Minim Invasive Gynecol. 2020 Nov. doi: 10.1016/j.jmig.2020.08.069.
FROM AAGL GLOBAL CONGRESS

Diabetic retinopathy may predict greater risk of COVID-19 severity
Risk of intubation for COVID-19 in very sick hospitalized patients was increased over fivefold in those with diabetic retinopathy, compared with those without, in a small single-center study from the United Kingdom.
Importantly, the risk of intubation was independent of conventional risk factors for poor COVID-19 outcomes.
“People with preexisting diabetes-related vascular damage, such as retinopathy, might be predisposed to a more severe form of COVID-19 requiring ventilation in the intensive therapy unit,” said lead investigator Janaka Karalliedde, MBBS, PhD.
Dr. Karalliedde and colleagues note that this is “the first description of diabetic retinopathy as a potential risk factor for poor COVID-19 outcomes.”
“For this reason, looking for the presence or history of retinopathy or other vascular complications of diabetes may help health care professionals identify patients at high risk of severe COVID-19,” added Dr. Karalliedde, of Guy’s and St Thomas’ NHS Foundation Trust, London.
The study was published online in Diabetes Research and Clinical Practice.
Preexisting diabetic retinopathy and COVID-19 outcomes
The prevalence of diabetic retinopathy is thought to be around 55% in people with type 1 diabetes and 30% in people with type 2 diabetes, on average.
Dr. Karalliedde is part of a research group at King’s College London that has been focused on how vascular disease may predispose to more severe COVID-19.
“COVID-19 affects the blood vessels all over the body,” he said, so they wondered whether having preexisting retinopathy “would predispose to a severe manifestation of COVID-19.”
The observational study included 187 patients with diabetes (179 patients with type 2 diabetes and 8 patients with type 1 diabetes) hospitalized with COVID-19 at Guy’s and St Thomas’ NHS Foundation Trust between March 12 and April 7 (the peak of the first wave of the pandemic in the United Kingdom).
“It was an ethnically diverse population who were very sick and provides a clinical observation of real life,” Dr. Karalliedde said.
Nearly half of patients were African Caribbean (44%), 39% were White, and 17% were of other ethnicities, including 8% who were Asian. The mean age of the cohort was 68 years (range, 22-97 years), and 60% were men.
Diabetic retinopathy was reported in 67 (36%) patients, of whom 80% had background retinopathy and 20% had more advanced retinopathy.
They then looked at whether the presence of retinopathy was associated with a more severe manifestation of COVID-19 as defined by the need for tracheal intubation.
Of the 187 patients, 26% were intubated and 45% of these patients had diabetic retinopathy.
The analysis showed those with diabetic retinopathy had an over-fivefold increased risk for intubation (odds ratio, 5.81; 95% confidence interval, 1.37-24.66).
Of the entire cohort, 32% of patients died, although no association was observed between retinopathy and mortality.
“A greater number of diabetes patients with COVID-19 ended up on the intensive therapy unit. Upon multivariate analysis, we found retinopathy was independently associated with ending up on the intensive therapy unit,” stressed Dr. Karalliedde.
However, they noted that, “due to the cross-sectional design of our study, we cannot prove causality [between retinopathy and intubation]. Further studies are required to understand the mechanisms that explain the associations between retinopathy and other indices of microangiopathy with severe COVID-19.”
A version of this article originally appeared on Medscape.com.
Risk of intubation for COVID-19 in very sick hospitalized patients was increased over fivefold in those with diabetic retinopathy, compared with those without, in a small single-center study from the United Kingdom.
Importantly, the risk of intubation was independent of conventional risk factors for poor COVID-19 outcomes.
“People with preexisting diabetes-related vascular damage, such as retinopathy, might be predisposed to a more severe form of COVID-19 requiring ventilation in the intensive therapy unit,” said lead investigator Janaka Karalliedde, MBBS, PhD.
Dr. Karalliedde and colleagues note that this is “the first description of diabetic retinopathy as a potential risk factor for poor COVID-19 outcomes.”
“For this reason, looking for the presence or history of retinopathy or other vascular complications of diabetes may help health care professionals identify patients at high risk of severe COVID-19,” added Dr. Karalliedde, of Guy’s and St Thomas’ NHS Foundation Trust, London.
The study was published online in Diabetes Research and Clinical Practice.
Preexisting diabetic retinopathy and COVID-19 outcomes
The prevalence of diabetic retinopathy is thought to be around 55% in people with type 1 diabetes and 30% in people with type 2 diabetes, on average.
Dr. Karalliedde is part of a research group at King’s College London that has been focused on how vascular disease may predispose to more severe COVID-19.
“COVID-19 affects the blood vessels all over the body,” he said, so they wondered whether having preexisting retinopathy “would predispose to a severe manifestation of COVID-19.”
The observational study included 187 patients with diabetes (179 patients with type 2 diabetes and 8 patients with type 1 diabetes) hospitalized with COVID-19 at Guy’s and St Thomas’ NHS Foundation Trust between March 12 and April 7 (the peak of the first wave of the pandemic in the United Kingdom).
“It was an ethnically diverse population who were very sick and provides a clinical observation of real life,” Dr. Karalliedde said.
Nearly half of patients were African Caribbean (44%), 39% were White, and 17% were of other ethnicities, including 8% who were Asian. The mean age of the cohort was 68 years (range, 22-97 years), and 60% were men.
Diabetic retinopathy was reported in 67 (36%) patients, of whom 80% had background retinopathy and 20% had more advanced retinopathy.
They then looked at whether the presence of retinopathy was associated with a more severe manifestation of COVID-19 as defined by the need for tracheal intubation.
Of the 187 patients, 26% were intubated and 45% of these patients had diabetic retinopathy.
The analysis showed those with diabetic retinopathy had an over-fivefold increased risk for intubation (odds ratio, 5.81; 95% confidence interval, 1.37-24.66).
Of the entire cohort, 32% of patients died, although no association was observed between retinopathy and mortality.
“A greater number of diabetes patients with COVID-19 ended up on the intensive therapy unit. Upon multivariate analysis, we found retinopathy was independently associated with ending up on the intensive therapy unit,” stressed Dr. Karalliedde.
However, they noted that, “due to the cross-sectional design of our study, we cannot prove causality [between retinopathy and intubation]. Further studies are required to understand the mechanisms that explain the associations between retinopathy and other indices of microangiopathy with severe COVID-19.”
A version of this article originally appeared on Medscape.com.
Risk of intubation for COVID-19 in very sick hospitalized patients was increased over fivefold in those with diabetic retinopathy, compared with those without, in a small single-center study from the United Kingdom.
Importantly, the risk of intubation was independent of conventional risk factors for poor COVID-19 outcomes.
“People with preexisting diabetes-related vascular damage, such as retinopathy, might be predisposed to a more severe form of COVID-19 requiring ventilation in the intensive therapy unit,” said lead investigator Janaka Karalliedde, MBBS, PhD.
Dr. Karalliedde and colleagues note that this is “the first description of diabetic retinopathy as a potential risk factor for poor COVID-19 outcomes.”
“For this reason, looking for the presence or history of retinopathy or other vascular complications of diabetes may help health care professionals identify patients at high risk of severe COVID-19,” added Dr. Karalliedde, of Guy’s and St Thomas’ NHS Foundation Trust, London.
The study was published online in Diabetes Research and Clinical Practice.
Preexisting diabetic retinopathy and COVID-19 outcomes
The prevalence of diabetic retinopathy is thought to be around 55% in people with type 1 diabetes and 30% in people with type 2 diabetes, on average.
Dr. Karalliedde is part of a research group at King’s College London that has been focused on how vascular disease may predispose to more severe COVID-19.
“COVID-19 affects the blood vessels all over the body,” he said, so they wondered whether having preexisting retinopathy “would predispose to a severe manifestation of COVID-19.”
The observational study included 187 patients with diabetes (179 patients with type 2 diabetes and 8 patients with type 1 diabetes) hospitalized with COVID-19 at Guy’s and St Thomas’ NHS Foundation Trust between March 12 and April 7 (the peak of the first wave of the pandemic in the United Kingdom).
“It was an ethnically diverse population who were very sick and provides a clinical observation of real life,” Dr. Karalliedde said.
Nearly half of patients were African Caribbean (44%), 39% were White, and 17% were of other ethnicities, including 8% who were Asian. The mean age of the cohort was 68 years (range, 22-97 years), and 60% were men.
Diabetic retinopathy was reported in 67 (36%) patients, of whom 80% had background retinopathy and 20% had more advanced retinopathy.
They then looked at whether the presence of retinopathy was associated with a more severe manifestation of COVID-19 as defined by the need for tracheal intubation.
Of the 187 patients, 26% were intubated and 45% of these patients had diabetic retinopathy.
The analysis showed those with diabetic retinopathy had an over-fivefold increased risk for intubation (odds ratio, 5.81; 95% confidence interval, 1.37-24.66).
Of the entire cohort, 32% of patients died, although no association was observed between retinopathy and mortality.
“A greater number of diabetes patients with COVID-19 ended up on the intensive therapy unit. Upon multivariate analysis, we found retinopathy was independently associated with ending up on the intensive therapy unit,” stressed Dr. Karalliedde.
However, they noted that, “due to the cross-sectional design of our study, we cannot prove causality [between retinopathy and intubation]. Further studies are required to understand the mechanisms that explain the associations between retinopathy and other indices of microangiopathy with severe COVID-19.”
A version of this article originally appeared on Medscape.com.
COVID redefines curriculum for hospitalists-in-training
Pandemic brings ‘clarity and urgency’
The coronavirus pandemic has impacted all facets of the education and training of this country’s future hospitalists, including their medical school coursework, elective rotations, clerkships, and residency training – although with variations between settings and localities.
The COVID-19 crisis demanded immediate changes in traditional approaches to medical education. Training programs responded quickly to institute those changes. As hospitals geared up for potential surges in COVID cases starting in mid-March, many onsite training activities for medical students were shut down in order to reserve personal protective equipment for essential personnel and not put learners at risk of catching the virus. A variety of events related to their education were canceled. Didactic presentations and meetings were converted to virtual gatherings on internet platforms such as Zoom. Many of these changes were adopted even in settings with few actual COVID cases.
Medical students on clinical rotations were provided with virtual didactics when in-person clinical experiences were put on hold. In some cases, academic years ended early and fourth-year students graduated early so they might potentially join the hospital work force. Residents’ assignments were also changed, perhaps seeing patients on non–COVID-19 units only or taking different shifts, assignments, or rotations. Public health or research projects replaced elective placements. New electives were created, along with journal clubs, online care conferences, and technology-facilitated, self-directed learning.
But every advancing medical student needs to rotate through an experience of taking care of real patients, said Amy Guiot, MD, MEd, a hospitalist and associate director of medical student education in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center. “The Liaison Committee of Medical Education, jointly sponsored by the Association of American Medical Colleges and the American Medical Association, will not let you graduate a medical student without actual hands-on encounters with patients,” she explained.
For future doctors, especially those pursuing internal medicine – many of whom will practice as hospitalists – their training can’t duplicate “in the hospital” experiences except in the hospital, said Dr. Guiot, who is involved in pediatric training for medical students from the University of Cincinnati and residents.
For third- and fourth-year medical students, getting that personal contact with patients has been the hardest part, she added. But from March to May 2020, that experience was completely shut down at CCHMC, as at many medical schools, because of precautions aimed at preventing exposure to the novel coronavirus for both students and patients. That meant hospitals had to get creative, reshuffling schedules and the order of learning experiences; converting everything possible to virtual encounters on platforms such as Zoom; and reducing the length of rotations, the total number of in-person encounters, and the number of learners participating in an activity.
“We needed to use shift work for medical students, which hadn’t been done before,” Dr. Guiot said. Having students on different shifts, including nights, created more opportunities to fit clinical experiences into the schedule. The use of standardized patients – actors following a script who are examined by a student as part of learning how to do a physical exam – was also put on hold.
“Now we’re starting to get it back, but maybe not as often,” she said. “The actor wears a mask. The student wears a mask and shield. But it’s been harder for us to find actors – who tend to be older adults who may fear coming to the medical center – to perform their role, teaching medical students the art of examining a patient.”
Back to basics
The COVID-19 pandemic forced medical schools to get back to basics, figuring out the key competencies students needed to learn, said Alison Whelan, MD, AAMC’s chief medical education officer. Both medical schools and residency programs needed to respond quickly and in new ways, including with course content that would teach students about the virus and its management and treatment.

Schools have faced crises before, responding in real time to SARS (severe acute respiratory syndrome), Ebola, HIV, and natural disasters, Dr. Whelan said. “But there was a nimbleness and rapidity of adapting to COVID – with a lot of sharing of curriculums among medical colleges.” Back in late March, AAMC put out guidelines that recommended removing students from direct patient contact – not just for the student’s protection but for the community’s. A subsequent guidance, released Aug. 14, emphasized the need for medical schools to continue medical education – with appropriate attention to safety and local conditions while working closely with clinical partners.
Dr. Guiot, with her colleague Leslie Farrell, MD, and four very creative medical students, developed an online fourth-year elective course for University of Cincinnati medical students, offered asynchronously. It aimed to transmit a comprehensive understanding of COVID-19, its virology, transmission, clinical prevention, diagnosis and treatment, as well as examining national and international responses to the pandemic and their consequences and related issues of race, ethnicity, socioeconomic status, and health disparities. “We used several articles from the Journal of Hospital Medicine for students to read and discuss,” Dr. Guiot said.

Christopher Sankey, MD, SFHM, associate program director of the traditional internal medicine residency program and associate professor of medicine at Yale University, New Haven, Conn., oversees the inpatient educational experience for internal medicine residents at Yale. “As with most programs, there was a lot of trepidation as we made the transition from in-person to virtual education,” he said.
The two principal, non–ward-based educational opportunities for the Yale residents are morning report, which involves a case-based discussion of various medical issues, usually led by a chief resident, and noon conference, which is more didactic and content based. Both made the transition to virtual meetings for residents.
“We wondered, could these still be well-attended, well-liked, and successful learning experiences if offered virtually? What I found when I surveyed our residents was that the virtual conferences were not only well received, but actually preferred,” Dr. Sankey said. “We have a large campus with lots of internal medicine services, so it’s hard to assemble everyone for meetings. There were also situations in which there were so many residents that they couldn’t all fit into the same room.” Zoom, the virtual platform of choice, has actually increased attendance.

Marc Miller, MD, a pediatric hospitalist at the Cleveland Clinic, helped his team develop a virtual curriculum in pediatrics presented to third-year medical students during the month of May, when medical students were being taken off the wards. “Some third-year students still needed to get their pediatric clerkships done. We had to balance clinical exposure with a lot of other things,” he explained.
The curriculum included a focus on interprofessional aspects of interdisciplinary, family-centered bedside rounds; a COVID literature review; and a lot of case-based scenarios. “Most challenging was how to remake family rounds. We tried to incorporate students into table rounds, but that didn’t feel as valuable,” Dr. Miller said. “Because pediatrics is so family centered, talking to patients and families at the bedside is highly valued. So we had virtual sessions talking about how to do that, with videos to illustrate it put out by Cincinnati Children’s Hospital.”
The most interactive sessions got the best feedback, but all the sessions went over very well, Dr. Miller said. “Larger lessons from COVID include things we already knew, but now with extra importance, such as the need to encourage interactivity to get students to buy in and take part in these conversations – whatever the structure.”

Vineet Arora, MD, MHM, an academic hospitalist and chief medical officer for the clinical learning environment at the University of Chicago, said that the changes wrought by COVID have also produced unexpected gains for medical education. “We’ve also had to think differently and more creatively about how to get the same information across in this new environment,” she explained. “In some cases, we saw that it was easier for learners to attend conferences and meetings online, with increased attendance for our events.” That includes participation on quality improvement committees, and attending online medical conferences presented locally and regionally.
“Another question: How do we teach interdisciplinary rounds and how to work with other members of the team without having face-to-face interactions?” Dr. Arora said. “Our old interdisciplinary rounding model had to change. It forced us to rethink how to create that kind of learning. We can’t have as many people in the patient’s room at one time. Can there be a physically distanced ‘touch-base’ with the nurse outside the patient’s room after a doctor has gone in to meet the patient?”
Transformational change
In a recent JAMA Viewpoint column, Catherine R. Lucey, MD, and S. Claiborne Johnston, MD, PhD,1 called the impact of COVID-19 “transformational,” in line with changes in medical curriculums recommended by the 2010 Global Independent Commission on Education of Health Professionals for the 21st Century,2 which asserted that the purpose of professional education is to improve the health of communities.
The authors stated that COVID-19 brought clarity and urgency to this purpose, and will someday be viewed as a catalyst for the needed transformation of medical education as medical schools embarked on curriculum redesign to embrace new competencies for current health challenges.
They suggested that medical students not only continued to learn during the COVID crisis “but in many circumstances, accelerated their attainment of the types of competencies that 21st century physicians must master.” Emerging competencies identified by Dr. Lucey and Dr. Johnston include:
- Being able to address population and public health issues
- Designing and continuously improving of the health care system
- Incorporating data and technology in service to patient care, research, and education
- Eliminating health care disparities and discrimination in medicine
- Adapting the curriculum to current issues in real-time
- Engaging in crisis communication and active change leadership
How is the curriculum changing? It’s still a work in progress. “After the disruptions of the spring and summer, schools are now trying to figure which of the changes should stay,” said Dr. Whelan. “The virus has also highlighted other crises, with social determinants of health and racial disparities becoming more front and center. In terms of content, medical educators are rethinking a lot of things – in a good way.”
Another important trend cast in sharper relief by the pandemic is a gradual evolution toward competency-based education and how to assess when someone is ready to be a doctor, Dr. Whelan said. “There’s been an accelerated consideration of how to be sure each student is competent to practice medicine.”3
Many practicing physicians and students were redeployed in the crisis, she said. Pediatric physicians were asked to take care of adult patients, and internists were drafted to work in the ICU. Hospitals quickly developed refresher courses and competency-based assessments to facilitate these redeployments. What can be learned from such on-the-fly assessments? What was needed to make a pediatrician, under the supervision of an internist, able to take good care of adult patients?
And does competency-based assessment point toward some kind of time-variable graduate medical education of the future – with graduation when the competencies are achieved, rather than just tethered to time- and case volume–based requirements? It seems Canada is moving in this direction, and COVID might catalyze a similar transformation in the United States.3
Changing the curriculum
Does the content of the curriculum for preparing future hospitalists need to change significantly? “My honest answer is yes and no,” Dr. Sankey said. “One thing we found in our training program is that it’s possible to become consumed by this pandemic. We need to educate residents about it, but future doctors still need to learn a lot of other things. Heart failure has not gone away.
“It’s okay to stick to the general curriculum, but with a wider variety of learning opportunities. Adding content sessions on population health, social determinants of health, race and bias, and equity is a start, but it’s by no means sufficient to give these topics the importance they deserve. We need to interpolate these subjects into sessions we’re already doing,” he said. “It is not enough to do a couple of lectures on diversity. We need to weave these concepts into the education we provide for residents every day.
“I think the pandemic has posed an opportunity to critically consider what’s the ideal teaching and learning environment. How can we make it better? Societal events around race have demonstrated essential areas for curricular development, and the pandemic had us primed and already thinking about how we educate future doctors – both in terms of medium and content,” he said.
Some medical schools started their new academic year in July; others put it off until September. Patient care at CCHMC is nearly back to where it used to be before COVID-19 began, Dr. Guiot said in a September interview, “but in masks and goggles.” As a result, hospitals are having to get creative all over again to accommodate medical students.
“I am amazed at the camaraderie of hospitals and medical schools, trying to support our learners in the midst of the pandemic,” she said. “I learned that we can be more adaptive than I ever imagined. We were all nervous about the risks, but we learned how to support each other and still provide excellent care in the midst of the pandemic. We’re forever changed. We also learned how to present didactics on Zoom, but that was the easy part.”
References
1. Lucey CR, Johnston SC. The transformational effects of COVID-19 on medical education. JAMA. 2020;324(11):1033-4.
2. Bhutta ZA et al. Education of health professionals for the 21st century: A global independent Commission. Lancet. 2010 Apr 3;375(9721):1137-8.
3. Goldhamer MEJ et al. Can COVID catalyze an educational transformation? Competency-based advancement in a crisis. N Engl J Med. 2020;383:1003-5.
Pandemic brings ‘clarity and urgency’
Pandemic brings ‘clarity and urgency’
The coronavirus pandemic has impacted all facets of the education and training of this country’s future hospitalists, including their medical school coursework, elective rotations, clerkships, and residency training – although with variations between settings and localities.
The COVID-19 crisis demanded immediate changes in traditional approaches to medical education. Training programs responded quickly to institute those changes. As hospitals geared up for potential surges in COVID cases starting in mid-March, many onsite training activities for medical students were shut down in order to reserve personal protective equipment for essential personnel and not put learners at risk of catching the virus. A variety of events related to their education were canceled. Didactic presentations and meetings were converted to virtual gatherings on internet platforms such as Zoom. Many of these changes were adopted even in settings with few actual COVID cases.
Medical students on clinical rotations were provided with virtual didactics when in-person clinical experiences were put on hold. In some cases, academic years ended early and fourth-year students graduated early so they might potentially join the hospital work force. Residents’ assignments were also changed, perhaps seeing patients on non–COVID-19 units only or taking different shifts, assignments, or rotations. Public health or research projects replaced elective placements. New electives were created, along with journal clubs, online care conferences, and technology-facilitated, self-directed learning.
But every advancing medical student needs to rotate through an experience of taking care of real patients, said Amy Guiot, MD, MEd, a hospitalist and associate director of medical student education in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center. “The Liaison Committee of Medical Education, jointly sponsored by the Association of American Medical Colleges and the American Medical Association, will not let you graduate a medical student without actual hands-on encounters with patients,” she explained.
For future doctors, especially those pursuing internal medicine – many of whom will practice as hospitalists – their training can’t duplicate “in the hospital” experiences except in the hospital, said Dr. Guiot, who is involved in pediatric training for medical students from the University of Cincinnati and residents.
For third- and fourth-year medical students, getting that personal contact with patients has been the hardest part, she added. But from March to May 2020, that experience was completely shut down at CCHMC, as at many medical schools, because of precautions aimed at preventing exposure to the novel coronavirus for both students and patients. That meant hospitals had to get creative, reshuffling schedules and the order of learning experiences; converting everything possible to virtual encounters on platforms such as Zoom; and reducing the length of rotations, the total number of in-person encounters, and the number of learners participating in an activity.
“We needed to use shift work for medical students, which hadn’t been done before,” Dr. Guiot said. Having students on different shifts, including nights, created more opportunities to fit clinical experiences into the schedule. The use of standardized patients – actors following a script who are examined by a student as part of learning how to do a physical exam – was also put on hold.
“Now we’re starting to get it back, but maybe not as often,” she said. “The actor wears a mask. The student wears a mask and shield. But it’s been harder for us to find actors – who tend to be older adults who may fear coming to the medical center – to perform their role, teaching medical students the art of examining a patient.”
Back to basics
The COVID-19 pandemic forced medical schools to get back to basics, figuring out the key competencies students needed to learn, said Alison Whelan, MD, AAMC’s chief medical education officer. Both medical schools and residency programs needed to respond quickly and in new ways, including with course content that would teach students about the virus and its management and treatment.
Schools have faced crises before, responding in real time to SARS (severe acute respiratory syndrome), Ebola, HIV, and natural disasters, Dr. Whelan said. “But there was a nimbleness and rapidity of adapting to COVID – with a lot of sharing of curriculums among medical colleges.” Back in late March, AAMC put out guidelines that recommended removing students from direct patient contact – not just for the student’s protection but for the community’s. A subsequent guidance, released Aug. 14, emphasized the need for medical schools to continue medical education – with appropriate attention to safety and local conditions while working closely with clinical partners.
Dr. Guiot, with her colleague Leslie Farrell, MD, and four very creative medical students, developed an online fourth-year elective course for University of Cincinnati medical students, offered asynchronously. It aimed to transmit a comprehensive understanding of COVID-19, its virology, transmission, clinical prevention, diagnosis and treatment, as well as examining national and international responses to the pandemic and their consequences and related issues of race, ethnicity, socioeconomic status, and health disparities. “We used several articles from the Journal of Hospital Medicine for students to read and discuss,” Dr. Guiot said.
Christopher Sankey, MD, SFHM, associate program director of the traditional internal medicine residency program and associate professor of medicine at Yale University, New Haven, Conn., oversees the inpatient educational experience for internal medicine residents at Yale. “As with most programs, there was a lot of trepidation as we made the transition from in-person to virtual education,” he said.
The two principal, non–ward-based educational opportunities for the Yale residents are morning report, which involves a case-based discussion of various medical issues, usually led by a chief resident, and noon conference, which is more didactic and content based. Both made the transition to virtual meetings for residents.
“We wondered, could these still be well-attended, well-liked, and successful learning experiences if offered virtually? What I found when I surveyed our residents was that the virtual conferences were not only well received, but actually preferred,” Dr. Sankey said. “We have a large campus with lots of internal medicine services, so it’s hard to assemble everyone for meetings. There were also situations in which there were so many residents that they couldn’t all fit into the same room.” Zoom, the virtual platform of choice, has actually increased attendance.
Marc Miller, MD, a pediatric hospitalist at the Cleveland Clinic, helped his team develop a virtual curriculum in pediatrics presented to third-year medical students during the month of May, when medical students were being taken off the wards. “Some third-year students still needed to get their pediatric clerkships done. We had to balance clinical exposure with a lot of other things,” he explained.
The curriculum included a focus on interprofessional aspects of interdisciplinary, family-centered bedside rounds; a COVID literature review; and a lot of case-based scenarios. “Most challenging was how to remake family rounds. We tried to incorporate students into table rounds, but that didn’t feel as valuable,” Dr. Miller said. “Because pediatrics is so family centered, talking to patients and families at the bedside is highly valued. So we had virtual sessions talking about how to do that, with videos to illustrate it put out by Cincinnati Children’s Hospital.”
The most interactive sessions got the best feedback, but all the sessions went over very well, Dr. Miller said. “Larger lessons from COVID include things we already knew, but now with extra importance, such as the need to encourage interactivity to get students to buy in and take part in these conversations – whatever the structure.”
Vineet Arora, MD, MHM, an academic hospitalist and chief medical officer for the clinical learning environment at the University of Chicago, said that the changes wrought by COVID have also produced unexpected gains for medical education. “We’ve also had to think differently and more creatively about how to get the same information across in this new environment,” she explained. “In some cases, we saw that it was easier for learners to attend conferences and meetings online, with increased attendance for our events.” That includes participation on quality improvement committees, and attending online medical conferences presented locally and regionally.
“Another question: How do we teach interdisciplinary rounds and how to work with other members of the team without having face-to-face interactions?” Dr. Arora said. “Our old interdisciplinary rounding model had to change. It forced us to rethink how to create that kind of learning. We can’t have as many people in the patient’s room at one time. Can there be a physically distanced ‘touch-base’ with the nurse outside the patient’s room after a doctor has gone in to meet the patient?”
Transformational change
In a recent JAMA Viewpoint column, Catherine R. Lucey, MD, and S. Claiborne Johnston, MD, PhD,1 called the impact of COVID-19 “transformational,” in line with changes in medical curriculums recommended by the 2010 Global Independent Commission on Education of Health Professionals for the 21st Century,2 which asserted that the purpose of professional education is to improve the health of communities.
The authors stated that COVID-19 brought clarity and urgency to this purpose, and will someday be viewed as a catalyst for the needed transformation of medical education as medical schools embarked on curriculum redesign to embrace new competencies for current health challenges.
They suggested that medical students not only continued to learn during the COVID crisis “but in many circumstances, accelerated their attainment of the types of competencies that 21st century physicians must master.” Emerging competencies identified by Dr. Lucey and Dr. Johnston include:
- Being able to address population and public health issues
- Designing and continuously improving of the health care system
- Incorporating data and technology in service to patient care, research, and education
- Eliminating health care disparities and discrimination in medicine
- Adapting the curriculum to current issues in real-time
- Engaging in crisis communication and active change leadership
How is the curriculum changing? It’s still a work in progress. “After the disruptions of the spring and summer, schools are now trying to figure which of the changes should stay,” said Dr. Whelan. “The virus has also highlighted other crises, with social determinants of health and racial disparities becoming more front and center. In terms of content, medical educators are rethinking a lot of things – in a good way.”
Another important trend cast in sharper relief by the pandemic is a gradual evolution toward competency-based education and how to assess when someone is ready to be a doctor, Dr. Whelan said. “There’s been an accelerated consideration of how to be sure each student is competent to practice medicine.”3
Many practicing physicians and students were redeployed in the crisis, she said. Pediatric physicians were asked to take care of adult patients, and internists were drafted to work in the ICU. Hospitals quickly developed refresher courses and competency-based assessments to facilitate these redeployments. What can be learned from such on-the-fly assessments? What was needed to make a pediatrician, under the supervision of an internist, able to take good care of adult patients?
And does competency-based assessment point toward some kind of time-variable graduate medical education of the future – with graduation when the competencies are achieved, rather than just tethered to time- and case volume–based requirements? It seems Canada is moving in this direction, and COVID might catalyze a similar transformation in the United States.3
Changing the curriculum
Does the content of the curriculum for preparing future hospitalists need to change significantly? “My honest answer is yes and no,” Dr. Sankey said. “One thing we found in our training program is that it’s possible to become consumed by this pandemic. We need to educate residents about it, but future doctors still need to learn a lot of other things. Heart failure has not gone away.
“It’s okay to stick to the general curriculum, but with a wider variety of learning opportunities. Adding content sessions on population health, social determinants of health, race and bias, and equity is a start, but it’s by no means sufficient to give these topics the importance they deserve. We need to interpolate these subjects into sessions we’re already doing,” he said. “It is not enough to do a couple of lectures on diversity. We need to weave these concepts into the education we provide for residents every day.
“I think the pandemic has posed an opportunity to critically consider what’s the ideal teaching and learning environment. How can we make it better? Societal events around race have demonstrated essential areas for curricular development, and the pandemic had us primed and already thinking about how we educate future doctors – both in terms of medium and content,” he said.
Some medical schools started their new academic year in July; others put it off until September. Patient care at CCHMC is nearly back to where it used to be before COVID-19 began, Dr. Guiot said in a September interview, “but in masks and goggles.” As a result, hospitals are having to get creative all over again to accommodate medical students.
“I am amazed at the camaraderie of hospitals and medical schools, trying to support our learners in the midst of the pandemic,” she said. “I learned that we can be more adaptive than I ever imagined. We were all nervous about the risks, but we learned how to support each other and still provide excellent care in the midst of the pandemic. We’re forever changed. We also learned how to present didactics on Zoom, but that was the easy part.”
References
1. Lucey CR, Johnston SC. The transformational effects of COVID-19 on medical education. JAMA. 2020;324(11):1033-4.
2. Bhutta ZA et al. Education of health professionals for the 21st century: A global independent Commission. Lancet. 2010 Apr 3;375(9721):1137-8.
3. Goldhamer MEJ et al. Can COVID catalyze an educational transformation? Competency-based advancement in a crisis. N Engl J Med. 2020;383:1003-5.
The coronavirus pandemic has impacted all facets of the education and training of this country’s future hospitalists, including their medical school coursework, elective rotations, clerkships, and residency training – although with variations between settings and localities.
The COVID-19 crisis demanded immediate changes in traditional approaches to medical education. Training programs responded quickly to institute those changes. As hospitals geared up for potential surges in COVID cases starting in mid-March, many onsite training activities for medical students were shut down in order to reserve personal protective equipment for essential personnel and not put learners at risk of catching the virus. A variety of events related to their education were canceled. Didactic presentations and meetings were converted to virtual gatherings on internet platforms such as Zoom. Many of these changes were adopted even in settings with few actual COVID cases.
Medical students on clinical rotations were provided with virtual didactics when in-person clinical experiences were put on hold. In some cases, academic years ended early and fourth-year students graduated early so they might potentially join the hospital work force. Residents’ assignments were also changed, perhaps seeing patients on non–COVID-19 units only or taking different shifts, assignments, or rotations. Public health or research projects replaced elective placements. New electives were created, along with journal clubs, online care conferences, and technology-facilitated, self-directed learning.
But every advancing medical student needs to rotate through an experience of taking care of real patients, said Amy Guiot, MD, MEd, a hospitalist and associate director of medical student education in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center. “The Liaison Committee of Medical Education, jointly sponsored by the Association of American Medical Colleges and the American Medical Association, will not let you graduate a medical student without actual hands-on encounters with patients,” she explained.
For future doctors, especially those pursuing internal medicine – many of whom will practice as hospitalists – their training can’t duplicate “in the hospital” experiences except in the hospital, said Dr. Guiot, who is involved in pediatric training for medical students from the University of Cincinnati and residents.
For third- and fourth-year medical students, getting that personal contact with patients has been the hardest part, she added. But from March to May 2020, that experience was completely shut down at CCHMC, as at many medical schools, because of precautions aimed at preventing exposure to the novel coronavirus for both students and patients. That meant hospitals had to get creative, reshuffling schedules and the order of learning experiences; converting everything possible to virtual encounters on platforms such as Zoom; and reducing the length of rotations, the total number of in-person encounters, and the number of learners participating in an activity.
“We needed to use shift work for medical students, which hadn’t been done before,” Dr. Guiot said. Having students on different shifts, including nights, created more opportunities to fit clinical experiences into the schedule. The use of standardized patients – actors following a script who are examined by a student as part of learning how to do a physical exam – was also put on hold.
“Now we’re starting to get it back, but maybe not as often,” she said. “The actor wears a mask. The student wears a mask and shield. But it’s been harder for us to find actors – who tend to be older adults who may fear coming to the medical center – to perform their role, teaching medical students the art of examining a patient.”
Back to basics
The COVID-19 pandemic forced medical schools to get back to basics, figuring out the key competencies students needed to learn, said Alison Whelan, MD, AAMC’s chief medical education officer. Both medical schools and residency programs needed to respond quickly and in new ways, including with course content that would teach students about the virus and its management and treatment.
Schools have faced crises before, responding in real time to SARS (severe acute respiratory syndrome), Ebola, HIV, and natural disasters, Dr. Whelan said. “But there was a nimbleness and rapidity of adapting to COVID – with a lot of sharing of curriculums among medical colleges.” Back in late March, AAMC put out guidelines that recommended removing students from direct patient contact – not just for the student’s protection but for the community’s. A subsequent guidance, released Aug. 14, emphasized the need for medical schools to continue medical education – with appropriate attention to safety and local conditions while working closely with clinical partners.
Dr. Guiot, with her colleague Leslie Farrell, MD, and four very creative medical students, developed an online fourth-year elective course for University of Cincinnati medical students, offered asynchronously. It aimed to transmit a comprehensive understanding of COVID-19, its virology, transmission, clinical prevention, diagnosis and treatment, as well as examining national and international responses to the pandemic and their consequences and related issues of race, ethnicity, socioeconomic status, and health disparities. “We used several articles from the Journal of Hospital Medicine for students to read and discuss,” Dr. Guiot said.
Christopher Sankey, MD, SFHM, associate program director of the traditional internal medicine residency program and associate professor of medicine at Yale University, New Haven, Conn., oversees the inpatient educational experience for internal medicine residents at Yale. “As with most programs, there was a lot of trepidation as we made the transition from in-person to virtual education,” he said.
The two principal, non–ward-based educational opportunities for the Yale residents are morning report, which involves a case-based discussion of various medical issues, usually led by a chief resident, and noon conference, which is more didactic and content based. Both made the transition to virtual meetings for residents.
“We wondered, could these still be well-attended, well-liked, and successful learning experiences if offered virtually? What I found when I surveyed our residents was that the virtual conferences were not only well received, but actually preferred,” Dr. Sankey said. “We have a large campus with lots of internal medicine services, so it’s hard to assemble everyone for meetings. There were also situations in which there were so many residents that they couldn’t all fit into the same room.” Zoom, the virtual platform of choice, has actually increased attendance.
Marc Miller, MD, a pediatric hospitalist at the Cleveland Clinic, helped his team develop a virtual curriculum in pediatrics presented to third-year medical students during the month of May, when medical students were being taken off the wards. “Some third-year students still needed to get their pediatric clerkships done. We had to balance clinical exposure with a lot of other things,” he explained.
The curriculum included a focus on interprofessional aspects of interdisciplinary, family-centered bedside rounds; a COVID literature review; and a lot of case-based scenarios. “Most challenging was how to remake family rounds. We tried to incorporate students into table rounds, but that didn’t feel as valuable,” Dr. Miller said. “Because pediatrics is so family centered, talking to patients and families at the bedside is highly valued. So we had virtual sessions talking about how to do that, with videos to illustrate it put out by Cincinnati Children’s Hospital.”
The most interactive sessions got the best feedback, but all the sessions went over very well, Dr. Miller said. “Larger lessons from COVID include things we already knew, but now with extra importance, such as the need to encourage interactivity to get students to buy in and take part in these conversations – whatever the structure.”
Vineet Arora, MD, MHM, an academic hospitalist and chief medical officer for the clinical learning environment at the University of Chicago, said that the changes wrought by COVID have also produced unexpected gains for medical education. “We’ve also had to think differently and more creatively about how to get the same information across in this new environment,” she explained. “In some cases, we saw that it was easier for learners to attend conferences and meetings online, with increased attendance for our events.” That includes participation on quality improvement committees, and attending online medical conferences presented locally and regionally.
“Another question: How do we teach interdisciplinary rounds and how to work with other members of the team without having face-to-face interactions?” Dr. Arora said. “Our old interdisciplinary rounding model had to change. It forced us to rethink how to create that kind of learning. We can’t have as many people in the patient’s room at one time. Can there be a physically distanced ‘touch-base’ with the nurse outside the patient’s room after a doctor has gone in to meet the patient?”
Transformational change
In a recent JAMA Viewpoint column, Catherine R. Lucey, MD, and S. Claiborne Johnston, MD, PhD,1 called the impact of COVID-19 “transformational,” in line with changes in medical curriculums recommended by the 2010 Global Independent Commission on Education of Health Professionals for the 21st Century,2 which asserted that the purpose of professional education is to improve the health of communities.
The authors stated that COVID-19 brought clarity and urgency to this purpose, and will someday be viewed as a catalyst for the needed transformation of medical education as medical schools embarked on curriculum redesign to embrace new competencies for current health challenges.
They suggested that medical students not only continued to learn during the COVID crisis “but in many circumstances, accelerated their attainment of the types of competencies that 21st century physicians must master.” Emerging competencies identified by Dr. Lucey and Dr. Johnston include:
- Being able to address population and public health issues
- Designing and continuously improving of the health care system
- Incorporating data and technology in service to patient care, research, and education
- Eliminating health care disparities and discrimination in medicine
- Adapting the curriculum to current issues in real-time
- Engaging in crisis communication and active change leadership
How is the curriculum changing? It’s still a work in progress. “After the disruptions of the spring and summer, schools are now trying to figure which of the changes should stay,” said Dr. Whelan. “The virus has also highlighted other crises, with social determinants of health and racial disparities becoming more front and center. In terms of content, medical educators are rethinking a lot of things – in a good way.”
Another important trend cast in sharper relief by the pandemic is a gradual evolution toward competency-based education and how to assess when someone is ready to be a doctor, Dr. Whelan said. “There’s been an accelerated consideration of how to be sure each student is competent to practice medicine.”3
Many practicing physicians and students were redeployed in the crisis, she said. Pediatric physicians were asked to take care of adult patients, and internists were drafted to work in the ICU. Hospitals quickly developed refresher courses and competency-based assessments to facilitate these redeployments. What can be learned from such on-the-fly assessments? What was needed to make a pediatrician, under the supervision of an internist, able to take good care of adult patients?
And does competency-based assessment point toward some kind of time-variable graduate medical education of the future – with graduation when the competencies are achieved, rather than just tethered to time- and case volume–based requirements? It seems Canada is moving in this direction, and COVID might catalyze a similar transformation in the United States.3
Changing the curriculum
Does the content of the curriculum for preparing future hospitalists need to change significantly? “My honest answer is yes and no,” Dr. Sankey said. “One thing we found in our training program is that it’s possible to become consumed by this pandemic. We need to educate residents about it, but future doctors still need to learn a lot of other things. Heart failure has not gone away.
“It’s okay to stick to the general curriculum, but with a wider variety of learning opportunities. Adding content sessions on population health, social determinants of health, race and bias, and equity is a start, but it’s by no means sufficient to give these topics the importance they deserve. We need to interpolate these subjects into sessions we’re already doing,” he said. “It is not enough to do a couple of lectures on diversity. We need to weave these concepts into the education we provide for residents every day.
“I think the pandemic has posed an opportunity to critically consider what’s the ideal teaching and learning environment. How can we make it better? Societal events around race have demonstrated essential areas for curricular development, and the pandemic had us primed and already thinking about how we educate future doctors – both in terms of medium and content,” he said.
Some medical schools started their new academic year in July; others put it off until September. Patient care at CCHMC is nearly back to where it used to be before COVID-19 began, Dr. Guiot said in a September interview, “but in masks and goggles.” As a result, hospitals are having to get creative all over again to accommodate medical students.
“I am amazed at the camaraderie of hospitals and medical schools, trying to support our learners in the midst of the pandemic,” she said. “I learned that we can be more adaptive than I ever imagined. We were all nervous about the risks, but we learned how to support each other and still provide excellent care in the midst of the pandemic. We’re forever changed. We also learned how to present didactics on Zoom, but that was the easy part.”
References
1. Lucey CR, Johnston SC. The transformational effects of COVID-19 on medical education. JAMA. 2020;324(11):1033-4.
2. Bhutta ZA et al. Education of health professionals for the 21st century: A global independent Commission. Lancet. 2010 Apr 3;375(9721):1137-8.
3. Goldhamer MEJ et al. Can COVID catalyze an educational transformation? Competency-based advancement in a crisis. N Engl J Med. 2020;383:1003-5.
How Twitter amplifies my doctor and human voice
When I graduated from residency in 2007, Facebook had just become “a thing,” and my cohort decided to use it to keep in touch. These days, Twitter seems to be the social media platform of choice for health care professionals.

When I started on Twitter a few years ago, it was in reaction to the current political climate. I wanted to keep track of what my favorite thinkers were writing. I was anonymous and tweeted about politics mostly. My husband was my only follower for a while.
I deanonymized when, at last year’s American College of Rheumatology meeting, I presented a poster and wanted to reach a wider audience. I could have created two different personas on Twitter, like many doctors apparently do. Initially, I resisted doing that because I am frankly too lazy to keep track of two different social media profiles, but now I resist because I see my profession as an extension of my political self, and have no problem with using my (very low) profile to amplify both my doctor voice and my human voice.
Professionally, Twitter is rewarding. It is a space for networking and for promoting one’s work. It is a fantastic learning format, as evidenced by the popularity of tweetorials. The international consortium that has worked to collect information on rheumatology patients with COVID started as an idea on Twitter. The fact that ACR Convergence 2020 abstracts are now available? I only know because of the #ACRambassadors that I follow.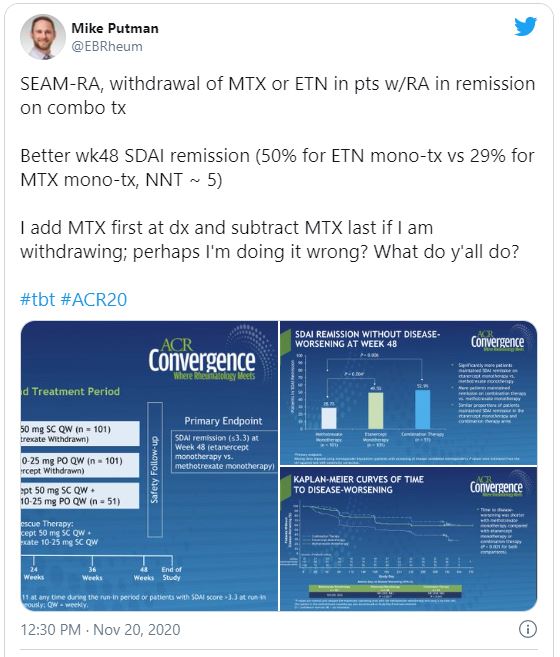
But I find that I cannot separate who I am from what I do. As a rheumatologist, I build long-term relationships with patients. I cannot care for their medical conditions in isolation without also concerning myself with their nonmedical circumstances. For that reason, I have opinions that one might call humanist, and I suspect that I am not alone among rheumatologists.
I can think of three areas, broadly construed but with huge overlaps, that concern me a great deal.
First, there are things that affect all physicians: race and gender discrimination in the workplace; advancement of women in science, technology, engineering, or math; Medicare reimbursement; COVID-19 preparedness; immigration issues (an issue near and dear to me, as I am an immigrant and a foreign medical graduate); and federal funding (including funding for training programs and community health centers, funding for the National Institutes of Health, and funding for stem cell research).
Then there are the things that affect rheumatologists in particular. Access to medications and procedures is one thing. (I did say these categories hugely overlap.) If you›ve ever tried to prescribe even a drug as old as oral cyclophosphamide, you’ll have experienced the difficulty of getting it for Medicare patients. Patients who need biologics are limited by insurance contracts with pharmaceutical companies, but also by requirements such as step therapy. I am all varieties of annoyed, incredulous, and apologetic that when a patient asks me how much a treatment will cost him/her, I do not have an answer.
Speaking of pricing, don’t even get me started on pharmaceutical company price gouging. Yes, the H.P. Acthar gel may be the most egregious offender among rheumatology medications, but it’s easy to not prescribe a drug that costs $80,000 a vial and which does not do much more than prednisone does. On the other hand, I remember a time when colchicine cost $0.10 cents a pill and patients did not have to jump through hoops to get it.
And what of reproductive freedom? Our patients rely on us for advice about their childbearing options, including birth control, in vitro fertilization, and pregnancy termination.
Finally, and most important, the things that affect me most are the issues that affect patients. The lowest-hanging fruit here is the abject incompetence of the federal response to the ongoing pandemic. How many of our patients’ lives have been lost or adversely affected? And what of coverage for preexisting conditions for the vast majority of our patients, whose illnesses are chronic?
While we’re at it, the fact of health insurance being tied to employment, something that seemingly no other country in the developed world does, makes living with chronic conditions outright scary, doesn’t it? It isn’t quite so easy to remain employed when one cannot get the right medications for RA.
I could go on. Gun violence and health care disparities, vaccine denialism, coverage for mental health issues, LGBTQ rights, refugee rights, police brutality … there is a seemingly endless list of things to care about. It’s exhausting.
While I do use my Twitter account to learn from colleagues and to promote work that interests me, my primary aim is to participate in civil society as a person. Critics will use “stay in your lane” as shorthand to say x professionals should stick to x (actors to acting, musicians to music, athletes to sports). If only I could. But my humanity won’t let me. Aristotle said man is a political animal; even the venerable New England Journal of Medicine has found it impossible to keep silent.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medicine, New York, and an attending physician at the Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center, both in New York. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a past columnist for MDedge Rheumatology, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com.
When I graduated from residency in 2007, Facebook had just become “a thing,” and my cohort decided to use it to keep in touch. These days, Twitter seems to be the social media platform of choice for health care professionals.
When I started on Twitter a few years ago, it was in reaction to the current political climate. I wanted to keep track of what my favorite thinkers were writing. I was anonymous and tweeted about politics mostly. My husband was my only follower for a while.
I deanonymized when, at last year’s American College of Rheumatology meeting, I presented a poster and wanted to reach a wider audience. I could have created two different personas on Twitter, like many doctors apparently do. Initially, I resisted doing that because I am frankly too lazy to keep track of two different social media profiles, but now I resist because I see my profession as an extension of my political self, and have no problem with using my (very low) profile to amplify both my doctor voice and my human voice.
Professionally, Twitter is rewarding. It is a space for networking and for promoting one’s work. It is a fantastic learning format, as evidenced by the popularity of tweetorials. The international consortium that has worked to collect information on rheumatology patients with COVID started as an idea on Twitter. The fact that ACR Convergence 2020 abstracts are now available? I only know because of the #ACRambassadors that I follow.
But I find that I cannot separate who I am from what I do. As a rheumatologist, I build long-term relationships with patients. I cannot care for their medical conditions in isolation without also concerning myself with their nonmedical circumstances. For that reason, I have opinions that one might call humanist, and I suspect that I am not alone among rheumatologists.
I can think of three areas, broadly construed but with huge overlaps, that concern me a great deal.
First, there are things that affect all physicians: race and gender discrimination in the workplace; advancement of women in science, technology, engineering, or math; Medicare reimbursement; COVID-19 preparedness; immigration issues (an issue near and dear to me, as I am an immigrant and a foreign medical graduate); and federal funding (including funding for training programs and community health centers, funding for the National Institutes of Health, and funding for stem cell research).
Then there are the things that affect rheumatologists in particular. Access to medications and procedures is one thing. (I did say these categories hugely overlap.) If you›ve ever tried to prescribe even a drug as old as oral cyclophosphamide, you’ll have experienced the difficulty of getting it for Medicare patients. Patients who need biologics are limited by insurance contracts with pharmaceutical companies, but also by requirements such as step therapy. I am all varieties of annoyed, incredulous, and apologetic that when a patient asks me how much a treatment will cost him/her, I do not have an answer.
Speaking of pricing, don’t even get me started on pharmaceutical company price gouging. Yes, the H.P. Acthar gel may be the most egregious offender among rheumatology medications, but it’s easy to not prescribe a drug that costs $80,000 a vial and which does not do much more than prednisone does. On the other hand, I remember a time when colchicine cost $0.10 cents a pill and patients did not have to jump through hoops to get it.
And what of reproductive freedom? Our patients rely on us for advice about their childbearing options, including birth control, in vitro fertilization, and pregnancy termination.
Finally, and most important, the things that affect me most are the issues that affect patients. The lowest-hanging fruit here is the abject incompetence of the federal response to the ongoing pandemic. How many of our patients’ lives have been lost or adversely affected? And what of coverage for preexisting conditions for the vast majority of our patients, whose illnesses are chronic?
While we’re at it, the fact of health insurance being tied to employment, something that seemingly no other country in the developed world does, makes living with chronic conditions outright scary, doesn’t it? It isn’t quite so easy to remain employed when one cannot get the right medications for RA.
I could go on. Gun violence and health care disparities, vaccine denialism, coverage for mental health issues, LGBTQ rights, refugee rights, police brutality … there is a seemingly endless list of things to care about. It’s exhausting.
While I do use my Twitter account to learn from colleagues and to promote work that interests me, my primary aim is to participate in civil society as a person. Critics will use “stay in your lane” as shorthand to say x professionals should stick to x (actors to acting, musicians to music, athletes to sports). If only I could. But my humanity won’t let me. Aristotle said man is a political animal; even the venerable New England Journal of Medicine has found it impossible to keep silent.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medicine, New York, and an attending physician at the Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center, both in New York. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a past columnist for MDedge Rheumatology, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com.
When I graduated from residency in 2007, Facebook had just become “a thing,” and my cohort decided to use it to keep in touch. These days, Twitter seems to be the social media platform of choice for health care professionals.
When I started on Twitter a few years ago, it was in reaction to the current political climate. I wanted to keep track of what my favorite thinkers were writing. I was anonymous and tweeted about politics mostly. My husband was my only follower for a while.
I deanonymized when, at last year’s American College of Rheumatology meeting, I presented a poster and wanted to reach a wider audience. I could have created two different personas on Twitter, like many doctors apparently do. Initially, I resisted doing that because I am frankly too lazy to keep track of two different social media profiles, but now I resist because I see my profession as an extension of my political self, and have no problem with using my (very low) profile to amplify both my doctor voice and my human voice.
Professionally, Twitter is rewarding. It is a space for networking and for promoting one’s work. It is a fantastic learning format, as evidenced by the popularity of tweetorials. The international consortium that has worked to collect information on rheumatology patients with COVID started as an idea on Twitter. The fact that ACR Convergence 2020 abstracts are now available? I only know because of the #ACRambassadors that I follow.
But I find that I cannot separate who I am from what I do. As a rheumatologist, I build long-term relationships with patients. I cannot care for their medical conditions in isolation without also concerning myself with their nonmedical circumstances. For that reason, I have opinions that one might call humanist, and I suspect that I am not alone among rheumatologists.
I can think of three areas, broadly construed but with huge overlaps, that concern me a great deal.
First, there are things that affect all physicians: race and gender discrimination in the workplace; advancement of women in science, technology, engineering, or math; Medicare reimbursement; COVID-19 preparedness; immigration issues (an issue near and dear to me, as I am an immigrant and a foreign medical graduate); and federal funding (including funding for training programs and community health centers, funding for the National Institutes of Health, and funding for stem cell research).
Then there are the things that affect rheumatologists in particular. Access to medications and procedures is one thing. (I did say these categories hugely overlap.) If you›ve ever tried to prescribe even a drug as old as oral cyclophosphamide, you’ll have experienced the difficulty of getting it for Medicare patients. Patients who need biologics are limited by insurance contracts with pharmaceutical companies, but also by requirements such as step therapy. I am all varieties of annoyed, incredulous, and apologetic that when a patient asks me how much a treatment will cost him/her, I do not have an answer.
Speaking of pricing, don’t even get me started on pharmaceutical company price gouging. Yes, the H.P. Acthar gel may be the most egregious offender among rheumatology medications, but it’s easy to not prescribe a drug that costs $80,000 a vial and which does not do much more than prednisone does. On the other hand, I remember a time when colchicine cost $0.10 cents a pill and patients did not have to jump through hoops to get it.
And what of reproductive freedom? Our patients rely on us for advice about their childbearing options, including birth control, in vitro fertilization, and pregnancy termination.
Finally, and most important, the things that affect me most are the issues that affect patients. The lowest-hanging fruit here is the abject incompetence of the federal response to the ongoing pandemic. How many of our patients’ lives have been lost or adversely affected? And what of coverage for preexisting conditions for the vast majority of our patients, whose illnesses are chronic?
While we’re at it, the fact of health insurance being tied to employment, something that seemingly no other country in the developed world does, makes living with chronic conditions outright scary, doesn’t it? It isn’t quite so easy to remain employed when one cannot get the right medications for RA.
I could go on. Gun violence and health care disparities, vaccine denialism, coverage for mental health issues, LGBTQ rights, refugee rights, police brutality … there is a seemingly endless list of things to care about. It’s exhausting.
While I do use my Twitter account to learn from colleagues and to promote work that interests me, my primary aim is to participate in civil society as a person. Critics will use “stay in your lane” as shorthand to say x professionals should stick to x (actors to acting, musicians to music, athletes to sports). If only I could. But my humanity won’t let me. Aristotle said man is a political animal; even the venerable New England Journal of Medicine has found it impossible to keep silent.
Karmela Kim Chan, MD, is an assistant professor at Weill Cornell Medicine, New York, and an attending physician at the Hospital for Special Surgery and Memorial Sloan Kettering Cancer Center, both in New York. Before moving to New York City, she spent 7 years in private practice in Rhode Island and was a past columnist for MDedge Rheumatology, writing about the challenges of starting life as a full-fledged rheumatologist in a private practice.
A version of this article originally appeared on Medscape.com.
COVID-19 vaccine distribution could start in 2 weeks, Pence says
Initial doses of a coronavirus vaccine could be sent out as early as mid-December, Vice President Mike Pence told governors during a call on Monday.
The distribution process could start during the week of Dec. 14, according to audio of a White House Coronavirus Task Force call obtained by CBS News. The call focused on the timeline of vaccine approval and distribution.
“With this morning’s news that Moderna is joining Pfizer in submitting an emergency-use authorization [to the Food and Drug Administration], we continue to be on pace,” Pence said.
The FDA is scheduled to make a decision about Pfizer’s emergency use authorization after an advisory panel meets on Dec. 10 to review the company’s application. FDA Commissioner Stephen Hahn, MD, didn’t commit to the Dec. 14 date, CBS News reported.
“We do all the number crunching ourselves,” Dr. Hahn said. “We look line by line by line on all the data, on all the patients and manufacturing. We do statistical analyses and we come to our own conclusions to support a decision of either thumbs-up or thumbs-down.”
According to a meeting agenda, Pfizer vaccine deliveries should start on Dec. 15, followed by the Moderna vaccine on Dec. 22, CBS News reported.
Between Dec. 13-19, Pfizer is slated to deliver 6.4 million doses, which is enough to immunize about 3 million people with two shots. An “undetermined number” are reserved for backup doses, the news outlet reported.
During the next week, Pfizer and Moderna are scheduled to produce enough doses to vaccinate an additional 10 million people. By the end of the month, about 30 million people should receive doses.
As vaccines begin to roll out, Mr. Pence said “we have a ways to go” in reassuring the public about immunization. He urged governors to use their “bully pulpit” to educate their states and “develop public confidence” in the vaccines.
During the call, Anthony Fauci, MD, director of the National Institute for Allergy and Infectious Diseases, supported the safety and efficacy of the vaccines. Although the vaccine development and approval process was accelerated this year, he said, it “does not at all compromise safety, nor does it compromise scientific integrity.”
“Any misrepresentation that the vaccines had government interference or company interference is patently untrue,” he said.
This article first appeared on Medscape.com.
Initial doses of a coronavirus vaccine could be sent out as early as mid-December, Vice President Mike Pence told governors during a call on Monday.
The distribution process could start during the week of Dec. 14, according to audio of a White House Coronavirus Task Force call obtained by CBS News. The call focused on the timeline of vaccine approval and distribution.
“With this morning’s news that Moderna is joining Pfizer in submitting an emergency-use authorization [to the Food and Drug Administration], we continue to be on pace,” Pence said.
The FDA is scheduled to make a decision about Pfizer’s emergency use authorization after an advisory panel meets on Dec. 10 to review the company’s application. FDA Commissioner Stephen Hahn, MD, didn’t commit to the Dec. 14 date, CBS News reported.
“We do all the number crunching ourselves,” Dr. Hahn said. “We look line by line by line on all the data, on all the patients and manufacturing. We do statistical analyses and we come to our own conclusions to support a decision of either thumbs-up or thumbs-down.”
According to a meeting agenda, Pfizer vaccine deliveries should start on Dec. 15, followed by the Moderna vaccine on Dec. 22, CBS News reported.
Between Dec. 13-19, Pfizer is slated to deliver 6.4 million doses, which is enough to immunize about 3 million people with two shots. An “undetermined number” are reserved for backup doses, the news outlet reported.
During the next week, Pfizer and Moderna are scheduled to produce enough doses to vaccinate an additional 10 million people. By the end of the month, about 30 million people should receive doses.
As vaccines begin to roll out, Mr. Pence said “we have a ways to go” in reassuring the public about immunization. He urged governors to use their “bully pulpit” to educate their states and “develop public confidence” in the vaccines.
During the call, Anthony Fauci, MD, director of the National Institute for Allergy and Infectious Diseases, supported the safety and efficacy of the vaccines. Although the vaccine development and approval process was accelerated this year, he said, it “does not at all compromise safety, nor does it compromise scientific integrity.”
“Any misrepresentation that the vaccines had government interference or company interference is patently untrue,” he said.
This article first appeared on Medscape.com.
Initial doses of a coronavirus vaccine could be sent out as early as mid-December, Vice President Mike Pence told governors during a call on Monday.
The distribution process could start during the week of Dec. 14, according to audio of a White House Coronavirus Task Force call obtained by CBS News. The call focused on the timeline of vaccine approval and distribution.
“With this morning’s news that Moderna is joining Pfizer in submitting an emergency-use authorization [to the Food and Drug Administration], we continue to be on pace,” Pence said.
The FDA is scheduled to make a decision about Pfizer’s emergency use authorization after an advisory panel meets on Dec. 10 to review the company’s application. FDA Commissioner Stephen Hahn, MD, didn’t commit to the Dec. 14 date, CBS News reported.
“We do all the number crunching ourselves,” Dr. Hahn said. “We look line by line by line on all the data, on all the patients and manufacturing. We do statistical analyses and we come to our own conclusions to support a decision of either thumbs-up or thumbs-down.”
According to a meeting agenda, Pfizer vaccine deliveries should start on Dec. 15, followed by the Moderna vaccine on Dec. 22, CBS News reported.
Between Dec. 13-19, Pfizer is slated to deliver 6.4 million doses, which is enough to immunize about 3 million people with two shots. An “undetermined number” are reserved for backup doses, the news outlet reported.
During the next week, Pfizer and Moderna are scheduled to produce enough doses to vaccinate an additional 10 million people. By the end of the month, about 30 million people should receive doses.
As vaccines begin to roll out, Mr. Pence said “we have a ways to go” in reassuring the public about immunization. He urged governors to use their “bully pulpit” to educate their states and “develop public confidence” in the vaccines.
During the call, Anthony Fauci, MD, director of the National Institute for Allergy and Infectious Diseases, supported the safety and efficacy of the vaccines. Although the vaccine development and approval process was accelerated this year, he said, it “does not at all compromise safety, nor does it compromise scientific integrity.”
“Any misrepresentation that the vaccines had government interference or company interference is patently untrue,” he said.
This article first appeared on Medscape.com.
Medicare finalizes 2021 physician pay rule with E/M changes
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule will take effect within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%).
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a Tuesday statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’ planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on January 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement on Tuesday, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a Tuesday tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a November 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
A version of this article originally appeared on Medscape.com.
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule will take effect within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%).
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a Tuesday statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’ planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on January 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement on Tuesday, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a Tuesday tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a November 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
A version of this article originally appeared on Medscape.com.
Medicare officials stuck with their plan to increase payments for office visits for primary care and several other specialties that focus on helping patients manage complex conditions such as diabetes. In doing so, Medicare also finalized cuts for other fields, triggering a new wave of protests.
The final version of the 2021 Medicare physician fee schedule was unveiled on the night of Dec. 1. The Centers for Medicare & Medicaid Services posted an unofficial copy of the rule, which will later be published in the Federal Register.
CMS said it completed work on this massive annual review of payments for clinicians later than it usually does because of the demands of the federal response to the COVID-19 pandemic. The 2021 physician fee rule will take effect within a 30-day period instead of the usual 60-day time frame.
The most contentious item proposed for 2021 was a reshuffling of payments among specialties as part of an overhaul of Medicare’s approach to valuing evaluation and management (E/M) services. There was broader support for other aspects of the E/M overhaul, which are intended to cut some of the administrative hassle clinicians face.
“This finalized policy marks the most significant updates to E/M codes in 30 years, reducing burden on doctors imposed by the coding system and rewarding time spent evaluating and managing their patients’ care,” CMS Administrator Seema Verma said in a statement. “In the past, the system has rewarded interventions and procedures over time spent with patients – time taken preventing disease and managing chronic illnesses.”
In the final rule, CMS summarized these results of the E/M changes in Table 106. CMS largely stuck with the approach outlined in a draft rule released in August, with minor changes in the amounts of cuts and increases.
Specialties in line for increases under the 2021 final physician fee schedule include allergy/immunology (9%), endocrinology (16%), family practice (13%), general practice (7%), geriatrics (3%), hematology/oncology (14%), internal medicine (4%), nephrology (6%), physician assistants (8%), psychiatry (7%), rheumatology (15%), and urology (8%).
In line for cuts would be anesthesiology (–8%), cardiac surgery (–8%), emergency medicine (–6%), general surgery (–6%), infectious disease (–4%), neurosurgery (–6%), physical/occupational therapy (–9%), plastic surgery (–7%), radiology (–10%), and thoracic surgery (–8%).
CMS had initially set these changes in 2021 pay in motion in the 2020 physician fee schedule. The agency subsequently faced significant opposition to its plans. Many physician groups sought to waive a “budget-neutral” approach to the E/M overhaul, which makes the offsetting of cuts necessary. They argued this would allow increased compensation for clinicians whose practices focus on office visits without requiring offsetting cuts from other fields of medicine.
The American Medical Association is among those urging Congress to prevent or postpone the payment reductions resulting from Medicare’s budget neutrality requirement as applied to the E/M overhaul.
In a Tuesday statement, AMA President Susan R. Bailey, MD, noted that many physicians are facing “substantial economic hardships due to COVID-19.”
By AMA’s calculations, CMS’ planned 2021 E/M overhaul could result in “a shocking reduction of 10.2% to Medicare payment rates,” according to Bailey’s statement. The AMA strongly supports other aspects of the E/M changes CMS finalized, which Bailey said will result in “simpler and more flexible” coding and documentation.
The Surgical Care Coalition, which represents about a dozen medical specialty associations, is asking members of Congress to block the full implementation of the E/M overhaul.
In a Dec. 1 statement, the coalition urged the passage of a bill (HR 8702) that has been introduced in the House by a bipartisan duo of physicians, Rep. Ami Bera, MD (D-Calif.), and Rep. Larry Bucshon, MD (R-Ind.). Their bill would effectively block the cuts from going into effect on January 1, 2021. It would provide an additional Medicare payment for certain services in 2021 and 2022 if the otherwise applicable payment is less than it would have been in 2020.
The Medicare E/M overhaul “was a dangerous policy even before the pandemic, and enacting it during the worst health care crisis in a century is unconscionable. If Congress fails to act, it will further strain a health care system that’s already been pushed to the brink due to the COVID-19 pandemic and undermine patient care,” said John A. Wilson, MD, president of the American Association of Neurological Surgeons, in a statement.
Also backing the Bera-Bucshon bill is the American College of Emergency Physicians. In a statement on Tuesday, ACEP President Mark Rosenberg, DO, MBA, urged Congress to act on this measure.
“Emergency physicians and other health care providers battling on the front lines of the ongoing pandemic are already under unprecedented financial strain as they continue to bear the brunt of COVID-19,” Dr. Rosenberg said. “These cuts would have a devastating impact for the future of emergency medicine and could seriously impede patients’ access to emergency care when they need it most.”
“Long overdue”
But there also are champions for the approach CMS took in the E/M overhaul. The influential Medicare Payment Advisory Commission (MedPAC) has argued strongly for keeping the budget-neutral approach to the E/M overhaul.
In an Oct. 2 comment to CMS about the draft 2021 physician fee schedule, MedPAC Chairman Michael E. Chernew, PhD, said this approach would “help rebalance the fee schedule from services that have become overvalued to services that have become undervalued.”
This budget-neutral approach also “will go further in reducing the large gap in compensation between primary care physicians (who had a median income of $243,000 in 2018) and specialists such as surgeons (whose median income was $426,000 in 2018),” Dr. Chernew wrote.
In a Tuesday tweet, Robert B. Doherty, senior vice president of governmental affairs and public policy for the American College of Physicians, said CMS had “finalized long overdue payment increases for primary and comprehensive care including an add-in for more complex visits.”
The American Academy of Family Physicians joined ACP in a November 30 letter to congressional leaders, urging them to allow Medicare “to increase investment in primary care, benefiting millions of Medicare patients and the program itself, and reject last minute efforts to prevent these essential and long-overdue changes from going fully into effect on January 1, 2021.”
In the letter, AAFP and ACP and their cosigners argued for a need to address “underinvestment” in primary care by finalizing the E/M overhaul.
“Given that six in ten American adults have a chronic disease and four in ten have two or more chronic conditions, why would we, as a country, accept such an inadequate investment in the very care model that stands to provide maximum value to these patients?” they wrote. “Since we know that individuals with a longitudinal relationship with a primary care physician have better health outcomes and use fewer health care resources, why would we continue to direct money to higher-cost, marginal value services?”
A version of this article originally appeared on Medscape.com.
Colchicine a case study for what’s wrong with U.S. drug pricing
Public spending on colchicine has grown exponentially over the past decade despite generics suggesting an uphill slog for patients seeking access to long-term therapy for gout or cardiac conditions.
Medicaid spending on single-ingredient colchicine jumped 2,833%, from $1.1 million in 2008 to $32.2 million in 2017, new findings show. Medicaid expansion likely played a role in the increase, but 58% was due to price hikes alone.
The centuries-old drug sold for pennies in the United States before increasing 50-fold to about $5 per pill in 2009 after the first FDA-approved colchicine product, Colcrys, was granted 3 years’ market exclusivity for the treatment of acute gout based on a 1-week trial.
If prices had remained at pre-Colcrys levels, Medicaid spending in 2017 would have totaled just $2.1 million rather than $32.2 million according to the analysis, published online Nov. 30 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2020.5017).
The study was motivated by difficulties gout patients have in accessing colchicine, but also last year’s COLCOT trial, which reported fewer ischemic cardiovascular events in patients receiving colchicine after MI, observed Natalie McCormick, PhD, of Massachusetts General Hospital and Harvard Medical School, both in Boston.
“They were suggesting it could be a cost-effective way for secondary prevention and it is fairly inexpensive in most countries, but not the U.S.,” she said in an interview. “So there’s really a potential to increase public spending if more and more patients are then taking colchicine for prevention of cardiovascular events and the prices don’t change.”
The current pandemic could potentially further increase demand. Results initially slated for September are expected this month from the COLCORONA trial, which is testing whether the anti-inflammatory agent can prevent hospitalizations, lung complications, and death when given early in the course of COVID-19.
University of Oxford (England) researchers also announced last week that colchicine is being added to the massive RECOVERY trial, which is studying treatments for hospitalized COVID-19 patients.
Notably, the Canadian-based COLCOT trial did not use Colcrys, but rather a colchicine product that costs just $0.26 a pill in Canada, roughly the price of most generics available worldwide.
Authorized generics typically drive down drug prices when competing with independent generics, but this competition is missing in the United States, where Colcrys holds patents until 2029, Dr. McCormick and colleagues noted. More than a half-dozen independent generics have FDA approval to date, but only authorized generics with price points set by the brand-name companies are available to treat acute gout, pericarditis, and potentially millions with MI.
“One of the key takeaways is this difference between the brand names and the authorized generics and the independents,” she said. “The authorized [generics] have really not saved money. The list prices were just slightly lower and patients can also have more difficulty in getting those covered.”
For this analysis, the investigators used Medicaid and Medicare data to examine prices for all available forms of colchicine from 2008 to 2017, including unregulated/unapproved colchicine (2008-2010), generic combination probenecid-colchicine (2008-2017), Colcrys (2009-2017), brand-name single-ingredient colchicine Mitigare (approved in late 2014 but not marketed until 2015), and their authorized generics (2015-2017). Medicare trends from 2012 to 2017 were analyzed separately because pre-Colcrys Medicare data were not available.
Based on the results, combined spending on Medicare and Medicaid claims for single-ingredient colchicine exceeded $340 million in 2017.
Inflation- and rebate-adjusted Medicaid unit prices rose from $0.24 a pill in 2008, when unapproved formulations were still available, to $4.20 a pill in 2011 (Colcrys only), and peaked at $4.66 a pill in 2015 (Colcrys plus authorized generics).
Prescribing of lower-priced probenecid-colchicine ($0.66/pill in 2017) remained stable throughout. Medicaid rebate-adjusted prices in 2017 were $3.99/pill for all single-ingredient colchicine products, $5.13/pill for Colcrys, $4.49/pill for Mitigare, and $3.88/pill for authorized generics.
Medicare rebate-adjusted 2017 per-pill prices were $5.81 for all single-ingredient colchicine products, $6.78 for Colcrys, $5.68 for Mitigare, $5.16 for authorized generics, and $0.70 for probenecid-colchicine.
“Authorized generics have still driven high spending,” Dr. McCormick said. “We really need to encourage more competition in order to improve access.”
In an accompanying commentary, B. Joseph Guglielmo, PharmD, University of California, San Francisco, pointed out that the estimated median research and development cost to bring a drug to market is between $985 million and $1,335 million, which inevitably translates into a high selling price for the drug. Such investment and its resultant cost, however, should be associated with potential worth to society.
“Only a fraction of an investment was required for Colcrys, a product that has provided no increased value and an unnecessary, long-term cost burden to the health care system,” he wrote. “The current study findings illustrate that we can never allow such an egregious case to take place again.”
Dr. McCormick reported grants from Canadian Institutes of Health Research during the conduct of the study. Dr. Guglielmo reported having no relevant conflicts of interest.
This article first appeared on Medscape.com.
Public spending on colchicine has grown exponentially over the past decade despite generics suggesting an uphill slog for patients seeking access to long-term therapy for gout or cardiac conditions.
Medicaid spending on single-ingredient colchicine jumped 2,833%, from $1.1 million in 2008 to $32.2 million in 2017, new findings show. Medicaid expansion likely played a role in the increase, but 58% was due to price hikes alone.
The centuries-old drug sold for pennies in the United States before increasing 50-fold to about $5 per pill in 2009 after the first FDA-approved colchicine product, Colcrys, was granted 3 years’ market exclusivity for the treatment of acute gout based on a 1-week trial.
If prices had remained at pre-Colcrys levels, Medicaid spending in 2017 would have totaled just $2.1 million rather than $32.2 million according to the analysis, published online Nov. 30 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2020.5017).
The study was motivated by difficulties gout patients have in accessing colchicine, but also last year’s COLCOT trial, which reported fewer ischemic cardiovascular events in patients receiving colchicine after MI, observed Natalie McCormick, PhD, of Massachusetts General Hospital and Harvard Medical School, both in Boston.
“They were suggesting it could be a cost-effective way for secondary prevention and it is fairly inexpensive in most countries, but not the U.S.,” she said in an interview. “So there’s really a potential to increase public spending if more and more patients are then taking colchicine for prevention of cardiovascular events and the prices don’t change.”
The current pandemic could potentially further increase demand. Results initially slated for September are expected this month from the COLCORONA trial, which is testing whether the anti-inflammatory agent can prevent hospitalizations, lung complications, and death when given early in the course of COVID-19.
University of Oxford (England) researchers also announced last week that colchicine is being added to the massive RECOVERY trial, which is studying treatments for hospitalized COVID-19 patients.
Notably, the Canadian-based COLCOT trial did not use Colcrys, but rather a colchicine product that costs just $0.26 a pill in Canada, roughly the price of most generics available worldwide.
Authorized generics typically drive down drug prices when competing with independent generics, but this competition is missing in the United States, where Colcrys holds patents until 2029, Dr. McCormick and colleagues noted. More than a half-dozen independent generics have FDA approval to date, but only authorized generics with price points set by the brand-name companies are available to treat acute gout, pericarditis, and potentially millions with MI.
“One of the key takeaways is this difference between the brand names and the authorized generics and the independents,” she said. “The authorized [generics] have really not saved money. The list prices were just slightly lower and patients can also have more difficulty in getting those covered.”
For this analysis, the investigators used Medicaid and Medicare data to examine prices for all available forms of colchicine from 2008 to 2017, including unregulated/unapproved colchicine (2008-2010), generic combination probenecid-colchicine (2008-2017), Colcrys (2009-2017), brand-name single-ingredient colchicine Mitigare (approved in late 2014 but not marketed until 2015), and their authorized generics (2015-2017). Medicare trends from 2012 to 2017 were analyzed separately because pre-Colcrys Medicare data were not available.
Based on the results, combined spending on Medicare and Medicaid claims for single-ingredient colchicine exceeded $340 million in 2017.
Inflation- and rebate-adjusted Medicaid unit prices rose from $0.24 a pill in 2008, when unapproved formulations were still available, to $4.20 a pill in 2011 (Colcrys only), and peaked at $4.66 a pill in 2015 (Colcrys plus authorized generics).
Prescribing of lower-priced probenecid-colchicine ($0.66/pill in 2017) remained stable throughout. Medicaid rebate-adjusted prices in 2017 were $3.99/pill for all single-ingredient colchicine products, $5.13/pill for Colcrys, $4.49/pill for Mitigare, and $3.88/pill for authorized generics.
Medicare rebate-adjusted 2017 per-pill prices were $5.81 for all single-ingredient colchicine products, $6.78 for Colcrys, $5.68 for Mitigare, $5.16 for authorized generics, and $0.70 for probenecid-colchicine.
“Authorized generics have still driven high spending,” Dr. McCormick said. “We really need to encourage more competition in order to improve access.”
In an accompanying commentary, B. Joseph Guglielmo, PharmD, University of California, San Francisco, pointed out that the estimated median research and development cost to bring a drug to market is between $985 million and $1,335 million, which inevitably translates into a high selling price for the drug. Such investment and its resultant cost, however, should be associated with potential worth to society.
“Only a fraction of an investment was required for Colcrys, a product that has provided no increased value and an unnecessary, long-term cost burden to the health care system,” he wrote. “The current study findings illustrate that we can never allow such an egregious case to take place again.”
Dr. McCormick reported grants from Canadian Institutes of Health Research during the conduct of the study. Dr. Guglielmo reported having no relevant conflicts of interest.
This article first appeared on Medscape.com.
Public spending on colchicine has grown exponentially over the past decade despite generics suggesting an uphill slog for patients seeking access to long-term therapy for gout or cardiac conditions.
Medicaid spending on single-ingredient colchicine jumped 2,833%, from $1.1 million in 2008 to $32.2 million in 2017, new findings show. Medicaid expansion likely played a role in the increase, but 58% was due to price hikes alone.
The centuries-old drug sold for pennies in the United States before increasing 50-fold to about $5 per pill in 2009 after the first FDA-approved colchicine product, Colcrys, was granted 3 years’ market exclusivity for the treatment of acute gout based on a 1-week trial.
If prices had remained at pre-Colcrys levels, Medicaid spending in 2017 would have totaled just $2.1 million rather than $32.2 million according to the analysis, published online Nov. 30 in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2020.5017).
The study was motivated by difficulties gout patients have in accessing colchicine, but also last year’s COLCOT trial, which reported fewer ischemic cardiovascular events in patients receiving colchicine after MI, observed Natalie McCormick, PhD, of Massachusetts General Hospital and Harvard Medical School, both in Boston.
“They were suggesting it could be a cost-effective way for secondary prevention and it is fairly inexpensive in most countries, but not the U.S.,” she said in an interview. “So there’s really a potential to increase public spending if more and more patients are then taking colchicine for prevention of cardiovascular events and the prices don’t change.”
The current pandemic could potentially further increase demand. Results initially slated for September are expected this month from the COLCORONA trial, which is testing whether the anti-inflammatory agent can prevent hospitalizations, lung complications, and death when given early in the course of COVID-19.
University of Oxford (England) researchers also announced last week that colchicine is being added to the massive RECOVERY trial, which is studying treatments for hospitalized COVID-19 patients.
Notably, the Canadian-based COLCOT trial did not use Colcrys, but rather a colchicine product that costs just $0.26 a pill in Canada, roughly the price of most generics available worldwide.
Authorized generics typically drive down drug prices when competing with independent generics, but this competition is missing in the United States, where Colcrys holds patents until 2029, Dr. McCormick and colleagues noted. More than a half-dozen independent generics have FDA approval to date, but only authorized generics with price points set by the brand-name companies are available to treat acute gout, pericarditis, and potentially millions with MI.
“One of the key takeaways is this difference between the brand names and the authorized generics and the independents,” she said. “The authorized [generics] have really not saved money. The list prices were just slightly lower and patients can also have more difficulty in getting those covered.”
For this analysis, the investigators used Medicaid and Medicare data to examine prices for all available forms of colchicine from 2008 to 2017, including unregulated/unapproved colchicine (2008-2010), generic combination probenecid-colchicine (2008-2017), Colcrys (2009-2017), brand-name single-ingredient colchicine Mitigare (approved in late 2014 but not marketed until 2015), and their authorized generics (2015-2017). Medicare trends from 2012 to 2017 were analyzed separately because pre-Colcrys Medicare data were not available.
Based on the results, combined spending on Medicare and Medicaid claims for single-ingredient colchicine exceeded $340 million in 2017.
Inflation- and rebate-adjusted Medicaid unit prices rose from $0.24 a pill in 2008, when unapproved formulations were still available, to $4.20 a pill in 2011 (Colcrys only), and peaked at $4.66 a pill in 2015 (Colcrys plus authorized generics).
Prescribing of lower-priced probenecid-colchicine ($0.66/pill in 2017) remained stable throughout. Medicaid rebate-adjusted prices in 2017 were $3.99/pill for all single-ingredient colchicine products, $5.13/pill for Colcrys, $4.49/pill for Mitigare, and $3.88/pill for authorized generics.
Medicare rebate-adjusted 2017 per-pill prices were $5.81 for all single-ingredient colchicine products, $6.78 for Colcrys, $5.68 for Mitigare, $5.16 for authorized generics, and $0.70 for probenecid-colchicine.
“Authorized generics have still driven high spending,” Dr. McCormick said. “We really need to encourage more competition in order to improve access.”
In an accompanying commentary, B. Joseph Guglielmo, PharmD, University of California, San Francisco, pointed out that the estimated median research and development cost to bring a drug to market is between $985 million and $1,335 million, which inevitably translates into a high selling price for the drug. Such investment and its resultant cost, however, should be associated with potential worth to society.
“Only a fraction of an investment was required for Colcrys, a product that has provided no increased value and an unnecessary, long-term cost burden to the health care system,” he wrote. “The current study findings illustrate that we can never allow such an egregious case to take place again.”
Dr. McCormick reported grants from Canadian Institutes of Health Research during the conduct of the study. Dr. Guglielmo reported having no relevant conflicts of interest.
This article first appeared on Medscape.com.
Intensive glucose control after acute ischemic stroke does not improve functional outcomes
Background: Higher glucose immediately following acute ischemic stroke is known to be associated with poor outcomes. Patients with elevated glucoses in the aftermath of an acute ischemic stroke are more likely to have expansion of ischemic area and are more likely to have hemorrhagic conversion.

Study design: Randomized, controlled trial, with blinded outcome assessment.
Setting: 63 sites in the United States.
Synopsis: A total of 1,151 patients were randomized to either intensive (goal blood glucose, 80-130 mg/dL) or standard (goal blood glucose, 80-179 mg/dL) glucose control for up to the first 72 hours after presenting with acute ischemic stroke. Patients in the intensive control group were given continuous IV insulin and patients in the standard control group were given subcutaneous sliding. There was no difference between groups (intensive vs. standard) with regards to the primary outcome, which was the percentage of patients who achieved a modified Rankin Score at 90 days of 0-2 (20.5% vs 21.6%; adjusted relative risk, 0.97; 95% confidence interval, 0.87-1.08; P = .55). Severe hypoglycemia (blood glucose of less than 40 mg/dL) occurred in the intensive control group only. The American Heart Association/American Stroke Association guidelines support target blood glucose of 140-180 mg/dL, though limited evidence to support this guideline is noted.
Bottom line: Patients who underwent intensive glucose control regimens following acute ischemic stroke did not have significantly different functional outcomes at 90 days than those who had standard glucose control therapy.
Citation: Johnston KC et al. Intensive vs. standard treatment of hyperglycemia and functional outcome in patients with acute ischemic stroke: The SHINE randomized clinical trial. JAMA. 2019 Jul 23/30;322(4):326-35.
Dr. Fritz is assistant professor of medicine and the director of hospitalist operations at St. Louis University School of Medicine.
Background: Higher glucose immediately following acute ischemic stroke is known to be associated with poor outcomes. Patients with elevated glucoses in the aftermath of an acute ischemic stroke are more likely to have expansion of ischemic area and are more likely to have hemorrhagic conversion.
Study design: Randomized, controlled trial, with blinded outcome assessment.
Setting: 63 sites in the United States.
Synopsis: A total of 1,151 patients were randomized to either intensive (goal blood glucose, 80-130 mg/dL) or standard (goal blood glucose, 80-179 mg/dL) glucose control for up to the first 72 hours after presenting with acute ischemic stroke. Patients in the intensive control group were given continuous IV insulin and patients in the standard control group were given subcutaneous sliding. There was no difference between groups (intensive vs. standard) with regards to the primary outcome, which was the percentage of patients who achieved a modified Rankin Score at 90 days of 0-2 (20.5% vs 21.6%; adjusted relative risk, 0.97; 95% confidence interval, 0.87-1.08; P = .55). Severe hypoglycemia (blood glucose of less than 40 mg/dL) occurred in the intensive control group only. The American Heart Association/American Stroke Association guidelines support target blood glucose of 140-180 mg/dL, though limited evidence to support this guideline is noted.
Bottom line: Patients who underwent intensive glucose control regimens following acute ischemic stroke did not have significantly different functional outcomes at 90 days than those who had standard glucose control therapy.
Citation: Johnston KC et al. Intensive vs. standard treatment of hyperglycemia and functional outcome in patients with acute ischemic stroke: The SHINE randomized clinical trial. JAMA. 2019 Jul 23/30;322(4):326-35.
Dr. Fritz is assistant professor of medicine and the director of hospitalist operations at St. Louis University School of Medicine.
Background: Higher glucose immediately following acute ischemic stroke is known to be associated with poor outcomes. Patients with elevated glucoses in the aftermath of an acute ischemic stroke are more likely to have expansion of ischemic area and are more likely to have hemorrhagic conversion.
Study design: Randomized, controlled trial, with blinded outcome assessment.
Setting: 63 sites in the United States.
Synopsis: A total of 1,151 patients were randomized to either intensive (goal blood glucose, 80-130 mg/dL) or standard (goal blood glucose, 80-179 mg/dL) glucose control for up to the first 72 hours after presenting with acute ischemic stroke. Patients in the intensive control group were given continuous IV insulin and patients in the standard control group were given subcutaneous sliding. There was no difference between groups (intensive vs. standard) with regards to the primary outcome, which was the percentage of patients who achieved a modified Rankin Score at 90 days of 0-2 (20.5% vs 21.6%; adjusted relative risk, 0.97; 95% confidence interval, 0.87-1.08; P = .55). Severe hypoglycemia (blood glucose of less than 40 mg/dL) occurred in the intensive control group only. The American Heart Association/American Stroke Association guidelines support target blood glucose of 140-180 mg/dL, though limited evidence to support this guideline is noted.
Bottom line: Patients who underwent intensive glucose control regimens following acute ischemic stroke did not have significantly different functional outcomes at 90 days than those who had standard glucose control therapy.
Citation: Johnston KC et al. Intensive vs. standard treatment of hyperglycemia and functional outcome in patients with acute ischemic stroke: The SHINE randomized clinical trial. JAMA. 2019 Jul 23/30;322(4):326-35.
Dr. Fritz is assistant professor of medicine and the director of hospitalist operations at St. Louis University School of Medicine.
Should CTCs guide treatment choice in HR+, HER2– breast cancer?
investigators wrote in JAMA Oncology.
However, authors of a related editorial suggested CTC counts are not adequate for guiding treatment choice in this population.
In a phase 3 trial, investigators compared the use of CTC counts and the use of clinical factors to guide the decision between chemotherapy and endocrine therapy. Results showed similar progression-free survival (PFS) and overall survival (OS) with both methods but more chemotherapy use with the CTC method.
“The results of this trial demonstrate the reliability and clinical utility of CTC count to guide the choice between single-agent endocrine therapy and chemotherapy as first-line treatment,” but “at the cost of a higher proportion of patients treated with chemotherapy,” study author François-Clement Bidard, MD, PhD, of Institut Curie in Saint-Cloud, France, and colleagues wrote.
The investigators explained that endocrine therapy is the preferred first-line treatment option in this patient population, but chemotherapy is used when women are in visceral crisis, with rapidly progressive, symptomatic disease. The decision usually rests on clinical factors, such as tumor subtype and performance status, but there’s interphysician variability.
The team hoped to find a “more reliable, standardized, and reproducible” biomarker to help remove some of the uncertainty from the situation. They tested CTC count, a well-established prognostic indicator of PFS and OS, as a candidate.
Study results
The trial included 755 patients with hormone receptor–positive, HER2-negative breast cancer in the per-protocol population. The patients’ median age was 63 years (range, 30-88 years).
Among the 377 patients randomized to the CTC arm, those with counts at or above 5 CTCs per 7.5 mL received chemotherapy, while those with a lower count received endocrine therapy.
The 378 patients in the standard-care group received endocrine therapy or chemotherapy based on provider choice guided by clinical factors.
Chemotherapy was given to 37% of patients in the CTC arm and 27% of those in the standard arm.
The median PFS was 15.5 months in the CTC arm and 13.9 months in the standard arm, which meant the primary endpoint of noninferiority was met (hazard ratio, 0.94; 90% confidence interval, 0.81-1.09).
Age older than 60 years was the only baseline characteristic associated with better PFS with CTC-driven decision-making. This may be because of the greater “use of endocrine therapy as the clinically favored treatment, whatever the other clinicopathologic characteristics,” in older subjects, the investigators wrote.
As with PFS, the median OS was similar between the study arms – 47.3 months in the CTC arm and 42.8 months in the standard arm (HR, 0.91; 95% CI, 0.71-1.16).
‘Not good enough’
The investigators behind this study had “a worthy goal,” according to authors of a related editorial.
Without “predictive biomarkers, we are left with our clinical knowledge, experience, and intuition. Patients are left with uncertainty, doubt, and fear,” Tarah Ballinger, MD,, of Indiana University, Indianapolis, and colleagues wrote in the editorial.
However, the editorialists had concerns about the findings. For one thing, the investigators hypothesized that relying on CTC would lead to a deescalation from chemotherapy to endocrine therapy, but use of chemotherapy was actually 10% higher in the CTC arm.
“Adding to or replacing the parameters we use to make a clinical decision should help us improve the lives of patients. ... We should demand an improvement in outcomes before accepting a strategy that exposes more patients to more toxic therapy. Not worse simply is not good enough,” the editorialists wrote.
In addition, the trial was completed before CDK4/6 inhibitors became a standard add-on with endocrine therapy for hormone receptor–positive, HER2-negative patients.
“The overall response rate to CDK4/6 inhibitor therapy is higher than with traditional chemotherapy, and several randomized trials have failed to show a survival benefit of upfront chemotherapy compared with CDK4/6 inhibitor use. ... Thus, it is even less likely that we can assume that baseline high CTC count corresponds to a need for chemotherapy in a modern treatment landscape that offers more patients more benefit from hormone therapy,” Dr. Ballinger and colleagues wrote.
The editorialists concluded that CTC count “alone at baseline primarily reflects disease bulk, much like anatomic staging, rather than disease biology. As treatments become more rooted in our knowledge of breast cancer biology, decisions based on disease bulk are decidedly out of place.”
Perhaps a better use, they suggested, is for treatment personalization. For instance, patients with persistently elevated CTCs despite standard approaches could consider trials of novel targeted therapies, or CTCs could be sequenced to identify actionable molecular targets, achieving a “clinical utility that merely counting CTCs lacks,” the editorialists wrote.
This study was funded by the Institut Curie, the French National Cancer Institute, and Menarini Silicon Biosystems, the maker of the CTC assay used in the trial. The investigators disclosed relationships with Menarini and many other companies. Dr. Ballinger receives honoraria from Medscape, which is owned by the same company as this news organization.
SOURCE: Bidard FC et al. JAMA Oncol. 2020 Nov 5. doi: 10.1001/jamaoncol.2020.5660.
investigators wrote in JAMA Oncology.
However, authors of a related editorial suggested CTC counts are not adequate for guiding treatment choice in this population.
In a phase 3 trial, investigators compared the use of CTC counts and the use of clinical factors to guide the decision between chemotherapy and endocrine therapy. Results showed similar progression-free survival (PFS) and overall survival (OS) with both methods but more chemotherapy use with the CTC method.
“The results of this trial demonstrate the reliability and clinical utility of CTC count to guide the choice between single-agent endocrine therapy and chemotherapy as first-line treatment,” but “at the cost of a higher proportion of patients treated with chemotherapy,” study author François-Clement Bidard, MD, PhD, of Institut Curie in Saint-Cloud, France, and colleagues wrote.
The investigators explained that endocrine therapy is the preferred first-line treatment option in this patient population, but chemotherapy is used when women are in visceral crisis, with rapidly progressive, symptomatic disease. The decision usually rests on clinical factors, such as tumor subtype and performance status, but there’s interphysician variability.
The team hoped to find a “more reliable, standardized, and reproducible” biomarker to help remove some of the uncertainty from the situation. They tested CTC count, a well-established prognostic indicator of PFS and OS, as a candidate.
Study results
The trial included 755 patients with hormone receptor–positive, HER2-negative breast cancer in the per-protocol population. The patients’ median age was 63 years (range, 30-88 years).
Among the 377 patients randomized to the CTC arm, those with counts at or above 5 CTCs per 7.5 mL received chemotherapy, while those with a lower count received endocrine therapy.
The 378 patients in the standard-care group received endocrine therapy or chemotherapy based on provider choice guided by clinical factors.
Chemotherapy was given to 37% of patients in the CTC arm and 27% of those in the standard arm.
The median PFS was 15.5 months in the CTC arm and 13.9 months in the standard arm, which meant the primary endpoint of noninferiority was met (hazard ratio, 0.94; 90% confidence interval, 0.81-1.09).
Age older than 60 years was the only baseline characteristic associated with better PFS with CTC-driven decision-making. This may be because of the greater “use of endocrine therapy as the clinically favored treatment, whatever the other clinicopathologic characteristics,” in older subjects, the investigators wrote.
As with PFS, the median OS was similar between the study arms – 47.3 months in the CTC arm and 42.8 months in the standard arm (HR, 0.91; 95% CI, 0.71-1.16).
‘Not good enough’
The investigators behind this study had “a worthy goal,” according to authors of a related editorial.
Without “predictive biomarkers, we are left with our clinical knowledge, experience, and intuition. Patients are left with uncertainty, doubt, and fear,” Tarah Ballinger, MD,, of Indiana University, Indianapolis, and colleagues wrote in the editorial.
However, the editorialists had concerns about the findings. For one thing, the investigators hypothesized that relying on CTC would lead to a deescalation from chemotherapy to endocrine therapy, but use of chemotherapy was actually 10% higher in the CTC arm.
“Adding to or replacing the parameters we use to make a clinical decision should help us improve the lives of patients. ... We should demand an improvement in outcomes before accepting a strategy that exposes more patients to more toxic therapy. Not worse simply is not good enough,” the editorialists wrote.
In addition, the trial was completed before CDK4/6 inhibitors became a standard add-on with endocrine therapy for hormone receptor–positive, HER2-negative patients.
“The overall response rate to CDK4/6 inhibitor therapy is higher than with traditional chemotherapy, and several randomized trials have failed to show a survival benefit of upfront chemotherapy compared with CDK4/6 inhibitor use. ... Thus, it is even less likely that we can assume that baseline high CTC count corresponds to a need for chemotherapy in a modern treatment landscape that offers more patients more benefit from hormone therapy,” Dr. Ballinger and colleagues wrote.
The editorialists concluded that CTC count “alone at baseline primarily reflects disease bulk, much like anatomic staging, rather than disease biology. As treatments become more rooted in our knowledge of breast cancer biology, decisions based on disease bulk are decidedly out of place.”
Perhaps a better use, they suggested, is for treatment personalization. For instance, patients with persistently elevated CTCs despite standard approaches could consider trials of novel targeted therapies, or CTCs could be sequenced to identify actionable molecular targets, achieving a “clinical utility that merely counting CTCs lacks,” the editorialists wrote.
This study was funded by the Institut Curie, the French National Cancer Institute, and Menarini Silicon Biosystems, the maker of the CTC assay used in the trial. The investigators disclosed relationships with Menarini and many other companies. Dr. Ballinger receives honoraria from Medscape, which is owned by the same company as this news organization.
SOURCE: Bidard FC et al. JAMA Oncol. 2020 Nov 5. doi: 10.1001/jamaoncol.2020.5660.
investigators wrote in JAMA Oncology.
However, authors of a related editorial suggested CTC counts are not adequate for guiding treatment choice in this population.
In a phase 3 trial, investigators compared the use of CTC counts and the use of clinical factors to guide the decision between chemotherapy and endocrine therapy. Results showed similar progression-free survival (PFS) and overall survival (OS) with both methods but more chemotherapy use with the CTC method.
“The results of this trial demonstrate the reliability and clinical utility of CTC count to guide the choice between single-agent endocrine therapy and chemotherapy as first-line treatment,” but “at the cost of a higher proportion of patients treated with chemotherapy,” study author François-Clement Bidard, MD, PhD, of Institut Curie in Saint-Cloud, France, and colleagues wrote.
The investigators explained that endocrine therapy is the preferred first-line treatment option in this patient population, but chemotherapy is used when women are in visceral crisis, with rapidly progressive, symptomatic disease. The decision usually rests on clinical factors, such as tumor subtype and performance status, but there’s interphysician variability.
The team hoped to find a “more reliable, standardized, and reproducible” biomarker to help remove some of the uncertainty from the situation. They tested CTC count, a well-established prognostic indicator of PFS and OS, as a candidate.
Study results
The trial included 755 patients with hormone receptor–positive, HER2-negative breast cancer in the per-protocol population. The patients’ median age was 63 years (range, 30-88 years).
Among the 377 patients randomized to the CTC arm, those with counts at or above 5 CTCs per 7.5 mL received chemotherapy, while those with a lower count received endocrine therapy.
The 378 patients in the standard-care group received endocrine therapy or chemotherapy based on provider choice guided by clinical factors.
Chemotherapy was given to 37% of patients in the CTC arm and 27% of those in the standard arm.
The median PFS was 15.5 months in the CTC arm and 13.9 months in the standard arm, which meant the primary endpoint of noninferiority was met (hazard ratio, 0.94; 90% confidence interval, 0.81-1.09).
Age older than 60 years was the only baseline characteristic associated with better PFS with CTC-driven decision-making. This may be because of the greater “use of endocrine therapy as the clinically favored treatment, whatever the other clinicopathologic characteristics,” in older subjects, the investigators wrote.
As with PFS, the median OS was similar between the study arms – 47.3 months in the CTC arm and 42.8 months in the standard arm (HR, 0.91; 95% CI, 0.71-1.16).
‘Not good enough’
The investigators behind this study had “a worthy goal,” according to authors of a related editorial.
Without “predictive biomarkers, we are left with our clinical knowledge, experience, and intuition. Patients are left with uncertainty, doubt, and fear,” Tarah Ballinger, MD,, of Indiana University, Indianapolis, and colleagues wrote in the editorial.
However, the editorialists had concerns about the findings. For one thing, the investigators hypothesized that relying on CTC would lead to a deescalation from chemotherapy to endocrine therapy, but use of chemotherapy was actually 10% higher in the CTC arm.
“Adding to or replacing the parameters we use to make a clinical decision should help us improve the lives of patients. ... We should demand an improvement in outcomes before accepting a strategy that exposes more patients to more toxic therapy. Not worse simply is not good enough,” the editorialists wrote.
In addition, the trial was completed before CDK4/6 inhibitors became a standard add-on with endocrine therapy for hormone receptor–positive, HER2-negative patients.
“The overall response rate to CDK4/6 inhibitor therapy is higher than with traditional chemotherapy, and several randomized trials have failed to show a survival benefit of upfront chemotherapy compared with CDK4/6 inhibitor use. ... Thus, it is even less likely that we can assume that baseline high CTC count corresponds to a need for chemotherapy in a modern treatment landscape that offers more patients more benefit from hormone therapy,” Dr. Ballinger and colleagues wrote.
The editorialists concluded that CTC count “alone at baseline primarily reflects disease bulk, much like anatomic staging, rather than disease biology. As treatments become more rooted in our knowledge of breast cancer biology, decisions based on disease bulk are decidedly out of place.”
Perhaps a better use, they suggested, is for treatment personalization. For instance, patients with persistently elevated CTCs despite standard approaches could consider trials of novel targeted therapies, or CTCs could be sequenced to identify actionable molecular targets, achieving a “clinical utility that merely counting CTCs lacks,” the editorialists wrote.
This study was funded by the Institut Curie, the French National Cancer Institute, and Menarini Silicon Biosystems, the maker of the CTC assay used in the trial. The investigators disclosed relationships with Menarini and many other companies. Dr. Ballinger receives honoraria from Medscape, which is owned by the same company as this news organization.
SOURCE: Bidard FC et al. JAMA Oncol. 2020 Nov 5. doi: 10.1001/jamaoncol.2020.5660.
FROM JAMA ONCOLOGY